Common conditions
26 December 2020
22:57
Common Procedures and examples
A patient undergoing an
orthopaedic procedure
Arthroscopy
Joint replacement
A patient undergoing an
abdominal/gastrointestinal tract procedure
Cholecystectomy
Hernia repair
Colonoscopy
Colectomy
A patient undergoing a breast
procedure
Lumpectomy
Mastectomy
A patient undergoing an opthalmic
procedure
Cataract surgery
A patient undergoing a urological
procedure
Cystoscopy
Common Conditions and Examples
A patient with cancer
Colorectal cancer
Breast cancer
Lung cancer
Prostate cancer
A patient with musculoskeletal
disease
Osteoarthritis
Rheumatoid arthritis
Neck or back pain
Osteoporosis
A patient with chronic kidney
disease
A patient with diabetes mellitus
A patient with lung disease
Chronic obstructive pulmonary
disease
Asthma
A patient with chronic liver
disease
Alcoholic liver disease
Nonalcoholic steatohepatitis
Chronic viral hepatitis
A patient with hearing loss
Presbyacusis
A patient with visual loss
Macular degeneration
Glaucoma
Cataract
A patient with vascular disease
Hypertension
Ischaemic heart disease
Heart failure
A patient with skin disease
Eczema
Psoriasis
Acne
A patient with chronic
neurological disease
Epilepsy
Stroke
Migraine
A patient with persistent
unexplained physical symptoms
Stroke
24 December 2020
23:10
The clinical features of stroke
are of a “sudden onset of focal or global cerebral dysfunction due to a
vascular cause”.
“a sudden onset of focal or global cerebral
dysfunction, persisting for more than 24 hours, for which the cause is
vascular”
It includes cerebral infarction,
intracerebral haemorrhage and subarachnoid haemorrhage
|
|
LACI |
TACI |
PACI |
POCI |
|
30
days |
|
|
|
|
|
Dead |
2% |
39% |
4% |
7% |
|
Dependent |
36% |
56% |
39% |
31% |
|
Independent |
62% |
4% |
56% |
62% |
|
1
Year |
|
|
|
|
|
Dead |
11% |
60% |
16% |
19% |
|
Dependent |
28% |
36% |
29% |
19% |
|
Independent |
60% |
4% |
55% |
62% |
From <https://mle.ncl.ac.uk/cases/page/8650/>
Antiplatelet-
These reduce the risk of further ischaemic
stroke (and of myocardial infarction and other vascular events) by a relative
risk reduction of 20-30%. In absolute
terms that means a reduction of risk of about 1% over the first month, 2-3 %
over the first year, and 1% per year thereafter.
They work by interfering in
platelet function and therefore reducing the risk that unstable atherosclerotic
plaque will cause an occlusive thrombus or embolus.
The most commonly used after
stroke would include aspirin (used in a 300mg or 75 mg daily dose predominantly
in the first fortnight after stroke where the evidence is strongest for it’s
effect) or clopidogrel (which appears to be more effective in longer term
prevention and is used at a 75mg daily dose).
An inevitable consequence of
reducing blood clotting capacity is to increase the risk of bleeding. Many patients have minor bleeding or easy
bruising as a result of these medications.
More rarely serious bleeding will be caused or significantly exacerbated
(in 1-2% of patients per year). Serious
bleeding is more common in patients who have a recent history of bleeding from
for example a peptic ulcer. For patients
over 50 it is usually recommended that a proton pump inhibitor (PPI) be
prescribed at the same time to reduce the risk of bleeding from peptic ulcers –
but that obviously exposes the patient to the risk of further side effects
(e.g. diarrhoea) from the PPI.
Statins-
These also reduce the risk of
further ischaemic stroke (and of myocardial infarction and other vascular
events) by a relative risk reduction of 20-30%.
In absolute terms that means a reduction of risk of about 1% over the
first month, 2-3 % over the first year, and 1% per year thereafter. This risk reduction holds regardless of the
patients’ actual cholesterol level – risk is reduced even in patients with
relatively low cholesterol levels at the time of stroke. Likewise there is no specific cholesterol
target to be aimed for – just being on the drugs appears to be effective.
The strongest evidence is for
high potency statins at maximal doses – particularly for atorvastatin at 80 mg
per day. The evidence for effectiveness
for other “cholesterol lowering” drugs is poor and they are not recommended.
Around 10% of patients started on
statin treatments will develop unpleasant usually localised muscle aches. This is probably more common in patients with
lower muscle mass – but is largely unpredictable. Happily this side effect almost always
resolves promptly with reducing the dose of the statin, changing to a statin
with a different mode of action (pravastatin or rosuvastatin) or stopping
treatment. There is a much smaller risk
of severe muscle problems (myositis) which also present with muscle pain, but
where there is associated muscle damage evidenced by a raised serum creatine
kinase level) or of hepatotoxicity. NICE
guidelines suggest checking cholesterol levels 2-3 months after starting statin
treatment (these should drop by at least 20-30% over this time, and if they
don’t then the patient may not be taking or absorbing the tablets for some
reason), along with liver function tests to detect hepatotoxicity. Minor rises in the liver enzyme ALT are
common, and only rises to 3 times the upper limit of normal are considered a
reason to stop therapy.
Anti hypertensive-
Unlike statin therapy, where
there is no threshold level where treatment should start and no target to
achieve, treatment for hypertension is target driven. Optimal reduction in the risk of further
events – and this holds for intracerebral haemorrhage as well as for cerebral
infarction – is achieved with reduction of blood pressure to levels
consistently lower than 130/80.
Antihypertensive therapy is the only treatment that reduces the long
term risk of recurrent intracerebral haemorrhage – antiplatelet agents and
statins are not effective, and may slightly increase risk.
Achieving this blood pressure
again reduces the risk of further events by 20-30% in relative risk reduction
terms, and in absolute terms this equates to a long-term risk reduction of
around 1% per year.
There are many drugs that can be
used to achieve this. Clinicians usually
follow the NICE recommendations for choice of antihypertensive therapy
(referenced in Case 1 in years ½ MBBS).
Each drug has specific potential
side effects (e.g. persistent dry cough with angiotensin converting enzyme
(ACE) inhibitors). All have the frequent
side effect of causing or exacerbating orthostatic hypotension and therefore of
making patients feel dizzy or light headed, potentially causing syncope and
falls.
Anticoagulants-
Anticoagulants (e.g. warfarin or
direct oral anticoagulants like apixaban) have a specific role in reducing the
risk of ischaemic stroke in patients with atrial fibrillation, which could be
either permanent or paroxysmal. In this
specific situation the risk of recurrent ischaemic stroke is much higher than in
other patients with stroke (probably 15-20% in the first year and persisting at
greater than 10% per annum long term).
Strokes in the context of atrial
fibrillation have an additional potential mechanism, as they can arise from
emboli of thrombin rich thrombus which form in the left atrium of the
heart. The risk of forming these
thrombin rich (red) thrombi is greatly reduced by anticoagulant drugs (but not
by antiplatelet drugs).
For these patients anticoagulant
drugs reduce risk of stroke by a relative risk reduction of 60-70%. In absolute terms this equates to a risk
reduction of more than 10% in the first year and 7-8% every year thereafter.
These drugs also carry an
inevitable risk of causing serious bleeding complications which is probably around
3-4 % per year, and minor bleeding problems with bruising are very common. Bleeding complications, and particularly
intracranial bleeding complications, are significantly less frequent with the
direct oral anticoagulants than with warfarin.
Warfarin also has a disadvantage
compared with the direct oral anticoagulants in that the required dose varies
between people and over time, so that frequent (usually monthly) blood tests
and dose adjustments are necessary to maintain anticoagulation at levels that
are high enough to be effective but not so high as to further increase bleeding
risk. It has a modest advantage over the
direct agents in that warfarin is easily reversible with intravenous clotting
factors should serious bleeding occur, whilst direct anticoagulants are not
reliably reversible. It’s worth pointing
out that despite this the risk of serious bleeding is higher with warfarin.
Decision making around starting
anticoagulants in atrial fibrillation is an area which has been studied
extensively. There are many decision
aids to support this. These include
scores to estimate the risk of stroke in individual patients (e.g. the
CHADS2VASC score) and to estimate an individual patients risk of bleeding side
effects (e.g. HASBLED score). They also
include many videos and written materials including pictorial aids to help
clinicians explain these risks to their patients. It is one of the areas where shared decision
making has been most frequently used, and it would be worth your while to spend
some time considering how you might discuss these risks and benefits in a
clinical consultation.
It’s fair to say that as
anticoagulation has become safer the balance of risks even for primary
prevention of stroke is almost always in favour of anticoagulant drugs, and in
secondary prevention (where the stroke risk and the effectiveness of treatment
is higher) there are very few situations where the hard logic of statistical
risk/benefit balance would not strongly suggest using anticoagulants.
Carotid Endarterectomy-
In terms of reducing the risk of
further ischaemic stroke, there is good evidence that carotid endarterectomy
reduces the long term risk of recurrent stroke in patients who have a >50%
stenosis in the internal carotid artery on the same side as they had their
stroke. The effectiveness of this
treatment declines rapidly with time – so that by a point 3 months after stroke
the risks of the procedure almost balance those of avoiding treatment. The treatment has only been studied in
patients who have made a good recovery with minimal persistent deficit after
stroke (practically defined as being able to walk independently into the
outpatient consulting room and have a reasonable discussion with the vascular
surgery team).
The benefit of surgery increases
with the severity of carotid stenosis.
In those with 70-99% stenosis, endarterectomy reduced the risk of stroke
by an absolute 15% over 5 years. In
those with 50-60% stenosis the risk was reduced by 5% at 5 years. These reported benefits may be overestimates
as trials of surgery took place compared with standard treatment that at that
time did not include modern antiplatelet drugs or statins. Further it takes 6 months to a year for the
benefit of surgery to become apparent, because although the long term risk of
stroke is reduced, the operation itself causes a 3-4% additional risk of stroke
at the time of operation or within 30 days.
For patients with a lower life
expectancy (older patients or those with comorbidities) the potential for
benefit is lower as this only accrues many months after operation. Even if their life expectancy is longer most
people value their current health (and wealth) much more highly than their
health in the future (economists term this “discounting”), so for many patients
the prospect of increasing their immediate risk of stroke outweighs the
potential longer term benefits when considering operation. This effect is probably magnified by a
perhaps illogical but certainly real human perception that if they had a stroke
as a result of operation then this would be an unnatural event that they
precipitated – whereas a stroke occurring without operation would feel more
like an act of fate beyond their control and be more bearable as a result.
There are several risk and
benefit calculation tools that can help in supporting patients with these
decisions including one from the Department of Clinical Neuroscience in Oxford https://www.ndcn.ox.ac.uk/divisions/cpsd/carotid-stenosis-tool.
Migraines
26 December 2020
19:08
Commonly reported features of
migrainous aura include:
Visual disturbances e.g. blind
spots (scotoma), 'zig zags' (fortification spectra)
Numbness and tingling
Difficulty talking (aphasia)
Balance problems
And, very rarely, motor weakness
The frequency of migraine can
vary from every few months to daily
headaches. The severity may also fluctuate with 'typical' migraine headaches
that are worse than usual or better than usual.
Chronic
Migraine
Patients
with previously sporadic or regular but infrequent migraines can convert into
chronic migraine which is defined by headaches that occur at least 15 days out
of the month, where 8 of these 15 headaches are migrainous in nature.
From <https://mle.ncl.ac.uk/cases/page/8744/>
Status
Migrainosus
Status
migrainosus describes migraine attacks that are more severe and more prolonged
than a patients typical episodes. This is often defined as >72 hours in
duration.
These
severe episodes can be reduced by good acute management of migraine in the
earlier stages of an attack. They are however also associated with
overuse of medication.
From <https://mle.ncl.ac.uk/cases/page/8744/>
Medication
Overuse Headache
We
considered Medication Overuse Headache as a differential diagnosis for
migraine, but it is also a potential complication and consequence of migraine.
Recap:
Headaches associated with the overuse of certain medications.
Defined
as:
·
Present 15 or more
days per month
·
Developed or worsened
during medication overuse
·
Resolves or reverts to
previous pattern within two months of discontinuing medication overuse
·
Regular use for 3
months or more of one of the following drugs for headache:
·
Triptans, opioids,
ergots or combinations of these on 10 or more days per month
·
Paracetamol, aspirin,
NSAIDs or combinations or combinations of these on 15 or more days per month.
From <https://mle.ncl.ac.uk/cases/page/8744/>
Migrainous
Infarction
Migrainous
infarction is a rare complication where a migraine attack is associated with a
neurological lesion on imaging.
Features
of migrainous infarction are:
1.
One or more features
of migraine aura
2.
Migraine aura must be
typical of previous attacks
3.
Ischaemic brain
lesions demonstrated
4.
Focal neurological
deficit(s) must persist longer than 60 minutes
5.
Episode must be
associated with a pain crisis
From <https://mle.ncl.ac.uk/cases/page/8744/>
Acute
Management
The aim of acute management is the termination or
significant relief of the symptoms of migraine. These include pain, nausea and
vomiting. When considering acute management, factors such as the reliability of
the patient keeping medication down due to vomiting is important.
Acute
management should be taken at the start of headache whilst the pain is mild.
Simple
analgesia
Ibruprofen
Aspirin
Paracetamol
Triptans
5HT
agonists
Oral
preparations
Intranasal
or subcutaneous preparations can be used if vomitus prevents oral preparations
Patients
should be advised to only take triptans at the start of the headache not the
start of the aura.
Anti-Emetic
medications
Metoclopramide
Prochloperazine
All
patients should be followed up to track the effectiveness of acute management
and escalate if necessary.
Prophylaxis
For
many patients migraine is an intermittent problem, best managed acutely when it
arises. For others however migraine is so frequent, severe and disruptive
that they would consider daily medication to prevent attacks.
Prophylactic
treatment for migraine should be considered in the following circumstances:
·
Significant impact on
the patients quality of life and daily function
·
Frequent occurrence
·
Prolonged or severe
despite optimum acute management
·
Acute treatments are
contraindicated or ineffective
·
Patient is at high
risk of medication overuse due to frequent use of acute medication.
Pharmacological
Options
·
Propranolol
·
Topiramate
·
Amitriptyline
·
Botulinium A toxin
injections (where 3 prophylactic agents have failed)
Other options
·
Cognitive behavioural
therapy
·
Mindfulness therapy
·
Acupuncture - 10
sessions over 5-8 weeks
·
Riboflavin
supplementation - 400mg once daily
Follow
up for patients on prophylaxis:
Patients
should be advised to keep a headache diary where they track the incidence and
severity of their headaches. This allows both the patient and the clinician to
track the effectiveness of therapy and titrate medication as needed.
Patients
also need to be reviewed often during the titration process (2-3 weeks) for
side effects. Once on stable treatment patients can be reviewed every 6-12
months.
Patients
should be counselled that migraine relief on prophylaxis often takes 4-8 weeks
from the onset of treatment. This is to manage expectations.
Failure
to respond to max tolerated dose of prophylaxis for 3 months is a failure of
treatment and these patients should be referred to neurology.
From <https://mle.ncl.ac.uk/cases/page/9322/>
Interventional
Treatments
The
intention for all of these is relief but not cure of migraine
Transcutaneous
electrical stimulation of supra-orbital nerve
Involves
wearing a headband that uses small currents to stimulate the nerves of the
forehead to reduce pain. Has also been shown to reduce migraine. Indications: Distressing
symptoms where medical therapy has failed.
Transcutaneous
stimulation of the cervical branch of vagus nerve
Involves
using a small handheld device to deliver low voltage currents to stimulate the
cervical branch of vagus nerve. The aim is to relieve pain and reduce the
frequency of episodic headaches. It can be used for cluster headache and
migraine that are distressing where medical treatment has failed.
Transcranial
magnetic stimulation
Involves
placing a device on the scalp and delivering single or repeated magnetic
pulses.
Percutaneous
closure of the foramen ovale
Involves
closure of an abnormal remnant of the fetal heart where there is a persistent
communication between the left and right atrium. This has been shown in some
patients to be a cause of recurrent migraine.
Occipital
nerve stimulation
Involves
implanting electrodes to deliver electrical impulses to the occipital nerve to
mask migraine pain.
From <https://mle.ncl.ac.uk/cases/page/9325/>
Other
options in migraine
In
addition to clinician-led management, there are several self management
strategies that patients can employ themselves that may improve symptoms.
Nutrition
Regular
meals seem to reduce the frequency and severity of migraine attacks. Common
food triggers for migraine include caffeine, chocolate and alcohol.
Triggers
vary greatly between patients however, so there is no single dietary regime
that will apply to all patients. Patients can use their headache diaries
to attempt to identify and restrict any additional dietary factors that may
trigger headaches.
Specific
Diets
Whilst
regular meals are generally agreed to be preventative of migraine, there is
relatively little high quality evidence that specific diets consistently
improve the frequency and severity of migraine.
Ketogenic
diet: Involves restriction of carbohydrate
and sugar with dietary emphasis on protein and fat intake. The notion is to
enter a state of ketosis.
Low
glycaemic index diet: Involves
switching to consumption of low glycaemic index foods, which are metabolised
over a longer period of time and cause slower rises in blood sugar rather than
causing peaks and troughs in blood sugar. The notion is to maintain blood
glucose at a relative steady state.
Stress
Management
Psychological
stressors can trigger migraine. Avoiding or minimising stressful
situations and practicing effective stress management can reduce
migraine.
It's
worth considering that migraine (and it's effect on relationships and work for
example) can cause stress, producing a vicious cycle.
Sleep Quality and Hygiene
Disordered
sleep is a common trigger for migraine. Many patients find they can
reduce attacks by improving their sleep quality and hygiene; aiming to sleep at
the same time each night, followed by a predictable period of sleep and a
predictable waking time.
Disturbed
sleep may also be a consequence of prolonged severe migraine, either directly,
or because of associated stress. Again, breaking this cycle may lead to
significant benefits.
From <https://mle.ncl.ac.uk/cases/page/9324/>
NICE
would recommend escalating to use of a triptan if ibuprofen or paracetamol or
aspirin ineffecdtive.
·
Depending on the
severity of attacks, associated symptoms, contraindications and comorbidities:
o Offer simple analgesia such as:
·
Ibuprofen (400mg) — if
ineffective, consider increasing to 600 mg or
·
Aspirin (900
mg) or
·
Paracetamol (1000mg).
o Offer a triptan, alone or in combination with,
paracetamol or an NSAID:
·
Oral sumatriptan
(50–100 mg) is first choice — other triptans should be offered if sumatriptan
fails.
·
If vomiting restricts
oral treatment, consider a non-oral formulation (such as intra-nasal or
subcutaneous).
o Consider offering an anti-emetic (such as
metoclopramide 10mg or prochlorperazine 10mg) in addition to other acute
medication even in the absence of nausea and vomiting.
·
Metoclopramide should
not be used regularly due to the risk of extrapyramidal side effects.
·
Advise the person
that:
o Acute medication should be taken early while
pain is mild.
o If they have aura, triptans should be taken at
the start of the headache and not at the start of the aura (unless
the aura and headache start simultaneously).
·
Do NOT offer ergots or
opioids.
From <https://mle.ncl.ac.uk/cases/page/9342/>
2)
NICE guidelines state that topiramate, propranolol and amitriptyline are
indicated for medical prophylaxis of migraine. Riboflavin supplementation and
acupuncture can also be used as preventative measures.
From <https://mle.ncl.ac.uk/cases/page/9342/>
3)
Topiramate should not be used in pregnancy as it is actively teratogenic.
Propranolol and Amitriptyline are considered safer if prophylaxis is a
requirement. Seek specialist advice if unsure.
teratogenic
effects of beta blockers (propranolol) and anti-epileptics (topiromate) and the
implications if she were to fall pregnant.
prophylaxis
in this instance as his migraines as:
·
Significant impact on
quality of life and daily function (this is subjective)
·
Prolonged or severe
despite optimum acute management
Back and Neck pain
26 December 2020
21:58
red flag symptoms of back pain
T Trauma
U Unexplained weight loss
N Neurologic symptoms
A Age >50
F Fever
I IV drug use
S Steroid use
H History of cancer
·
Cauda
equina syndrome (CES). Red flags include:
o Severe or progressive bilateral neurological
deficit of the legs (such as major motor weakness with knee extension, ankle
eversion, or foot dorsiflexion.
o Recent-onset urinary retention and/or urinary
incontinence
o Recent-onset faecal incontinence
o Perianal or perineal sensory loss (saddle
anaesthesia or paraesthesia)
o Unexpected laxity of the anal sphincter.
·
Spinal
fracture. Red flags include:
o Sudden onset of severe central spinal pain
which is relieved by lying down.
o A history of major trauma (such as road
traffic collision or fall from a height), minor trauma, or even just strenuous
lifting in people with osteoporosis or those who are taking corticosteroids.
o Structural deformity of the spine
o There may be point tenderness over a vertebral
body.
·
Cancer. Red flags include:
o The person being over 50 years of age.
o Gradual onset of symptoms
o Severe unremitting pain that remains when the
person is supine
o Aching night pain that prevents or disturbs
sleep
o Pain aggravated by straining
o Thoracic pain
o Localised spinal tenderness
o No symptomatic improvement after 4-6 weeks of
conservative low back pain therapy.
o Unexplained weight loss.
o Past history of cancer – breast, lung,
gastrointestinal, prostate, renal, and thyroid cancers are more likely to
metastasise to the spine.
o Back pain could also point towards multiple
myeloma, or lymphoma.
·
Infection (such as discitis, vertebral osteomyelitis, or
spinal epidural abscess). Red flags include:
o Fever
o Tuberculosis, or recent urinary tract
infection
o Diabetes
o History of IV drug use
o Immunocompromised patients (for example due to
HIV infection, or the use of immunosuppressants).
This
list isn’t inclusive. There are other serious causes of back pain that aren’t
related to the spine, such as an Abdominal Aortic Aneurysm (Triple A) rupture,
or pathology in the kidneys.
From <https://mle.ncl.ac.uk/cases/page/9879/>

NICE
suggests should be done:
·
If there are red flag
symptoms and signs that may suggest a serious underlying cause, admit of refer
urgently for specialist assessment, or imaging, using clinical judgement.
·
If an underlying cause
for the low back pain has been identified, manage according to the specific
diagnosis.
From <https://mle.ncl.ac.uk/cases/page/9888/>
Yellow Flag Symptoms
There
will be psychosocial barriers to active rehabilitation, and these should be
spotted to reduce the risk of chronicity.
These
barriers are called “Yellow Flags”. They include:
·
Sickness behaviours,
such as extended rest.
·
Belief that pain and
activity are harmful
·
Social withdrawal
·
Emotional problems
such as low mood, depression, anxiety, and stress.
·
Problems and/or
dissatisfaction at work
·
Problems with claims
or compensation, or time off work
·
Overprotective or
unsupportive family/friends.
·
Inappropriate
expectations or engagement in treatment
From <https://mle.ncl.ac.uk/cases/page/9905/>
Risk
stratification tools such as STarT Back are a useful way of stratifying patient’s risk of a
poor prognosis, and matching the treatment option that is best for them.
Testing
for the presence of Waddell’s signs is also a suggested method of
identifying whether there are non-organic or psychological components to the
patient’s pain.
From <https://mle.ncl.ac.uk/cases/page/9905/>
Management of Non-Specific Lower Back Pain
Since
non-specific low back pain does not have a known patho-anatomical cause,
treatment focuses on reducing pain and its consequences.
Here
are a few tips:
·
Give information,
reassurance and advice.
·
Address issues that
may predispose to further episodes (yellow flags).
·
Do not prescribe bed
rest – advise the patient to stay as active as possible.
·
Consider regular pain
relief; lowest dose, short course of non-steroidal anti-inflammatory drugs.
Consider also a short course of muscle relaxants.
·
Only offer weak
opioids if non-steroidal anti-inflammatories are ineffective, contraindicated,
or not tolerated.
·
Paracetamol
mono-therapy has been shown to be ineffective, contraindicated or not
tolerated.
Pain Management Services
·
Multidisciplinary
approaches by Pain Management teams are an invaluable service aimed at
providing individualised care packages to help people live with their chronic
pain.
·
Referral should be
considered if not resuming normal activities or off work.
·
The Living Well
with Pain Team provide this service in the Northumbria Trust.
o GPs or advanced practitioner physiotherapists
from the area can make referrals.
o The team offers workshops on pain management,
psychological therapy, and physiotherapy.
·
If you’re interested,
you can find out more information about the team here: https://www.northumbria.nhs.uk/our-services/living-well-with-pain/

From <https://mle.ncl

.ac.uk/cases/page/9906/>
Rheumatoid Arthritis
26 December 2020
22:15
·
Boutonniere
deformity. There is DIP hyperextension and PIP flexion
·
swan neck deformity. There is DIP flexion and PIP
hyperextension
·
Z thumb
deformity or sometimes called Hitchhiker's thumb.
·
There is hyperextension of the interphalangeal joint,
and fixed flexion and subluxation of the metacarpophalangeal joint.
·
Ulnar deviation
Rheumatoid Arthritis
in a nutshell...
· RA is the commonest cause of
chronic inflammatory arthritis in the UK. It is much less common in Malaysia
and in this context the main differential diagnosis is Systemic Lupus
Erythematosus (SLE).
· Clinical features include joint
pain, joint swelling, morning stiffness, difficulty in moving and ability to
perform motor tasks. The presentations however can be variable and patients
often describe a fluctuation in symptoms from day to day and week to week.
There is often a chronic relapsing / remitting course which may be progressive
and indolent but acute presentations occur. There are often systemic symptoms –
again variable – including fatigue, loss of energy and even weight loss.
· The differential diagnosis is
wide and includes other causes of inflammatory arthritis (including SLE and
other connective tissue diseases), infection related arthritis, crystal
arthritis, hypothyroidism, and malignancy.
· The clinical assessment is most
important in making a diagnosis – taking an MSK history and performing a competent
joint examination are essential. The diagnosis of RA is essentially clinical
with investigations to exclude differential diagnoses. Radiographs can be
normal in early RA. US is a highly sensitive way to detect synovitis.
Rheumatoid factor can be negative in RA. Anti CCP antibodies are highly
specific for RA.
· RA can have a dramatic impact
on activities of daily living and the variability in symptoms make it difficult
to plan ahead.
· Being able to stay in work is
important to maintain an income and concern about work is often a cause of
anxiety.
· The approach to management of
RA includes medical and biopsychosocial aspects. The multidisciplinary team
(MDT) is essential and includes the nurse, allied health (physiotherapy and
occupational therapy).
· Management of RA includes
pharmacologic and non-pharmacologic options.
· The aim of management is to
achieve disease control as soon as possible, mitigate / avoid side effects of
treatment, optimise function and enable patients to lead a fulfilling
independent life.
· The medical management includes
treatment to manage symptoms, prevent joint damage and disability, and prevent
/ reduce the risk of complications of the disease and or side effects of
treatment.
· The emphasis is on early
diagnosis and prompt access to immunosuppressive treatments with escalation of
treatment to achieve rapid disease control.
· Early remission is the goal of
management and is achievable for many patients although patients have to take
treatments long term - a curative treatment is not currently available.
· Early RA clinics aim for all
suspected RA patients to have a prompt first assessment and access to highly
effective treatment options that are now available has led to clinical outcomes
being much improved.
· Comorbidities are common in
patients with RA and may influence the treatment options. Increased mortality
is reported in RA. The main cause of death is cardiovascular disease.
· RA is a serious disease and
prior to the emergence of highly effective DMARDS and biologics, high morbidity
with disability was common along with marked increased mortality from
cardiovascular disease in particular. The outcome has markedly improved in
recent decades.
Differentials
The differential diagnosis must
include other causes of inflammatory arthritis (including SLE and other
connective tissue diseases), infection related arthritis, crystal arthritis,
hypothyroidism, and malignancy. This list is not exhaustive.
The clinical assessment is most
important in making a diagnosis – taking an MSK history to come up with a
differential diagnosis and performing a competent joint examination is
essential.

Investigations
The
diagnosis of RA is essentially clinical with investigations to exclude
differential diagnoses.
1.
Bedside
·
Urinalysis as a baseline
and to exclude other differentials.
2.
Bloods - baseline before treatment and to exclude other differentials.
·
FBC, ESR, CRP,
U&Es, LFTs, Autoantibodies (including Rheumatoid factor / anti-CCP), TFTs.
Other
tests depending on the presentation to exclude other differentials. Remember
that Rheumatoid factor (RF) may be negative in RA and also a positive RF is not
diagnostic of RA. Anti CCP antibodies are highly specific for RA. Positive RF
and anti-CCP antibodies are prognostic indicators of a more severe course in
the context of a diagnosis of RA.
3.
Imaging - as a baseline before treatment and to exclude other differentials.
·
US joints are the most
sensitive imaging modality to detect synovitis.
·
Joint radiographs
helpful as a baseline and to exclude other differentials but are often normal
in early RA.
·
Chest XR - helpful as
a baseline (prior to starting methotrexate or other treatments) and to
exclude other differentials including latent TB.
4.
Special tests
·
Blood tests – latent
TB, Hep B, Hep C, HIV status (pending clinical context) – before starting
immunosuppressives.
·
Lung Function -
helpful as a baseline (prior to starting methotrexate or other treatments)
·
Synovial fluid
assessment – joint aspiration is essential to exclude septic arthritis and
crystal arthropathies
Risks
of investigations:
There
are no particular risks of the investigations although joint aspiration must be
done using sterile technique and by a competent operator. The blood tests may
be negative or normal so can be falsely reassuring – for example RF can be
negative in RA
From <https://mle.ncl.ac.uk/cases/page/13278/>
Patients suspected to have RA
should be referred to a rheumatologist as soon as possible to confirm the
diagnosis, establish the severity of the disease and develop a care plan. Early
referral and ongoing rheumatology input has bee shown to improve disease outcomes.
A
combination of therapies is used:
1.
Anti- inflammatory medication ( e.g NSAIDs and systemic/intraarticular
glucocortoids)
These
medications are used to temporarily control the disease in patients commencing
DMARDs or during disease flares. They are useful at reducing inflammation but
do not provide long term control or prevent joint injury. Glucocorticoids are
often not used for long periods of time due to their side effects.
2.
Disease Modifying Anti-rheumatic Drug (DMARDs)
These
include nonbiological and biological DMARDs which can reduce or prevent joint
damage and preserve function. Patients should therefore be started on DMARDs as
soon as possible.
Examples
of nonbiological DMARDs include Methotrexate, hydroxychloroquine and
sulfasalazine.
Biological
DMARDs work by targeting cytokines or their receptors. They can therefore be
subclassifed into TNF-alpha inhibitors e.g infliximab, adalimumab; IL-1
receptor antagonists e.g anakinra and IL-6 receptor antagonists e.g
tocilizumab etc.
Typically
patients are commended on Methotrexate first line.
Patients
unable to take methotrexate will require an alternative such as
hydroxychloroquine or sulfasalazine.
If
patients are resistant to initial DMARD therapy then a combination of DMARDs
can be used e.g methotrexate +TNF inhibitor.
From <https://mle.ncl.ac.uk/cases/page/13281/>
1. Pregnancy/ women of child
bearing age- methotrexate is teratogenic. If used in women of child bearing age
effective contraception should be used and continued for 6 months after
treatment. Hepatic impairment
The emphasis is on early
diagnosis and access to immunosuppressive treatments with escalation of
treatment to achieve rapid disease control (so called ‘treat to target’).
Regular monitoring patient is important to assess the response to treatment and
any side effects.
Disease activity and severity is
assessed clinically (history and examination), bloods tests (acute phase
reactants) and imaging of joints (usually by US). There are various outcome
measures and the Disease Activity Score (DAS28) is a composite score to assess
indication and response to biologics. Patient Reported outcomes measures
(PROMS) are important and relate to the impact on the individual. Active
RA and systemic effects are usually
easily recognized by the presence of actively inflamed joints, fever, anaemia,
an elevated erythrocyte sedimentation rate (ESR), or an elevated serum
C-reactive protein (CRP).
The management of RA is complex and
the MDT approach is important to enable patients to understand the rationale
for treatments and make appropriate choice for them. A shared decision making
approach is important.
Non-pharmacologic options.
Briefly, these measures include:
●Patient education
●Psychosocial interventions
●Rest, exercise, and physical and
occupational therapy
●Nutritional and dietary
counselling
●Interventions to reduce risks of
cardiovascular disease, including smoking cessation and lipid control
●Screening for and treatment of
osteoporosis
●Immunizations to decrease risk
of infectious complications of immunosuppressive therapies.

Joint failure
Patients with RA are at risk of
secondary osteoarthritis even with therapeutic interventions. Some patients
progress to disabling, destructive joint disease. Patients may present with
mechanical symptoms (pain on weight bearing and walking) and in the case of
knee or ankle involvement, with locking and or giving way. The accurate
evaluation of such patients is essential, since deterioration associated with
mechanical problems of the muscle or joint is treated much differently from
ongoing inflammation or systemic manifestations of rheumatoid arthritis
(RA). Osteoporosis can lead to avascular
necrosis of the hip and secondary osteoarthritis.
The goals of therapy in the
patient with end-stage disease are:
●Pain relief
●Protection of remaining
articular structures
●Maintenance of function
●Relief from fatigue and weakness
The indications for surgical
intervention in patients with RA include severe pain or functional disability
due to joint destruction. The timing of surgery is important - waiting too long has the risk of much muscle
atrophy from disuse resulting in postoperative rehabilitation being
unsuccessful.
Treatment
during pregnacy:
-
Pre-conception counselling should be offered involving a rheumatologist and
obstetrician.
-
Ideally pregnancy should be planned for when their disease is under good
control on medications compatible with pregnancy e.g TNF inhibitors,
sulfasalazine
-Commence
folic acid prior to pregnancy
- If RA
becomes active in pregnancy, NSAIDs can be used until the 3rd trimester or low
dose prednisolone. Or the patient can be commenced on a safe DMARD.
From <https://mle.ncl.ac.uk/cases/page/13294/>
Infection
●Serious infection – In patients
with an active serious infection, conventional and biologic disease-modifying
antirheumatic drugs (DMARDs) and tofacitinib should be temporarily held until
resolution of infection and completion of antimicrobial therapy. In patients
with a history of a serious infection, we recommend conventional DMARDs over
biologic agents. Medications administered more frequently are preferred in
patients in whom there is heightened concern regarding infection or with
recurrent infections because of the relative greater ease of discontinuing the
therapy and its immunomodulatory effect if needed.
●Hepatitis B – In patients with
natural immunity to hepatitis B virus (HBV; HBV core antibody [HBc]-positive,
normal liver chemistries, HBV surface antibody [HBs]-positive, and HBV surface
antigen [HBsAg]-negative), treatment for RA should be the same as for
HBV-unexposed RA patients, but viral loads should be monitored every 6 to 12
months to ensure there is no reactivation. For patients with active untreated
hepatitis, referral for antiviral therapy should be obtained before
immunosuppressive therapy, and patients should be treated in collaboration with
their hepatologist. In the absence of additional harms, RA treatment may
proceed for patients with active HBV on concomitant antiviral treatment. (See
"Hepatitis B virus: Screening and diagnosis" and "Hepatitis B
virus: Overview of management".)
●Hepatitis C – Patients with
active hepatitis C virus (HCV) and normal liver function should not be treated
differently than RA patients without HCV. If underlying liver disease is
present, non-hepatotoxic DMARDs (sulfasalazine [SSZ] or hydroxychloroquine
[HCQ]) are preferred initially. Patients with HCV infection should be managed
in collaboration with their hepatologist. (See "Overview of the management
of chronic hepatitis C virus infection".)
●Tuberculosis – Prior to
initiation of immunomodulatory therapy, patients with risk factors for
tuberculosis (TB) should be screened for latent TB and treated if indicated
(see 'Pre-treatment evaluation' above). In patients in whom latent TB is
diagnosed, at least one month of treatment should be completed prior to the
initiation of immunosuppressive agents.
In patients with latent TB who
are unable to complete anti-TB therapy, we prefer to use nonbiologic DMARDs as
monotherapy or in combinations. In patients with persistent disease activity
despite such intervention, it may be necessary to use a biologic DMARD, in
which case we prefer agents other than tumour necrosis factor (TNF) inhibitors.
We also review the risks of such intervention in detail with the patient when
deciding upon therapy and consult with a specialist in infectious disease for
additional assistance in management.
Malignancy
Management of RA in patients with
malignancy or a history of malignancy is based upon findings from observational
studies including registries together with expert opinion.
●Non-melanoma skin cancer (basal
cell and squamous cell carcinoma) – In patients with a history of non-melanoma
skin cancer, conventional DMARDs are preferred over biologic DMARDs or
tofacitinib. There is no contraindication to escalation of therapy to include
biologics, but routine skin cancer surveillance is indicated.
●Melanoma skin cancer – In
patients with a history of melanoma conventional DMARDs are preferred over
biologic DMARDs or tofacitinib. Approaches including monoclonal antibody
treatments that activate T cells have shown benefit in treating melanoma;
therefore, some clinicians avoid the use of abatacept in patients with a prior
history of melanoma. Routine skin cancer surveillance is indicated.
●History of lymphoproliferative
disorder – In patients with a history of a lymphoproliferative disorder, we
prefer conventional DMARDs, and if a biologic agent is needed, the first choice
would be rituximab, given its use in the treatment of lymphoproliferative
disorders and a lack of evidence for increased cancer risk with its use.
●Solid organ malignancy – In
patients with a treated solid organ malignancy within the past five years, we
use conventional DMARDs over biologic DMARDs. If a biologic agent is needed,
the first choice would be rituximab, given the lack of evidence for increased
cancer risk with its use. In patients who are more than five years out from a
treated solid organ malignancy, excluding melanoma, RA treatment is no
different than from those without malignancy.
Lung disease - Comorbid pulmonary
disease is common in patients with RA and may also be a complication of therapy
or of the disease; adverse effects from methotrexate include a pneumonitis
especially in smokers. There is an increased risk of opportunistic infection
including TB with immunosuppressive treatments.
Diabetes — in patients with both
diabetes and RA, glucocorticoids should be used with particular caution because
they may worsen control of the diabetes.
Infections - Covid-19 pandemic
and implications for patients on immunosuppressive treatment – new guidance is
available
https://www.nice.org.uk/guidance/ng167.
Vaccines – vaccines are
encouraged although live vaccines are contra-indicated. Annual influenza
vaccine is recommended.
Osteoporosis – patients with RA
are at risk of osteoporosis for a number of reasons – chronic inflammation,
less weight bearing and systemic use of glucocorticoids are risk factors. Good
disease control, weight bearing exercise and diet supplementation with calcium
and vitamin D are important.
Increased mortality is reported
in RA. The main cause of death is cardiovascular disease. The increased risk of
cardiovascular disease is multi-factorial and control of chronic inflammation
is key as it may lead to the development of atherosclerosis. Medications used
to treat RA such as steroids and NSAIDs can also increase the risk of CVD.
The
QRISK assessment (a prediction algorithm for CVD) includes RA as a risk
factor. An important aspect of management of RA therefore is to establish and
manage cardiovascular risk (control of BP, lipids) and lifestyle factors
(smoking, diet and exercise) also need to be addressed.
From <https://mle.ncl.ac.uk/cases/page/13291/>
Some patients may develop
destructive joint disease despite maximal therapy. This can be without the
presence of any active inflammation.
Goals of treatment in these
patients are:
1. Adequate pain relief
2. Maintain fucntion
3. Relief of other symptoms such
as fatigue and weakness.
4. Protect remaining joints
If there is no ongoing
inflammation, treatments should be focussed instead on non-pharmacological
treatments e.g physical therapy and occupational therapy.
Osteoarthritis
26 December 2020
23:21
It is difficult to estimate the
prevalence of OA as it is asymptomatic in many people, but the WHO estimate
that worldwide, approximately 10% of men and 20% of women over 60 have
symptomatic OA. In England, between 2000 and 2018, 3.1 million patients
presented with OA. Involvement of the knee or hip each accounted for almost 40%
of presentations. Generally, regardless of the principal joint, OA incidence
tends to start rising rapidly from the age of 40 years and peaks in the
mid-60s.
Distal
Interphalangeal joints and thumb carpometacarpal joints (OA)
Distal
Interphalangeal joints (OA, PsA) Proximal interphalangeal joints (RhA, OA)
Proximal interphalangeal joints, metacarpophalangeal joints (RA) Index and
middle finger metacarpophalangeal joints (haemochromatosis)
From <https://mle.ncl.ac.uk/cases/page/13099/>
Bony
(OA) or soft tissue (Inflammatory)
Red,
warm (RA, PsA, gout, pseudogout) Variable (inflammatory arthritis or
Inflammatory OA
From <https://mle.ncl.ac.uk/cases/page/13099/>
Morning
stiffness of >30minutes increases the likelihood of inflammatory arthritis
From <https://mle.ncl.ac.uk/cases/page/13099/>
Risk
factors include
·
Age
·
Gender (females gender
is associated with higher prevalence and severity)
·
Genetic predisposition
·
Previous injury to a
joint
·
Anatomic features (eg
Developmental Dysplasia of the Hip)
·
Obesity (which
surprisingly is associated even with hand OA)
·
Occupation (e.g. heavy
manual work, whole-body vibration – such as heavy goods vehicle drivers)
From <https://mle.ncl.ac.uk/cases/page/13101/>
Physiotherapist (Exercise regime
and pain relieving modalities)
Occupational therapist (Joint
protection, aids and adaptations, coping strategies)
Podiatrist (splinting, insoles,
footwear advice, minor foot surgery)
Social worker (financial
implications of disability, housing)
Appliance officer (splints,
braces, walking aids)
Psychologist (coping strategies,
chronic pain management)
This
may be a useful adjunct to therapy by relieving the pain. In hand OA, it is
often used to relieve pain from the carpometacarpal joint of the thumb. However
it is not without risk. You may remember the following from last year’s EoCP:
·
Main indication for
injection is relief of symptoms
·
Complications –
infection (very rare <1/15,000), pain, bruising, failure, complications of
steroid
·
Rest for at least 24
hours after
·
US guidance –
especially hip
·
Equipment – gloves,
antiseptic spray, needles, syringes, swabs, plaster, steroid and lidocaine
·
Aseptic non-touch
technique (ASNTT)
·
Knee slightly flexed
(10-15 degrees)
·
Medial or lateral
approach
From <https://mle.ncl.ac.uk/cases/page/13110/>
Arthroplasty
(joint replacement) in OA:
·
Indicated in patients
with severe pain when conservative measures have failed
·
A risk-benefit balance
assessment is required when deciding to operate on patients who have OA and are
obese due to the increased risk of complications from surgery given the
patients are obese
·
Patients who are obese
may be at higher risk of requiring revisions
·
96% of total knee
replacements have a 10 year survival rate (i.e., survival of the joint
replacement)
·
OA is the most common
indication for hip replacements with pain relief being one of the principal
driving factors
·
Severity of X-ray
changes in and of themselves do not pose a sufficient indication for hip
replacements
·
NICE guidelines advise
that obesity should not prevent a patient being referred for consideration for
hip replacement surgery
From <https://mle.ncl.ac.uk/cases/page/13111/>
Acne
26 December 2020
23:54
Acne
vulgaris: Summary
·
Acne vulgaris is a
chronic inflammatory skin condition affecting mainly the face, back and chest -
it is characterised by blockage and inflammation of the pilosebaceous unit (the
hair follicle, hair shaft and sebaceous gland). It presents with lesions which
can be non-inflammatory (comedones), inflammatory (papules, pustules and
nodules) or a mixture of both.
·
Up to 95% of
adolescents in Western industrialized countries are affected by acne to some
extent — 20 to 35% develop moderate or severe acne.
·
Complications of acne
include skin changes such as scarring, post-inflammatory hyperpigmentation or
depigmentation and psychosocial problems such as depression and anxiety.
·
All people with acne
should be advised:
o To avoid over cleaning the skin (which may
cause dryness and irritation) - acne is not caused by poor hygiene.
o To use non-comedogenic make-up, cleansers
and/or emollients with a pH close to the skin if needed.
o To avoid picking and squeezing spots which may
increase the risk of scarring.
o That acne treatments are effective but take
time to work - usually up to 8 weeks.
o That acne treatments may irritate the skin,
especially at the start of treatment - concentration or application frequency
may need to be reduced if skin irritation occurs.
·
In mild acne where
open and closed comedones (blackheads and whiteheads) predominate:
o A single topical treatment such as a topical
retinoid (for example adapalene, if not contraindicated) or benzoyl peroxide
should be considered as first-line treatment.
o If both topical retinoids and benzoyl peroxide
are poorly tolerated, azelaic acid can be considered.
·
In moderate acne where
inflammatory lesions (papules and pustules) predominate and response to topical
preparations alone is inadequate:
o Addition of an oral antibiotic such as
lymecycline or doxycycline (for a maximum of 3 months) can be considered.
·
A topical retinoid (if
not contraindicated) or benzoyl peroxide should always be co-prescribed with
oral antibiotics to reduce the risk of antibiotic resistance.
·
Macrolide antibiotics
(such as erythromycin) should generally be avoided due to high levels
of P. acnes resistance but can be used if tetracyclines are
contraindicated (for example in pregnancy).
·
Non-response to two
different courses of antibiotics, or scarring are indications for referral to
dermatology for consideration of treatment with isotretinoin.
o Combined oral contraceptives (if not
contraindicated) in combination with topical agents can be considered as an
alternative to systemic antibiotics in women – prescription should be guided by
the UK Medical Eligibility Criteria for Contraceptive Use.
·
Referral to
dermatology should be arranged if:
o A severe variant of acne such as acne
conglobata or acne fulminans (immediate referral) is suspected.
o Acne is severe, there is visible scarring or
the person is at risk of scarring or significant hyperpigmentation.
o Multiple treatments in primary care have
failed.
o Significant psychological distress is
associated with acne, regardless of severity.
o There is diagnostic uncertainty.
·
Follow-up should be
arranged 8-12 weeks after initiation of each treatment step:
o If there has been an adequate response,
treatment should be continued for at least 12 weeks.
o If acne has cleared or almost cleared,
maintenance therapy with topical retinoids (if not contraindicated) or azelaic
acid should be considered.
o If there has not been an adequate response,
adherence to treatment, adverse effects and use of comedongenic make up or
face creams should be considered before swapping to an alternative product
or the next treatment step.
Isotretinoin last line
From <https://mle.ncl.ac.uk/cases/page/13311/>
Eczema
Sunday, 27 December 2020
21:08
lllness affecting the skin is the
fourth most frequent cause of all human disease. It affects some 1.9 billion
people at any time, almost one-third of the world’s population.
In the UK 1 in 5 children have
atopic eczema
Eczema, like most chronic
conditions, can have a profound impact on patients’ quality of life and
self-esteem and can contribute to mental illness.
Eczema is a complex, chronic,
itchy, inflammatory disease that arises from a complex interaction of genetic
and environmental factors.
The typical appearance of eczema consists of
flares, with red, inflamed patches which sometimes blister and weep. Between
flares there can be normal skin or chronic skin changes of dry thickened
patches – worsened by excoriations from scratching.
There are varying patterns of
distribution depending on age.
Eczema can be seen alongside
hayfever and/or asthma as part of an ‘atopic triad’.
Eczema can be managed with
emollients, steroid cream, Tacrolimus, Pimecrolimus, Alitretinoin and
phototherapy.
Flexors usually
CML
and AML chromo
Sunday, 3 January 2021
20:49
The
9:22 translocation (the Philadelphia chromosome) is typically found in chronic
phase chronic myeloid leukaemia. The translocation encodes for a protein with
tyrosine kinase activity which is responsible for the disease and its
manifestations. Translocation 15:17 is typically seen in acute pro-myelocytic
leukaemia. Translocation 8:21 and inverted 16 are all associated with good
prognosis in acute myeloid leukaemia. Abnormalities of 5,7 and 8 are seen in
acute myeloid leukaemia and are associated with a poor prognosis. They may
be seen in patients with a preceding history of myelodysplasia which has
transformed to acute myeloid leukaemia.
Psoriasis
27 December 2020
21:36
Model answer "Psoriasis is a
complex, chronic, multifactorial, inflammatory disease that involves
hyperproliferation of the keratinocytes in the epidermis, with an increase in
the epidermal cell turnover rate"
Key points:
Psoriasis is a complex, chronic,
multifactorial, inflammatory disease that involves hyperproliferation of the
keratinocytes in the epidermis, with an increase in the epidermal cell turnover
rate
The classic appearance of
psoriasis consists of well-dermarcated, red, plaques with silver scale
Chronic plaque psoriasis is the
most common pattern and consists of plaques on extensor surfaces
Pitting, leukonychia,
onycholysis, subungual hyperkeratosis, and oil drop are all nail signs of
psoriasis – don’t forget to examine nails!
Psoriasis can be managed with
topical steroids, phototherapy, systemic drugs and biologics depending on the
patient and their disease severity
Psoriasis, like most chronic
conditions, can have a profound impact on patients’ quality of life and
self-esteem and can contribute to mental illness
Psoriasis is a systemic
inflammatory condition and its affects aren’t limited to the skin i.e.
psoriatic arthritis, cardiovascular risk
Medically unexplained
physical symptoms
27 December 2020
22:16
Summary
Medically unexplained physical
symptoms are common - they account for almost half of all GP consultations and
an equivalent proportion in the hospital setting.
Ensure that you have completed a
thorough history and examination to ensure that an underlying physical cause
has been excluded.
Avoid using diagnostic labels
where possible - offer the patient reassurance and the offer of an 'open door'
to discuss their concerns.
Medically unexplained physical
symptoms should be managed holistically. Management compromises a range of
psychological and pharmaceutical therapies.
Remember that all actions are not
necessarily harmless - arranging investigations and prescribing medications
come with their own risks. This should be weighed against any potential
benefits.
Asthma
27 December 2020
22:25
Under 17-
Clinical History
As with any diagnostic process, a key part is taking a thorough and
structured history. Features to ask about include
Wheeze, cough or breathlessness
Specific triggers: common ones include cold temperatures, exercise or
dust
Personal or family history of atopic disorders such as eczema or
hayfever
While important, history alone is not sufficient to make a diagnosis an
objective test should be used.
Physical Examination
Asthma is generally associated with expiratory polyphonic wheeze. A
physical examination will also help identify other causes of respiratory
symptoms and will help in building your differential diagnosis.
Remember that examination results can be normal in people with asthma as
wheeze is not always present.
Under 5s or unable to tolerate objective tests
Treat based on symptoms and clinical judgement and arrange for regular
review. If symptoms persist, arrange for objective tests at the age of 5 or as
soon as they are able to reasonably tolerate the tests if they are unable to
manage at 5.
Spirometery
Spirometery is an objective testing method which should be performed if
asthma is suspected. A forced expiratory volume in 1 second/ forced vital
capacity (FEV1/FVC) ratio of less then 70% is positive for obstructive airway
disease and will be more suggestive of asthma
As part of the procedure, consider a
in those with obstrutive spirometery results. An improvement in FEV1 of
12% or more is a positive test.
FeNO test (fractional exhaled nitric oxide)
In the age range of 5-16, consider this test if there is diagnostic
uncertainty after initial assessment. This implies either a normal spirometery
test or an obstructive spirometery test with a negative bronchodilatory
reversibility test.
A FeNO level of 35 or more is a
postive test.
Other Tests:
Skin prick testing, serum IgE, and eosinophil counts should not be
routinely offered as they are not diagnostic.
Consider offering the above after a formal diagnosis of asthma has been
made to help identify triggers.
Over 17
Initial Assessment:
Initial investigation with clinical history and physical examination
are much the same as with ages 5-16. Important to ask in both cases whether
they smoke, though this will be more relevant in the older population
Fractional Exhaled Nitric Oxide Test
Regard a FeNO level of 40 or more as a positive test.
Be aware that a person's current smoking status can lower FeNO levels
both acutely and cumulatively. However, a high level remains useful in
supporting a diagnosis of asthma test to adults (aged 17 and over) if a
diagnosis of asthma is being considered.
Spirometery
Similar to ages 5-16, a FEV1/FVC of less then 70% is a positive test
and suggestive of obstructive airway disease.
Offer a BDR test to adults with obstructive spirometery. an improvement
in FEV1 of 12% or more is a positive test
Peak Flow Variability
In cases where the diagnosis is unclear (normal spirometery or
obstructive spirometery with positive BDR but FeNO levels of 39ppb or less)
after initital assessment and FeNO test then monitor peak flow variability for
2-4 weeks.
Greater then 20% variability is a positive test.
Other Tests:
Skin prick testing, serum IgE, and eosinophil counts should not be
routinely offered as they are not diagnostic.
Consider offering the above after a formal diagnosis of asthma has been
made to help identify triggers.

Short-acting Beta agonist (SABA) such as salbutamol 100microgram or terbutaline 250microgram. Usually
prescribed when required (two puffs as
required)
Method of Action:
These acheive bronchodilation through activation of beta-2 receptors on
the airway smooth muscle. Onset in most preperations will be within 5 minutes.
Primary use if for relief of breathlessness and chest tightness associated with
exacerbations
Side effects:
Fine tremor most noticible in hands and tachycardia. Also asoociated
with hypokalaemia in large doses.
Long-acting Beta2 adrenoreceptor (LABA) such as salmeterol or formoterol. Inhaled once or twice daily and
combined with inhaled corticosteroid as fixed-dose combinations
(salmeterol/fluticasone and formoterol/budesonide) in the same inhaler.
Method of Actions:
Acheive bronchodilation via activation of beta-2 receptors on the airway
smooth muscle. Use is typically or
maintenance of peristant asthma not controled with inhaled corticosteroids.
Also used as maintenance treatment for COPD patients with persitant
breathlessness.
Side Effects:
Fine Tremor in hands, headache, muscle cramps and tachycardia.
Inhaled corticosteroids:
Patients
who have regular persistent symptoms need inhaled corticosteroids.
Beclometasone is the most used and available in doses of 50,100,200 and 250
micrograms per puff. Others are budesonide,fluticasone propionate,fluticasone
furoate, mometasone furoate and triamcinolone.
Method
of Action:
Anti-inflammatory
effect on bronchial mucosa and reduces hyper-responsiveness of the bronchial
tract to exogenic challenges. Used as prophylactic management of mild, moderate
and severe persistant asthma.
Note
that the onset of action can take up to 6 weeks to see full response! It is important to emphasise this to patients
as some may give up on the ICS as they do not immediately feel the perceived
benefits!
Commonly patients
experience local side effectus such as oral thrush. Other more rare side
effects include: subcapsular cataract (rare), osteoporosis (high dose, such as
beclometasone >800mcg daily) and growth retardation (>400 mcg daily) in
children.
Oral corticosteroids and steroid sparing agents
Usually
used for acute exacerbation or longer-term use when other drugs have not
controlled symptoms successfully. A typical dose for an acute exacerbation of
asthma would be 40mg of prednisolone for 5 days.
Leukotriene receptor antagonists-
Examples
such as montelukast and zafirlukast are given orally and effective in
aspirin-intolerant asthmatic patients, rhinitis associated asthma and viral
wheeze. Should be started when the symptom is not controlled after SABA and
low/medium dose ICS.
Antimuscarinic bronchodilators
Short
acting antimuscarinic bronchodilators (ipratropium) is usually used in severe
exacerbation of asthma. It is not been shown to be of any benefit in patient on
standard therapy.
Long-acting
antimuscarinics (tiotropium,aclidinium) can be tried in severe cases.
Anti-inflammatory drugs
Sodium cromoglicate
and nedocromil sodium prevent activation of mast cells,eosinophils and
epithelial cells. They are not commonly used.
Monoclonal antibodies-
Omalizumab
is given subcutaneously every
2-4 weeks and very effective although expensive. It is a recombinant humanized
monoclonal antibody directed against IgE and down regulates the activity of
mast cell and basophils. Newer agents are mepolizumab,reslizumab and
benralizumab.
Antibiotics-
Probably
a bit of a trick entry this one. There is little evidence that antibiotics help
in acute exacerbations and should not be used in the treatment of an
exacerbation unless the underlying cuase is thought to be infective ( which is
rare in asthma).
Please
see NICE guidelines for the recommended treatment pathway. These are
recommendations and where asthma is well controlled on current treatment there
is no need to change to try and adhere to these guidelines
SABA
1.
Start with SABA reliever therapy. For those with infrequent short lived wheeze
and normal lung function, this alone may be sufficient.
SABA +
ICS
2. In
most cases, an additional low dose ICS is the first line maintenance therapy in
adults. Start when symptoms at presentations clearly suggest uncontrolled
asthma ( such as three exacerbations a week or nocturnal waking).
SABA +
ICS + LRTA
3. If
uncontrolled despite ICS and SABA therapy then offer a LTRA in addition to the
ICS and review response over 4-8 weeks.
SABA +
LABA + ICS +/- LRTA
4. If
uncontrolled, offer a LABA and ICS inhaler and review the LRTA treatment. This
involves a discussion with the patient to establish whether or not to continue
the LRTA. Should be based on side effects vs what perceived benefit the patient
has experienced.
MART
+/-LRTA + ICS
5. If
uncontrolled, offer to change the ICS and LABA to a combined ICS and LABA
inhaler (MART). This inhaler also included a fast acting LABA and can be used
for both maintenance and relief of sympoms. This is in addition to the low dose
maintenance ICS
MART or
LABA+ICS+SABA with moderate dose increase of ICS +/- LRTA
6. If
uncontrolled consider increasing the ICS dose to moderate dose.
MART or
LABA+ICS+SABA with high dose increase of ICS +/- LRTA. Options as
below. Refer to specialist.
7. If
Uncontrolled consider increasing ICS to high maintenance dose, trial an
additional drug such as a long-acting muscarinic recptor agonist or
theophylline or seek specialist advice.
From <https://mle.ncl.ac.uk/cases/page/14739/>
For
exercise induces asthma, having a reliever inhaler prior to activity can often
help manage symptoms.
Likewise,
maintaining an asthma diary and an asthma action plan can help direct
management
From <https://mle.ncl.ac.uk/cases/page/14745/>
·
Asthma is a lifelong
chronic inflammatory disease of the respiratory system characterized by
bronchial hyperresponsiveness, episodic exacerbations (asthma attacks), and
reversible airflow obstruction.
·
Allergic (extrinsic)
asthma usually develops in childhood and is triggered by allergens such as
pollen, dust mites, and certain foods.
·
Nonallergic (environmental
or intrinsic) asthma usually develops in patients over the age of forty and can
have various triggers, such as cold air, medication (e.g., aspirin), exercise,
and viral infection.
·
The cardinal symptoms
of asthma are intermittent dyspnea, coughing, and high-pitched expiratory
wheezing. Symptoms remit in response to antiasthmatic medication or resolve
spontaneously upon removal of the trigger.
·
Confirmation of the
diagnosis involves pulmonary function tests, allergy tests, and chest x-ray.
First-line treatment consists of inhaled bronchodilators (e.g., short-acting
beta-2 agonists) for acute exacerbations and inhaled corticosteroids (e.g.,
budesonide) for long-term asthma control.
·
Patients should be
taught the correct usage of inhalers for self-medication and measurement of
peak expiratory flow (PEF) to self-monitor disease progression and severity.
·
Severe asthma
exacerbation can be life-threatening and may require emergency treatment and/or
hospitalization.
·
As patients get older,
the management of asthma changes as well. Regular review of the patient at
least once a year is recommended. At the same time, changes in treatment may
also be needed due to other comorbidities such as arthritis or cardiac disease.
From <https://mle.ncl.ac.uk/cases/page/13033/>
Hypertension
27 December 2020
22:59
NICE recommend assessing frailty in primary care
settings when patients have multiple morbidities and/or who are at risk of
adverse events (e.g. falls). NICE recommend assessing frailty using one or more
of the following:
·
an informal assessment of gait speed (for example, time taken to
answer the door, time taken to walk from the waiting room)
·
self-reported health status (that is, 'how would you rate your
health status on a scale from 0 to 10?', with scores of 6 or less indicating
frailty)
·
a formal assessment of gait speed, with more than 5 seconds to
walk 4 metres indicating frailty
·
the PRISMA-7 questionnaire, with
scores of 3 and above indicating frailty.
In hypertension, many of the medications we prescribe
can cause postural hypotension as a side effect, which can cause dizziness and
syncope. If someone is frail, and we give them a medication that could
potentially make them dizzy and fall, we could significantly worsen their
frailty and quality of life.
From <https://mle.ncl.ac.uk/cases/page/9615/>
66% has comorbidity
Key Points
Most cases (95%) of hypertension
are primary (essential), where there is no definitive, treatable cause of the
raised blood pressure. Secondary hypertension (5%) causes include renal,
obesity, pregnancy-induced, endocrine and drug-related. It is essential to
screen for secondary causes when a patient presents with hypertension.
When history taking it is
important to ask about all the modifiable lifestyle factors that increase blood
pressure, such as smoking, increased alcohol intake, diet high in
salt/saturated fat and low levels of physical activity.
Important clinical indicators
that signal end organ damage are changes on fundoscopy (papilledema, AV
nicking, haemorrhages, exudates) and proteinuria.
It is key to assess a patient’s
cardiovascular risk using an appropriate tool (such as QRISK3)
Many patients often struggle to
take anti-hypertensive medication regularly either due to lack of symptoms from
hypertension, side effects of medication or medication fatigue.
66% of patients with hypertension
have a co-morbid condition
It is important to assess the
risks and benefits of starting someone on blood pressure medication,
particularly in the elderly, due to their side effects.
Breast cancers
27 December 2020
23:04
Most
breast lumps are benign and include fibroadenomas, papillomas, breast cysts,
and breast abscesses. Malignant breast lumps may include DCIS but these are
very rarely mass forming (asymptomatic) and usually present via screening.
From <https://mle.ncl.ac.uk/cases/page/9312/>
Triple assessment-
Clinical
assessment +/- imaging +/- biopsy
From <https://mle.ncl.ac.uk/cases/page/9312/>
Breast cancer
presentation-
Breast lump – either painful /
painless
Nipple changes / eczema / blood
stained discharge
Nipple or skin tethering and
indrawn
Axillary lymphadenopathy
Screen detected abnormality
Incidental finding on other
imaging (e.g. CT chest)
Inflammatory breast cancer
The two imaging modalities used
in the breast one stop clinic are mammogram and ultrasound.
Mammogram: This is a dual plane X-ray of the
breast. All patients over 40 have a bilateral mammogram in the one stop clinic
(assuming that they haven’t had a mammogram in the last year). Mammogram is
rarely performed on patients under the age of 40 as their higher breast density
makes it difficult to detect a dense abnormality (like cancer) leading to very
poor test sensitivity.
Ultrasound: All patients who have a breast abnormality on initial
clinical assessment will undergo ultrasound of the abnormality (regardless of
age). Note that it is an ultrasound of the abnormality in the breast as opposed
to an ultrasound scan of the whole breast to “look for” an abnormality;
although breast ultrasound is an excellent tool for assessing a lesion, it has
a very low sensitivity as a breast screening tool to find an abnormality.
As
the risk of breast cancer increases with age, breast screening in the UK is
offered to all women at the age of 50 who are registered with a GP. They are
invited for screening every three years until their 71st birthday. They can
choose to continue with the programme after this time period at their own
request. The procedure is a bilateral mammogram, taken in a horizontal and
vertical plane.
From <https://mle.ncl.ac.uk/cases/page/10066/>
In all
aspects of medicine, choosing a treatment requires a risk/benefit assessment.
Breast cancer prognosis varies from excellent to very poor, and these very
different prognoses will have very different risk/benefit balances. Because of
this, treatment “package” needs to be individualised for the patient. Before
discussing treatment options in this tutorial, it is therefore important to
outline the multiple factors that contribute to the prognostic information in
the diagnoses of breast cancer patients.
The
most basic prognostic factors are grade of tumour, size of
tumour, and axilla lymph node status.
Grade:
a measure of cellular differentiation, from grade 1 (well differentiated) to
grade 3 (poorly differentiated). Essentially, a measure of how “aggressive” the
individual cells are deemed to be.
Lymph
nodes can be scored from 1-3, with 1 = 0 nodes affected and 3 = >3 nodes
affected.
These
basic prognostic factors can be combined to give a 5-year survival probability
in the Nottingham Prognostic Index (NPI):
(0.2*size)
+ grade + lymph node score
A score
below 2.5 has a 93% 5-year survival, and a score of 5.5+ has a 50% 5-year
survival.
Other
prognostic factors include histology and stage.
From <https://mle.ncl.ac.uk/cases/page/9311/>
· Molecular subtyping involves testing ER
status, HER2 status, and in some patients oncotype DX
· ER status predicts response to hormone
therapy
· HER2 predicts response to trastuzumab and has
a poor prognosis
· HER2+ and triple negative cancers are given
chemotherapy
· TNM stage and sometimes oncotype DX determine
whether chemotherapy is necessary in ER+ HER2- cases
From <https://mle.ncl.ac.uk/cases/page/10495/>
Risks of
radiotherapy include:
Short
term: rib fracture, sunburn, blistering, oesophagitis, pneumonitis, lymphoedema
to breast and arm, fatigue
Long
term: lung fibrosis, osteonecrosis, coronary artery disease, pericarditis,
leathery skin, secondary malignancies (angiosarcoma, lung cancers)
Contraindications:
There
are some absolute and relative contraindications that
would prevent a patient from receiving radiotherapy. These include:
Absolute
contraindications:
· Connective
tissue disorders with significant vasculitis
· Prior
radiotherapy in the same part of the body
· Li-Fraumeni
syndrome (TP53 mutation), due to risk of secondary malignancies
Relative
contraindications:
· Significant
pre-existing lung disease
· Pacemaker
in the radiotherapy field
· Pregnancy
From <https://mle.ncl.ac.uk/cases/page/10497/>
Key
points:
· Local
treatments include surgery and radiotherapy
· Surgery
is split into the breast operation and axilla operation
· The
breast operation can be a mastectomy or breast conserving surgery with
radiotherapy
· The
axilla operation can be clearance, sentinel node biopsy, or omitted
· Radiotherapy
reduces recurrence
· Radiotherapy
is contraindicated in a number of patients
· Don’t
take blood from an arm that has had axillary clearance – it can trigger
lymphoedema
From <https://mle.ncl.ac.uk/cases/page/10497/>
Who
gets it?
Anyone
ER+ will usually receive
hormone therapy.
What is
it?
Hormone
therapies aim to prevent
the binding of oestrogen to oestrogen receptors by various modes of action, and
therefore inhibit ER+ tumour cell proliferation.
In premenopausal women,
the commonest drug used is tamoxifen.
Tamoxifen is a SERM (selective oestrogen receptor modulator), which
competitively binds the oestrogen receptors present in breast tissue.
In postmenopausal women, aromatase inhibitors (AIs) are usually used instead of
tamoxifen. AIs include letrozole, anastrozole, and exemestane. They work by blocking
non-ovarian sources of oestrogen, such as from fat cells. AIs show a lower rate
of recurrence than tamoxifen, however as they only affect non-ovarian sources
of oestrogen, they do not
work in premenopausal women.
From <https://mle.ncl.ac.uk/cases/page/10498/>
Chemo-
Regime
options include FEC (fluorouracil,
epirubicin, and cyclophosphamide) and EC (epirubicin
and cyclophosphamide). These regimes may have other medications added on top of
them. Taxanes (e.g.
docetaxel) may be added in patients with poor prognoses, for example node
positive patients (a common example of a taxane containing regime is FEC-T). Taxanes comes with the risk of
additional side effects, such as neuropathy, but reduce recurrence risk. Platinum-based medications (e.g.
carboplatin) may be added if the cancer is triple negative.
From <https://mle.ncl.ac.uk/cases/page/10499/>
Side
effects
Common
side effects of chemotherapy include:
Nausea,
appetite and weight loss, changes to taste, changes to skin and nails, severe
fatigue, immunosuppression, easy bleeding and bruising, bowel disturbance, hair
loss
Potentially
serious complications include:
Deterioration
in kidney function, thrombosis, changes in hearing
Severe
complications include:
Cardiotoxicity, neutropenic sepsis (especially with taxanes), death
Possible
late effects include:
peripheral
neuropathy, early menopause, infertility, secondary malignancy (with certain
chemotherapies)
It is
important to discuss these risks with the patient prior to treatment.
From <https://mle.ncl.ac.uk/cases/page/10499/>
Key
points:
· Systemic treatments include hormone therapy,
chemotherapy, HER2 therapy, and bisphosphonates
· Hormone therapy is given in ER+ cancers
· Tamoxifen is the hormone therapy drug used in
premenopausal patients, and AIs are preferred in postmenopausal patients
· Chemotherapy regimes include FEC and EC
· Taxanes may be added if the cancer has poor
prognosis
· Platinum-based medications may be added in
triple negative cancers
· Chemotherapy has a high morbidity
· Serious complications include cardiotoxicity,
neutropenic sepsis, and death
· There is a future risk of infertility and
sometimes secondary malignancy
From <https://mle.ncl.ac.uk/cases/page/10499/>
Heart failure
28 December 2020
00:47
What
is Heart Failure?
Heart
failure is a complex and progressive (i.e. it will naturally
deteriorate over time) clinical syndrome that you will encounter frequently in
your clinical practice. In short, heart failure is the result of impaired ventricular filling or contractility,
whether due to structural or functional causes.
This is not synonymous with
"cardiomyopathy" or "left ventricular dysfunction" - these
are themselves possible structural or functional causes for developing heart
failure.
The
major clinical manifestations of heart failure are: fluid retention, dyspnoea, and fatigue.
From <https://mle.ncl.ac.uk/cases/page/13016/>










From <https://mle.ncl.ac.uk/cases/page/14541/>
Arthroscopy
28 December 2020
01:34
A
meniscal tear is the commonest soft tissue ailment of the knee joint and causes
pain, swelling and mechanical symptoms. It can affect patients of all ages.
Patients whose symptoms are refractory to first line conservative treatment and
are medically fit to undergo an anaesthetic can benefit from arthroscopic knee
surgery. A meniscectomy removes the pain stimulus emanating from the meniscal
tear but in some patients, increases the risk of developing secondary OA. New
arthroscopic techniques, including meniscal repair, have shown promising
results but is a more technically demanding procedure with a stricter selection
criteria that is dependent on the tear pattern and has a more entailed
post-operative rehabilitation programme.
Joint Replacement
28 December 2020
01:35
The
prevalence of osteoarthritis is rising as the life expectancy of the general
population continues to rise and patients live long enough to develop
degenerative diseases. OA causes debilitating pain in the affected joints and
has a major impact on quality of life. Patients whose symptoms are refractory
to first line conservative treatment and are medically fit to undergo an
anaesthetic can significantly benefit from major joint replacement
surgery.
From <https://mle.ncl.ac.uk/cases/page/10552/>
Breast conserving surgery
28 December 2020
01:36
The
majority of women presenting with breast cancer undergo breast conserving
surgery (and therefore breast radiotherapy) as opposed to a mastectomy. There
are a number of forms of breast conserving surgery ranging from a simple wide
local excision to breast reduction surgery or combined with volume replacement
procedures.
From <https://mle.ncl.ac.uk/cases/page/10548/>
Cataract surgery
28 December 2020
01:36
In a
nutshell
Cataract
is an opacification of the crystalline lens. It is managed surgically by
removal of the cataract and insertion of a new clear lens.
Patients
should be referred for cataract surgery only when they have significant visual
loss and are fit enough for surgery.

Cataract
surgery is usually performed as a day case surgery under topical or local
anaesthetic. The cataract is
removed using a technique called phacoemulsification. Visual recovery is
usually immediate depending on anaesthetic used.
Post
operatively patients have a short course of antibiotic eye drops and a reducing
course of steroid eye drops for 4-6 weeks.
The
most important risk is that of ENDOPHTHALMITIS which is potentially sight threatening. Any
patient with increasing pain, redness and loss of vision should attend their
place of surgery ASAP. This is one of the very few true ocular
emergencies.
Posterior
Capsular Opacity can occur subsequent to cataract surgery and can be treated by
YAG capsulotomy.
From <https://mle.ncl.ac.uk/cases/page/9931/>
Cholecystectomy
28 December 2020
01:38
Laparoscopic cholecystectomy is a commonly performed
general surgical operation usually for symptomatic gallstones. In the elective
setting it is usually performed as a day case procedure with no routine
follow-up.
Recovery is rapid, although patients should show some
caution with regards to strenuous activity in the first few postoperative
weeks.
From <https://mle.ncl.ac.uk/cases/page/8708/>
Colectomy
28 December 2020
01:38
Colectomy is a major surgical
procedure which may be used to treat a variety of benign pathologies as well as
malignancy. It may also be performed as an emergency procedure. This is most
commonly due to benign problems such as ischaemia, or perforation, but patients
may also present with bowel obstruction due to malignancy.
A stoma may be created in high
risk patients where concerns about an anastomosis healing exist, or due to
necessity in the case of sub-total and total colectomies.
Patients usually stay in hospital
for approximately a week after surgery and can take several weeks or months to
recover fully from the operation.
Colonosopy
28 December 2020
01:39
Cystoscopy
28 December 2020
01:39
Cystoscopy
is a commonly performed diagnostic procedure that allows imaging of the inside
of the bladder. It is usually performed to identify a source of
haematuria in patients who may have a bladder cancer, or to follow up patients
how have had bladder cancer to detect recurrence.
It is
performed under local anaesthetic as a day case or outpatient procedure.
Recovery
is rapid, although sometimes complicated by infection or bleeding.
Treatment
procedures can also be performed transurethrally. These usually require
general anaesthetic, take longer to recover from and usually require an
overnight stay.
From <https://mle.ncl.ac.uk/cases/page/8689/>
Hernia repair
28 December 2020
01:40
Inguinal
hernia repair is a commonly performed operation to treat symptomatic inguinal
herniae. It may be performed as an open operation or a laparoscopic operation.
NICE guidelines indicate that a laparoscopic approach should be considered for
those with a bilateral hernia (allowing both to be easily fixed at the same
time) and those with a recurrent inguinal hernia, where the initial approach
was an open operation.
It is
usually performed under a general anaesthetic but may be done under a spinal
anaesthetic or local anaesthetic.
Recovery
is rapid, although sometimes complicated by infection or bleeding and care must
be taken by the patient not to over exert themselves in the first 6 weeks
whilst wound heals and is strengthened by the mesh.
From <https://mle.ncl.ac.uk/cases/page/8713/>
Mastectomy
28 December 2020
01:41
Although
most breast cancer is treated with breast conserving surgery, a mastectomy is
still a common operation in breast cancer and patients considered high risk for
developing breast cancer. Mastectomy can be performed with or without a
simultaneous reconstruction procedure, of which there are many options.
Physical recovery is fairly rapid but psychological recovery can take time and
require professional support.
From <https://mle.ncl.ac.uk/cases/page/8724/>
Cystopathology
03 January 2021
16:53
The
types of cytological sampling are:
·
Exfoliative cytology
·
Abrasive cytology
·
Interventional
(aspiration) cytology
·
Imprint cytology
Each of
these types, and the methods by which they are collected are described in more
detail in the following sections.
From <https://mle.ncl.ac.uk/cases/page/14658/>
Exfoliative
cytology involves the collection and microscopic examination of shed or
desquamated epithelial cells.
The
cells are collected from body fluids including sputum, urine, bile,
cerebrospinal fluid, vaginal discharge, pleural fluid, ascitic fluid, and fluid
from cysts often using a syringe or cotton swap.
The
samples collected contain cells that have been shed from surrounding tissues.
For example, sputum will contain cells derived from the buccal cavity, pharynx,
larynx, trachea and lungs.
The
sample collected should be processed as soon as possible to prevent
deterioration of the cells by drying out or through enzymatic or bacterial
activity.
From <https://mle.ncl.ac.uk/cases/page/14658/>
Abrasive
cytology involves the removal and examination of of cells from mucosal linings
and body surfaces.
The
cells are collected by scraping, brushing or washing the surface of the tissue
of interest. Unlike exfoliative cytopathology, this enables the sample to be
enriched with cells obtained directly form the surface of the tissue of
interest.
Samples
can be taken form superficial or deep lesions in tissues such as skin (scraping
of lesion), cervix (cervival Pap smear), gastrointestinal tract (endoscopy and
gastric lavage) and the oral oral mucosa (buccal smear).
The
video below describes what is involved in a cervical smear test.
From <https://mle.ncl.ac.uk/cases/page/1465
Aspiration
cytology involves the removal and examination of cells form a palpable solid
lump or mass.
The
cells are removed from lumps or masses, e.g. surface breast, lymph node or
tumour masses, with or without suction by needle aspiration. This is commonly
called fine needle aspiration (FNA) cytology. The needle can be inserted
directly for palpable lumps, or under radiological (ultrasound or CT) guidance
for non-palpable lumps.
You may
find this video showing how to collect a sample of cells by fine needle
aspiration interesting.
From <https://mle.ncl.ac.uk/cases/page/14658/>
Imprint
cytology involves the collection and examination of cells from the surface of
tissues.
The
cells are collecting my making in imprint of the tissue in question onto a
glass slide, leaving cells on the slide when it is removed.
From <https://mle.ncl.ac.uk/cases/page/14658/>
Stains
used in cytopathology include:
·
Papanicolaou (Pap)
stain. Pap stain is actually comprised of 5 stains that provide a multicoloured
cell sample allowing identification of different cell types and cellular
features. Pap stain is very reliable and widely used, notably for cervical
smears (Pap test or Pap smear).
·
Haematoxylin and eosin
(H&E) stain. It is one of the main stains used in histopathology and
cytopathology. Eosin stains the cytoplasm and extracellular matrix of cells
pink, while haematoxylin stains nuclei blue and is often used for fluids and
aspirates.
·
Other stains you many
come across are Romanaowski, Leishman and Giemsa (May Grunwald Geimsa) stains,
which may be used for fluids and aspirated samples.
From <https://mle.ncl.ac.uk/cases/page/14662/>
Indications
for cytopathological investigations include:
·
To support diagnosis
by differentiating between malignant and benign lesions
·
To support the
diagnosis of malignancy and the identification of the neoplasic cells in the
tumour
·
To support the
diagnosis of pre-malignant disease
·
Identification of
inflammation and some types of pathogens
·
To examine/monitor
squamous cells in vaginal smears which are influenced by ovarian hormones
·
To monitor responses
to chemotherapy and radiotherapy.
From <https://mle.ncl.ac.uk/cases/page/14664/>
Advantages
of cytopathology
·
Good morphological
detail can be obtained
·
Able to characterise
the cellular components of various fluids
·
Relatively quick to
obtain a sample and determine a diagnosis
·
Cost effective
·
Minimally invasive
diagnostic procedures that do not require surgery or anaesthesia
Limitations
of cytopathology
·
Tumors cannot be
graded
·
Margins cannot be
evaluated
·
Limited information
can be achieved about the structural arrangement of the cells within a lesion
·
Less definitive
diagnosis can be achieve as to specific tumour type or distribution of
inflammatory infiltrate
·
Potential for negative
test due to relatively small sample size and blind nature of many collection
techniques meaning he sample may not be representative of the primary lesion
Cyctopathology
can aid clinical diagnosis, but results must be considered in the context of
the overall case. Negative results should not be treated as conclusive given
the limitations.
From <https://mle.ncl.ac.uk/cases/page/14727/>
Tissue
samples, or biopsies, can be taken from almost anywhere on or in your body,
including the skin, organs and other structures.
There
are different types of biopsy which include:
·
Excision – a sample of tissue is removed in a
surgical procedure.
·
Endoscopic – a sample of tissue is removed using an
endoscope.
·
Punch – a sample of skin is obtained by
punching a small hole in the skin
·
Needle – a sample of tissue is removed from and
organ or tissue under the skin using a needle, guided by ultrasound, X-ray, CT
or MRI.
Histopathology
03 January 2021
17:01
Histopathology
includes macroscopic examination of the tissue, as well as examination of very
thin sections of the tissue under a microscope.
In this section we
will consider:
·
How samples are collected
·
How samples are processed
·
Indications for how histology can
support the detection, or exclusion, of disease and its management
·
The advantages and limitations of
histology
From <https://mle.ncl.ac.uk/cases/page/14666/>
Once
collected, the sample is fixed to harden and preserve the tissue in a solution
such as formaldehyde. The gross biopsy is then examined and described before
sections are selected to be dissected for microscopic study. The sample
is then processed further as described in the next section.
From <https://mle.ncl.ac.uk
Surgical
pathology is the study of tissues removed from living patients during surgery
that help diagnosis, informs the ongoing surgical procedure, and helps
determine a treatment plan. For example, when performing cancer surgery,
pathological examination of the tissue removed can help the surgeon to
determine whether or not to remove more surrounding tissues.
From <https://mle.ncl.ac.uk/cases/page/14657/>
ses/page/14667/>
The
indications for histopathological investigation include:
·
To aid diagnosis, or
exclusion of, disease
·
To support surgical
procedures by determining resection margins
·
To help determine
appropriate treatment options
·
To determine sentinel
lymph node involvement
·
To support the determination
of a prognosis by type, grade and stage of malignant disease
·
Monitoring response to
treatment and clinical course of disease
From <https://mle.ncl.ac.uk/cases/page/14729/>
Advantages
of histopathology
·
Enables evaluation of
resection margins
·
Provides information
about the structural arrangement of tissue within the lesion, e.g. vascular and
lymphatic invasion
·
Provides more information
than cytology providing a more definitive diagnosis as to the specific type of
tumour
·
Provides information
to inform staging, prognosis and treatment options
·
Can be used to monitor
response to treatment and clinical course of disease, e.g. in coeliac disease,
ulcerative colitis and cervical dysplasia
Limitations
of histopathology
·
Sample collection can
be invasive and traumatic
·
Processing and
obtaining a diagnosis can take longer than the likes of cytopathology
·
More expensive than
cytopathology
From <https://mle.ncl.ac.uk/cases/page/14730/>
Population-based management of conditions
03 January 2021
17:03
"The
aim of medicine is to prevent disease and prolong life, the ideal of medicine
is to eliminate the need of a physician." William Mayo (1861-1939)
Population
approaches may be defined as the science and art of promoting and protecting
health and well-being, preventing ill-health and prolonging life through the
organised efforts of society.
The
principles of population health are : (Faculty of Public Health 2020)
1. Health Protection. Measures to control
communicable diseases and environmental hazards including public health
emergencies
2. Health Promotion and Disease Prevention.
Societal and individual interventions to promote and protect health
3. Health and Care Public Health. The
organisation and delivery of safe and high quality services to prevention,
treat and care for patients and improve their outcomes.
These
are underpinned by epidemiology and health improvement which tackles health
inequalities.
From <https://mle.ncl.ac.uk/cases/page/13225/>

Therapeutics
03 January 2021
18:28



Adverse drug reaction






MOSLER
06 January 2021
23:33
Risk and benefits
What is going to happen if we
don’t do anything-
Risk of rupture per year
1 year 9.4 % 5.5 to 5.9cm risk of
rupture
1 in 10 4 year aftersurgery die
open and endocasvular surgery
30 days after surgery 4/100 die
open, 1/100 endovacular
https://www.nhs.uk/conditions/abdominal-aortic-aneurysm/
Risk of doing something-
Risk of surgery- risk of heart
attack during surgery, having a major embolic clot , risk of bleeding, risk of
losing a leg
Risk to life (MI) and risk to limb (ischaemia) (major risks), rupture of AAA,
Minor risks, risk of bleeding
after surgery, risk of infections after surgery, problems with bowels, risk of
another operation to put it correct, lung complication, kidney, non fatal
stroke,COVID risk coming to hospital,
Higher risk of death if they have
COVID during surgery
Anaesthetic risks but usually
very low.
Benefits-
Prognostic- increase their life
expectancy, no more symptoms
Stent option- endovascular
options
Other options?
Medication wouldn’t solve this
problem, can reduce risk- aspirin can help but if it ruptures they bleed more
3 options-
Treat conservatively doing
nothing,
Do surgery, laparotomy, graft to
replace
Do stenting, to avoid it
rupturing. (higher chance another surgery) say less invasive endovacular done
by interventiona radiologist usually covered by surgerons)
Vascular MDR to discuss this
patient- recommend one of the following options( surgeron, radiologist, IR,
gastro doctor, cardiologist, anaesthetic( fit for surgery))
Gold standard
Change lifestyle factors
Medical
management with beta-blockers, cessation of smoking and management of risk
factors, such as dyslipidemia and hypertension, may be helpful in patients with
small- to medium-sized aneurysms that are not treated surgically.
Advice them for both surgery and
conservative management- secondary
prevention for pt going to surgery, primary prevention for someone not going to
surgery
From <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3076160/>
They will do preoperative
assessments to check his risks for surgery, ?diabetes
Cardiology assessment-
MDT!!!!
Ask about past medical history-
hypertension, heart failure, previous myocardial infaraction, smoke? Family
history?
Previous surgery? Stents?
Abdominal surgery?(risky if redo surgery)
Size of patient? 5.5 cm AAA in
small is different to large person
Body surface area, body mass
index to measure
Ultrasound- simple way to
identify Aneurysm, best would be CT , reconstruction, 3D picture, extent of
AAA, position of AAA, relation to other vessels (coeliac, mesentary, renal
arteries), bifurcation graft or simple one graft.
AAAs
are mostly asymptomatic and found incidentally. The incidence of AAA is higher
in Caucasian men, individuals older than 60 years of age and smokers. Diagnosis
is usually reached using imaging modalities. Aneurysm rupture is a medical
emergency and risk of aneurysm rupture increases with increasing diameter,
rapid expansion, symptomatic aneurysm and history of smoking. Surgical
intervention is recommended for all symptomatic aneurysms and asymptomatic
aneurysms greater than 5.5 cm in diameter. Regular surveillance through imaging
studies should be conducted in asymptomatic aneurysms 3 cm to 5.5 cm in size.
Medical management with beta-blockers, cessation of smoking and management of
risk factors, such as dyslipidemia and hypertension, may be helpful in patients
with small- to medium-sized aneurysms that are not treated surgically.
From <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3076160/>
Wriske
1
15 January 2021
00:22


Wriske
2
15 January 2021
00:23
Situation
You are a Foundation year 2 doctor working in General
Practice.
Patient details
Name:
David Bannister
Address:
47 Hauxey Lane
Newtown
NE56 1EE
Date of birth:
24/02/1932
Patient
number:
4956 545 223
History
David Bannister has come to the Practice for
review.
He has a known diagnosis of pancreatic cancer with
widespread metastatic disease.
His regular medications are
Morphine sulphate modified release tablets
30 mg 12 hourly
Mr Bannister’s dose of morphine was increased 5 days ago
to improve control of his pain. The increased dose has been effective in
pain control, but he has started to suffer from hallucinations.
Examination
Temperature:
36.8 centigrade
Pulse:
90 beats per minute
Blood pressure:
118/87 mm Hg
Respiratory rate
14 breaths per minute
Oxygen saturations (on air)
98%
His airway is patent.
He is alert and responsive. He is orientated and
does not appear confused. The rest of his physical examination is normal.
Investigation
His blood glucose level is 5.3 mmol/L (usual fasting
range 3.0 – 6.0).
Renal and liver function are normal
·
TASK
You think the hallucinations may be an adverse effect of
the morphine.
You decide to prescribe oxycodone in a twice daily
preparation form in a dose equivalent to Mr Bannister’s current morphine dose
in the hope that analgesia will remain effective but without this side effect.
Please prescribe this on the FP10 prescription provided
in Question 2 Answer
From <https://mle.ncl.ac.uk/cases/page/19168/>
Wriske
3
15 January 2021
00:23
Situation
You are a Foundation doctor in medicine, working with
your consultant Dr Brown, in outpatients at Compassion Hospital.
Patient details
Name:
Khaled Aljboor
Date of
birth:
24/01/1985
Patient
number: 4385 375 473
History
This patient has been referred because he is suffering
from increasing shortness of breath on exertion. The shortness of breath
has been present for about 5 years now, but has been getting gradually
worse.
There is marked variability in his symptoms.
Sometimes he is able to walk only 20 meters before stopping, and is unable to
climb a flight of stairs. However, he is still able to ride his bicycle
as a hobby on weekends, and he thinks his breathing is much better when he is
on holiday.
He has a past history of eczema affecting his hands.
He regularly uses an emollient cream and occasionally 1%
hydrocortisone cream on his hands. He is on no other medications.
He has no known allergies.
Mr Aljboor works Monday to Thursday in a car bodywork
repair shop where his job is re-spraying paint on cars after they are repaired.
He has never smoked. He uses no recreational drugs. He drinks
around 18 units of alcohol per week. He has no pets.
Examination
Temperature:
37.1 °C
Pulse:
90 beats per minute
Blood pressure:
140/64mm Hg
Respiratory rate:
28 breaths
per minute
Oxygen saturations: 98%
on air
Chest expansion is reduced bilaterally.
Percussion is normal.
There is expiratory wheeze throughout the lung fields.
Click on the thumbnail below to open his spirometry
recording

His FEV1 increases by one litre after nebulized
bronchodilator, but his FVC is unchanged.
·
TASK
1. Write a report of the spirometry result in his
medical notes on the paper provided in Question 3 Answer
The structured report of the spirometry should include
measurements of the following items:
·
Forced expiratory volume in one second
·
Forced vital capacity
·
FEV1/FVC ratio
2. Underneath your report in his medical notes write the
likely differential diagnosis/cause of his symptoms considering the clinical
and spirometry findings
From <https://mle.ncl.ac.uk/cases/page/19169/>
Wriske
4
15 January 2021
00:23
Situation
You are a Foundation Year 2 doctor working in General
Practice.
Patient details
Name:
Alda Storey
Date of birth:
22/01/1945
Address:
Apple
Cottage, Hedgerow Lane, Corbridge. NE67 1EE
Patient
number:
444 565 7898
History
Mrs Storey has asked for a repeat prescription for her
regular medications. She has a history of myocardial infarction and of
peripheral vascular disease. Her medications were all started for
secondary prevention of vascular disease.
Atorvastatin 80 mg
once a day
Bisoprolol 5 mg
once a day
Clopidogrel 75 mg
once a day
She came to the surgery last week for some blood tests
to monitor her treatment, and the results are below.
Investigations
Haemoglobin
146 g/L (115-165)
White cell count
8.5 x 109/L (4-11)
Neutrophils
6.0 x 109/L (1.5-7.0)
Platelets
367 x 109/L (150–400)
Sodium
140 mmol/L
(137–144)
Potassium
4.2 mmol/L (3.5–4.9)
Urea
6.4 mmol/L (2.5–7.0)
Creatinine
88 µmol/L (60–110)
Glucose
5.2 mmol/L
Albumin
40 g/L (37–49)
Globulins
26 g/L (24–27)
Total Bilirubin
20 µmol/L (1–22)
Alanine Aminotransferase
160 U/L (5–35)
Alkaline Phosphatase
170U/L (45–105)
Prothrombin Time
13s (11.5–15.5)
Activated Partial Thromboplastin
Time 32s (30–40)
Fibrinogen
5.1g/L
(1.8–5.4)
·
TASK
Please prescribe her medications on the FP10 prescribing
sheet provided in the Question 4 Answer, making any alterations to
the regular prescription which are necessary given the blood results
From <https://mle.ncl.ac.uk/cases/page/19172/>
Cheat sheet
24 December 2020
21:00


24 December 2020
14:03
Myeloma: features
Multiple myeloma is a neoplasm of
the bone marrow plasma cells. The peak incidence is patients aged 60-70 years.
Clinical features
·
bone disease: bone pain, osteoporosis + pathological fractures
(typically vertebral), osteolytic lesions
·
lethargy
·
infection
·
hypercalcaemia (see below)
·
renal failure
·
other features: amyloidosis e.g. Macroglossia, carpal tunnel
syndrome; neuropathy; hyperviscosity
Investigations
·
monoclonal proteins (usually IgG or IgA) in the serum and urine
(Bence Jones proteins)
·
increased plasma cells in the bone marrow
·
historically a skeletal survey has been done to look for bone
lesions. However, whole-body MRI is increasingly used and is now
recommended in the 2016 NICE guidelines
·
X-rays: 'rain-drop skull' (likened to the pattern rain forms
after hitting a surface and splashing, where it leaves a random pattern of dark
spots). Note that a very similar, but subtly different finding is found in
primary hyperparathyroidism - 'pepperpot skull'
The diagnostic criteria for
multiple myeloma requires one major and one minor criteria or three minor
criteria in an individual who has signs or symptoms of multiple myeloma.
Major criteria
·
Plasmacytoma (as demonstrated on evaluation of biopsy specimen)
·
30% plasma cells in a bone marrow sample
·
Elevated levels of M protein in the blood or urine
Minor criteria
·
10% to 30% plasma cells in a bone marrow sample.
·
Minor elevations in the level of M protein in the blood or
urine.
·
Osteolytic lesions (as demonstrated on imaging studies).
·
Low levels of antibodies (not produced by the cancer cells) in
the blood.
Hypercalcaemia in myeloma
·
primary factor: due primarily to increased
osteoclastic bone resorption caused by local cytokines (e.g. IL-1, tumour
necrosis factor) released by the myeloma cells
·
much less common contributing factors: impaired renal function,
increased renal tubular calcium reabsorption and elevated PTH-rP levels
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:03
Direct oral anticoagulants
The table below summaries the three
direct oral anticoagulants (DOACs): dabigatran, rivaroxaban and apixaban.
|
|
Dabigatran |
Rivaroxaban |
Apixaban |
|
UK brand name |
Pradaxa |
Xarelto |
Eliquis |
|
Mechanism of action |
Direct thrombin inhibitor |
Direct factor Xa inhibitor |
Direct factor Xa inhibitor |
|
Route |
Oral |
Oral |
Oral |
|
Excretion |
Majority renal |
Majority liver |
Majority faecal |
|
NICE indications |
Prevention of VTE following hip/knee
surgery Treatment of DVT and PE Prevention of stroke in non-valvular
AF* |
Prevention of VTE following hip/knee
surgery Treatment of DVT and PE Prevention of stroke in non-valvular
AF* |
Prevention of VTE following hip/knee
surgery Treatment of DVT and PE Prevention of stroke in non-valvular
AF* |
|
Reversal |
Idarucizumab |
Andexanet alfa** |
Andexanet alfa** |
*NICE stipulate that certain other
risk factors should be present. These are complicated and differ between the
DOACs but generally require one of the following to be present:
·
prior stroke or transient ischaemic attack
·
age 75 years or older
·
hypertension
·
diabetes mellitus
·
heart failure
**Andexanet alfa is a recombinant
form of human factor Xa protein
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:03
G6PD deficiency
Glucose-6-phosphate dehydrogenase
(G6PD) deficiency is the commonest red blood cell enzyme defect. It is more
common in people from the Mediterranean and Africa and is inherited in an
X-linked recessive fashion. Many drugs can precipitate a crisis as well as
infections and broad (fava) beans
Pathophysiology
·
G6PD is the first step in the pentose phosphate pathway, which
converts glucose-6-phosphate→ 6-phosphogluconolactone
o this reaction also results in
nicotinamide adenine dinucleotide phosphate (NADP) → NADPH
o i.e. glucose-6-phosphate + NADP →
6-phosphogluconolactone + NADPH
·
NADPH is important for converting oxidizied glutathine back to
it's reduced form
·
reduced glutathine protects red blood cells from oxidative
damage by oxidants such as superoxide anion (O2-) and hydrogen peroxide
·
↓ G6PD → ↓ reduced NADPH → ↓ reduced glutathione → increased red
cell susceptibility to oxidative stress
Features
·
neonatal jaundice is often seen
·
intravascular haemolysis
·
gallstones are common
·
splenomegaly may be present
·
Heinz bodies on blood films. Bite and blister cells may also be seen
Diagnosis is made by using a G6PD
enzyme assay
·
levels should be checked around 3
months after an acute episode of hemolysis, RBCs with the most severely reduced G6PD activity will have
hemolysed → reduced G6PD activity → not be measured in the assay → false
negative results
Some drugs causing haemolysis
·
anti-malarials: primaquine
·
ciprofloxacin
·
sulph- group drugs: sulphonamides, sulphasalazine, sulfonylureas
Some drugs thought to be safe
·
penicillins
·
cephalosporins
·
macrolides
·
tetracyclines
·
trimethoprim
Comparing G6PD deficiency to
hereditary spherocytosis:
|
|
|
|
|
|
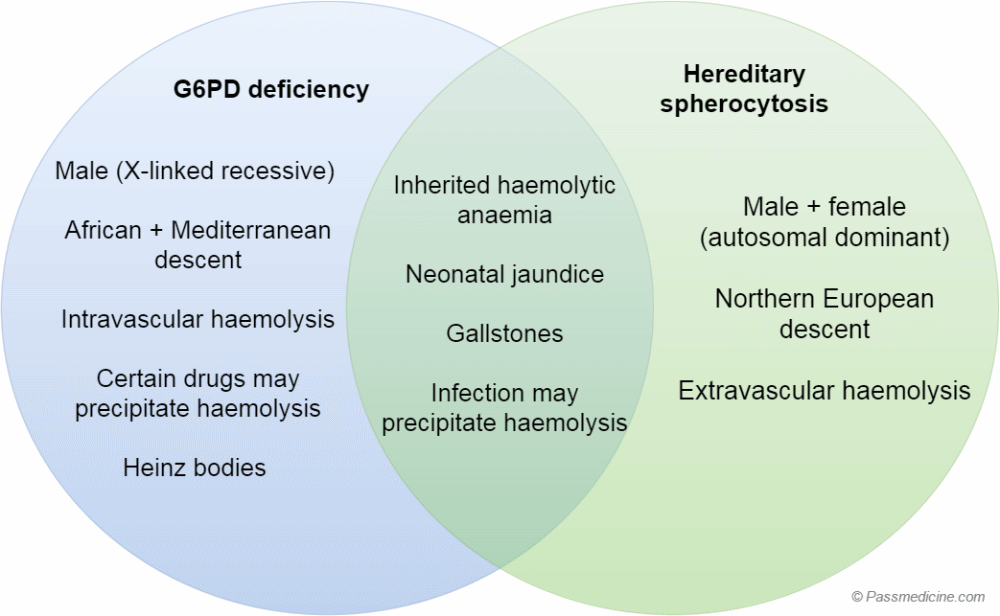
Comparison of G6PD deficiency to hereditary
spherocytosis
|
|
G6PD deficiency |
Hereditary spherocytosis |
|
Gender |
Male (X-linked recessive) |
Male + female (autosomal dominant) |
|
Ethnicity |
African + Mediterranean descent |
Northern European descent |
|
Typical history |
• Neonatal jaundice • Infection/drugs precipitate
haemolysis • Gallstones |
• Neonatal jaundice • Chronic symptoms although haemolytic
crises may be precipitated by infection • Gallstones • Splenomegaly is common |
|
Blood film |
Heinz bodies |
Spherocytes (round, lack of central
pallor) |
|
Diagnostic test |
Measure enzyme activity of G6PD |
Osmotic fragility test |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:03
Iron deficiency anaemia
Iron deficiency anaemia is the most
common anaemia worldwide. Iron is needed to make the haemoglobin in red blood
cells, therefore a deficiency of iron leads to a reduction in red blood
cells/haemoglobin i.e. anaemia. Iron deficiency anaemia has the highest incidence
amongst preschool-age children. The main causes are excessive blood loss,
inadequate dietary intake, poor intestinal absorption and increased iron
requirements.
Epidemiology
·
Globally, iron deficiency is the most common cause of anaemia
·
Preschool-age children have the highest prevalence of iron
deficiency anaemia
Causes
·
Excessive blood loss: blood loss due to menorrhagia is the most
common cause in pre-menopausal women, whereas gastrointestinal bleeding is the
most common cause in men (always suspect colon cancer) and post-menopausal
women.
·
Inadequate dietary intake: as meat is a good source of iron,
vegans and vegetarians are more likely to develop iron deficiency anaemia due
to a lack of meat in their diet. However dark green leafy vegetables are
another good source of iron, therefore people who don’t eat meat can still
receive enough iron through purely dietary sources.
·
Poor intestinal absorption: conditions which affect the small
intestine, such as coeliac disease, can prevent sufficient iron being absorbed.
·
Increased iron requirements: children have increased iron
demands during periods of rapid growth. Women also have increased demands
during pregnancy as the baby will receive their iron supply from the mother. In
addition, an increase in plasma volume during pregnancy causes iron deficiency
anaemia through dilution i.e. the proportion of fluid in comparison to red
blood cells increases.
Features
·
Fatigue
·
Shortness of breath on exertion
·
Palpitations
·
Pallor
·
Nail changes: this includes koilonychia (spoon-shaped nails)
·
Hair loss
·
Atrophic glossitis
·
Post-cricoid webs
·
Angular stomatitis
Investigations
·
Taking a history is the most important step in looking for
potential causes of iron deficiency. It is useful to inquire about: changes in
diet, medication history, menstrual history, weight loss, change in bowel habit
·
Full blood count (FBC) demonstrates
hypochromic microcytic anaemia
·
Serum ferritin this will likely be low, as
serum ferritin correlates with iron stores. However, it is important to
recognise that ferritin can be raised during states of inflammation; so a
raised ferritin does not necessarily rule out iron deficiency anaemia if the is
co-occurring inflammation. For patients with co-occurring inflammatory disease,
other iron studies can be performed.
·
Total iron-binding capacity (TIBC)/transferrin this will be high. A high TIBC reflects low iron stores. . Note that the transferrin saturation will however be low
·
Blood film anisopoikilocytosis (red blood
cells of different sizes and shapes) , target cells, 'pencil' poikilocytes
·
Endoscopy to rule out malignancy, males
and post-menopausal females who present with unexplained iron-deficiency
anaemia should be considered for further gastrointestinal investigations.
Post-menopausal women with a haemoglobin level ≤10 and men with a haemoglobin
level ≤11 should be referred to a gastroenterologist within 2 weeks.
Management
·
The underlying cause of the iron-deficiency anaemia must be
identified and managed. It is particularly important that malignancy has been
excluded by taking an adequate history and appropriate investigations if warranted
·
Oral ferrous sulfate: patients should continue taking iron for 3 months after the iron deficiency has been corrected in order to
replenish iron stores. Common side effects of iron supplementation include
nausea, abdominal pain, constipation, diarrhoea
·
Iron-rich diet: this includes dark-green leafy vegetables, meat,
iron-fortified bread
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:03
Sickle-cell
crises
Sickle cell anaemia is characterised by periods of good health
with intervening crises
A number of types of crises are recognised:
·
thrombotic, 'painful crises'
·
sequestration
·
acute chest syndrome
·
aplastic
·
haemolytic
Thrombotic crises
·
also known as painful crises or vaso-occlusive crises
·
precipitated by infection, dehydration,
deoxygenation
·
painful vaso-occlusive crises should be diagnosed
clinically - there isn't one test that can confirm them although tests may
be done to exclude other complications
·
infarcts occur in various organs including the bones (e.g.
avascular necrosis of hip, hand-foot syndrome in children, lungs, spleen and
brain
Sequestration crises
·
sickling within organs such as the spleen or lungs causes
pooling of blood with worsening of the anaemia
Acute chest syndrome
·
dyspnoea, chest pain, pulmonary infiltrates, low pO2
·
the most common cause of death after childhood
Aplastic crises
·
caused by infection with parvovirus
·
sudden fall in haemoglobin
Haemolytic crises
·
rare
·
fall in haemoglobin due an increased rate of haemolysis
From <https://www.passmedicine.com/review/textbook.php?s=#>
Acute chest crisis management:
·
Hydration
·
O2 therapy
·
Broad spectrum IV Abx
·
Pain relief
·
Incentive spirometry (if able)
·
Bronchodilators is element of bronchospasm
·
Transfusion
either top-up or exchange
Need to be aware of patients’ baseline
·
Early involvement of haematology and
critical care
24 December 2020
14:03
Von Willebrand's disease
Von Willebrand's disease is the most common inherited bleeding
disorder. The majority of cases are inherited in an autosomal dominant fashion* and characteristically behaves like a platelet disorder
i.e. epistaxis and menorrhagia are common whilst haemoarthroses and muscle
haematomas are rare
Role of von Willebrand factor
·
large glycoprotein which forms massive multimers up to 1,000,000
Da in size
·
promotes platelet adhesion to damaged endothelium
·
carrier molecule for factor VIII
Types
·
type 1: partial reduction in vWF (80% of patients)
·
type 2*: abnormal form of vWF
·
type 3**: total lack of vWF (autosomal recessive)
Investigation
·
prolonged bleeding time
·
APTT may be prolonged
·
factor VIII levels may be moderately reduced
·
defective platelet aggregation with ristocetin
Management
·
tranexamic acid for mild bleeding
·
desmopressin (DDAVP): raises levels of vWF by inducing release
of vWF from Weibel-Palade bodies in endothelial cells
·
factor VIII concentrate
*type 2A VWD is caused by defective
platelet adhesion due to decreased high molecular weight VWF multimers (i.e.
the VWF protein is too small). Type 2B is characterised by a pathological
increase of VWF-platelet interaction. Type 2M is caused by a decrease in VWF-platelet
interaction (not related to loss of high molecular weight multimers). Type 2N
is caused by abnormal binding of the VWF to Factor VIII. There is no clear
correlation between symptomatic presentation and type of VWD however common
themes amongst patients include excessive mucocutaneous bleeding, bruising in
the absence of trauma and menorrhagia in females.
**type 3 von Willebrand's disease
(most severe form) is inherited as an autosomal recessive trait. Around 80% of
patients have type 1 disease
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:03
Blood products: CMV negative and irradiated blood
Cytomegalovirus (CMV) is
transmitted in leucocytes. As most blood products (except granulocyte
transfusions) are now leucocyte depleted CMV negative products are rarely
required.
Irradiated blood products are depleted of T-lymphocytes and used to avoid transfusion-associated graft versus host disease (TA-GVHD) caused by engraftment of viable donor T lymphocytes.
The table below shows the
indications for CMV and irradiated blood:
|
Situation |
CMV negative |
Irradiated |
|
Granulocyte transfusions |
✓ |
✓ |
|
Intra-uterine transfusions |
✓ |
✓ |
|
Neonates up to 28 days post expected
date of delivery |
✓ |
✓ |
|
Pregnancy: Elective transfusions during
pregnancy (not during labour or delivery) |
✓ |
|
|
Bone marrow / stem cell transplants |
|
✓ |
|
Immunocompromised (e.g. chemotherapy or
congenital) |
|
✓ |
|
Patients with/previous Hodgkins Disease |
|
✓ |
|
HIV |
|
|
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Chronic myeloid leukaemia
The Philadelphia chromosome is present in more than 95% of patients with chronic myeloid
leukaemia (CML). It is due to a translocation
between the long arm of chromosome 9 and 22 - t(9:22)(q34; q11). This results in part of the ABL proto-oncogene from chromosome
9 being fused with the BCR gene from chromosome 22. The resulting BCR-ABL gene
codes for a fusion protein which has tyrosine kinase activity in excess of
normal
Presentation (60-70 years)
·
anaemia: lethargy
·
weight loss and sweating are common
·
splenomegaly may be marked → abdo discomfort
·
an increase in granulocytes at different stages of maturation
+/- thrombocytosis
·
decreased leukocyte alkaline phosphatase
·
may undergo blast transformation (AML in 80%, ALL in 20%)
Management
·
imatinib is now considered first-line treatment
·
hydroxyurea
·
interferon-alpha
·
allogenic bone marrow transplant
Imatinib
·
inhibitor of the tyrosine kinase associated with the BCR-ABL defect
·
very high response rate in chronic phase CML
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Hereditary spherocytosis
Basics
·
most common hereditary haemolytic anaemia in people of northern
European descent
·
autosomal dominant defect of red blood cell cytoskeleton
·
the normal biconcave disc shape is replaced by a sphere-shaped
red blood cell
·
red blood cell survival reduced as destroyed by the spleen
Presentation
·
failure to thrive
·
jaundice, gallstones
·
splenomegaly
·
aplastic crisis precipitated by parvovirus infection
·
degree of haemolysis variable
·
MCHC elevated
Diagnosis
·
the osmotic fragility test was previously the recommend
investigation of choice. However, it is now deemed unreliable and is no longer
recommended
·
the British Journal of Haematology (BJH) guidelines state that 'patients with a family history of HS, typical clinical features and
laboratory investigations (spherocytes, raised mean corpuscular haemoglobin
concentration[MCHC], increase in reticulocytes) do not require any additional
tests
·
if the diagnosis is equivocal the BJH recommend the
cryohaemolysis test and EMA binding
·
for atypical presentations electrophoresis analysis of
erythrocyte membranes is the method of choice
Management
·
acute haemolytic crisis:
o treatment is generally supportive
o transfusion if necessary
·
longer term treatment:
o folate replacement
o splenectomy
Comparing G6PD deficiency to
hereditary spherocytosis:
|
|
|
|
|
|
Comparison of G6PD deficiency to hereditary
spherocytosis
|
|
G6PD deficiency |
Hereditary spherocytosis |
|
Gender |
Male (X-linked recessive) |
Male + female (autosomal dominant) |
|
Ethnicity |
African + Mediterranean descent |
Northern European descent |
|
Typical history |
• Neonatal jaundice • Infection/drugs precipitate
haemolysis • Gallstones |
• Neonatal jaundice • Chronic symptoms although haemolytic
crises may be precipitated by infection • Gallstones • Splenomegaly is common |
|
Blood film |
Heinz bodies |
Spherocytes (round, lack of central
pallor) |
|
Diagnostic test |
Measure enzyme activity of G6PD |
EMA binding test |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Platelet transfusion: active bleeding
Active bleeding
Offer platelet transfusions to
patients with a platelet count of <30 x 10 9 with
clinically significant bleeding (World Health organisation bleeding grade 2-
e.g. haematemesis, melaena, prolonged epistaxis)
Platelet thresholds for transfusion
are higher (maximum < 100 x 10 9) for patients with severe bleeding (World Health organisation
bleeding grades 3&4), or bleeding at critical sites, such as the CNS.
It should be noted that platelet transfusions have the
highest risk of bacterial contamination compared to other types of blood
product.
Pre-invasive procedure
(prophylactic)
Platelet transfusion for
thrombocytopenia before surgery/ an invasive procedure. Aim for plt levels of:
·
> 50×109/L for most patients
·
50-75×109/L if high risk of bleeding
·
>100×109/L if surgery at critical site
If no active bleeding or planned
invasive procedure
A threshold of 10 x 109 except where
platelet transfusion is contradindicated or there are alternative treatments
for their condition
For example, do not perform
platelet transfusion for any of the following conditions:
·
Chronic bone marrow failure
·
Autoimmune thrombocytopenia
·
Heparin-induced thrombocytopenia, or
·
Thrombotic thrombocytopenic purpura.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Sickle-cell anaemia
Sickle-cell anaemia is an autosomal recessive condition that results for synthesis of an abnormal haemoglobin
chain termed HbS. It is more common in people of African descent as the
heterozygous condition offers some protection against malaria. Around 10% of UK
Afro-Caribbean's are carriers of HbS (i.e. heterozygous). Such people are only
symptomatic if severely hypoxic.
Symptoms in homozygotes don't tend
to develop until 4-6 months when the abnormal HbSS molecules take over from
fetal haemoglobin.
Pathophysiology
·
polar amino acid glutamate is substituted by non-polar valine in
each of the two beta chains (codon 6). This decreases the water solubility of
deoxy-Hb
·
in the deoxygenated state the HbS molecules polymerise and cause
RBCs to sickle
·
HbAS patients sickle at p02 2.5 - 4 kPa, HbSS patients at p02 5
- 6 kPa
·
sickle cells are fragile and haemolyse; they block small blood
vessels and cause infarction
Investigations
·
definitive diagnosis of sickle cell disease is by haemoglobin electrophoresis
From <https://www.passmedicine.com/review/textbook.php?s=#>

24 December 2020
14:04
Venous
thromboembolism: risk factors
Common predisposing factors include malignancy, pregnancy and
the period following an operation. The comprehensive list below is partly based
on the 2010 SIGN venous thromboembolism (VTE) guidelines:
General
·
increased risk with advancing age
·
obesity
·
family history of VTE
·
pregnancy (especially puerperium)
·
immobility
·
hospitalisation
·
anaesthesia
·
central venous catheter: femoral >> subclavian
Underlying conditions
·
malignancy
·
thrombophilia: e.g. Activated protein C resistance, protein C
and S deficiency
·
heart failure
·
antiphospholipid syndrome
·
Behcet's
·
polycythaemia
·
nephrotic syndrome
·
sickle cell disease
·
paroxysmal nocturnal haemoglobinuria
·
hyperviscosity syndrome
·
homocystinuria
Medication
·
combined oral contraceptive pill: 3rd
generation more than 2nd generation
·
hormone replacement therapy: the risk of VTE is higher in women
taking oestrogen + progestogen preparations compared to those taking
oestrogen-only preparations
·
raloxifene and tamoxifen
·
antipsychotics (especially olanzapine) have recently been shown
to be a risk factor
It should be remembered however that around 40% of patients
diagnosed with a PE have no major risk factors.
From <https://www.passmedicine.com/review/textbook.php?s=#>
·
Congenital thrombophilias (i.e
antithrombin deficiency, protein Cor S deficiency, prothrombin gene mutaions)
·
Acquired: Antiphospholipid syndrome,
Myeloproliferative conditions
·
Inflammatory states: malignancy, surgery
·
Poor mobility
·
Compression
24 December 2020
14:04
Vitamin B12 deficiency
Vitamin B12 is mainly used in the
body for red blood cell development and also maintenance of the nervous system.
It is absorbed after binding to intrinsic factor (secreted from parietal cells
in the stomach) and is actively absorbed in the terminal ileum. A small amount of vitamin B12 is passively absorbed without
being bound to intrinsic factor.
Causes of vitamin B12 deficiency
·
pernicious anaemia: most common cause
·
post gastrectomy
·
vegan diet or a poor diet
·
disorders/surgery of terminal ileum (site of absorption)
o Crohn's: either diease activity or
following ileocaecal resection
·
metformin (rare)
Features of vitamin B12 deficiency
·
macrocytic anaemia
·
sore tongue and mouth
·
neurological symptoms
o the dorsal column is usually
affected first (joint position, vibration) prior to distal paraesthesia
·
neuropsychiatric symptoms: e.g. mood disturbances
Management
·
if no neurological involvement 1 mg of IM hydroxocobalamin 3
times each week for 2 weeks, then once every 3 months
·
if a patient is also deficient in folic acid then it is
important to treat the B12 deficiency
first to avoid
precipitating subacute combined degeneration of the cord
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Blood products: red bloods cells
NICE published guidelines on the
use of blood products in 2015.
They recommended the following
thresholds for transfusion:
|
|
Patients without ACS |
Patients with ACS |
|
Transfusion threshold |
70 g/L |
80 g/L |
|
Target after transfusion |
70-90 g/L |
80-100 g/L |
(ACS = acute coronary syndrome)
Please note that these thresholds
should not be used in patients with ongoing major haemorrhage or patients who
require regular blood transfusions for chronic anaemia.
Practical points
·
red blood cells should be stored at 4°C prior to infusion
·
in a non-urgent scenario, a unit of RBC is usually transfused
over 90-120 minutes
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Chronic lymphocytic leukaemia: features and
investigation
Chronic lymphocytic leukaemia (CLL)
is caused by a monoclonal
proliferation of well-differentiated lymphocytes which are almost always
B-cells (99%). It is the most common form of leukaemia seen
in adults.
Features
·
often none: may be picked up by an incidental finding of
lymphocytosis
·
constitutional: anorexia, weight loss
·
bleeding, infections
·
lymphadenopathy more marked than chronic myeloid leukaemia
Investigations
·
full blood count:
o lymphocytosis
o anaemia
·
blood film: smudge cells (also known as smear cells)
·
immunophenotyping is the key investigation
|
|
|
|
Image
sourced from Wikipedia |
|
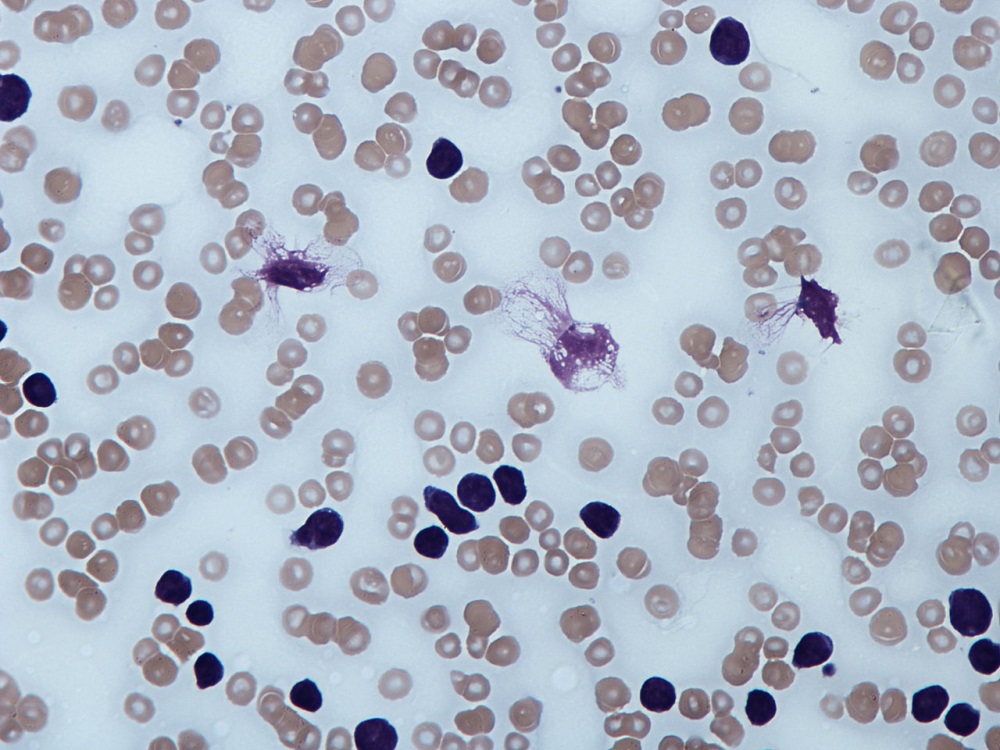
Peripheral blood film showing smudge B cells
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Hodgkin's lymphoma
Hodgkin's lymphoma is a malignant
proliferation of lymphocytes characterised by the presence of the
Reed-Sternberg cell. It has a bimodal age distributions being most common in
the third and seventh decades
Features
·
lymphadenopathy (75%) - painless, non-tender, asymmetrical
·
systemic (25%): weight loss, pruritus, night sweats, fever
(Pel-Ebstein)
·
alcohol pain in HL
·
normocytic anaemia, eosinophilia
·
LDH raised
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Polycythaemia vera: features
Polycythaemia vera (previously
called polycythaemia rubra vera) is a myeloproliferative disorder caused by
clonal proliferation of a marrow stem cell leading to an increase in red cell
volume, often accompanied by overproduction of neutrophils and platelets. It
has recently been established that a mutation in JAK2 is present in approximately 95% of patients with
polycythaemia vera and this has resulted in
significant changes to the diagnostic criteria. The incidence of polycythaemia
vera peaks in the sixth decade.
Features
·
hyperviscosity
·
pruritus, typically after a hot bath
·
splenomegaly
·
haemorrhage (secondary to abnormal platelet function)
·
plethoric appearance
·
hypertension in a third of patients
·
low ESR
Following history and examination,
the British Committee for Standards in Haematology (BCSH) recommend the
following tests are performed
·
full blood count/film (raised haematocrit; neutrophils,
basophils, platelets raised in half of patients)
·
JAK2 mutation
·
serum ferritin
·
renal and liver function tests
If the JAK2 mutation is negative
and there is no obvious secondary causes the BCSH suggest the following tests:
·
red cell mass
·
arterial oxygen saturation
·
abdominal ultrasound
·
serum erythropoietin level
·
bone marrow aspirate and trephine
·
cytogenetic analysis
·
erythroid burst-forming unit (BFU-E) culture
Other features that may be seen in
PRV include a low ESR and a raised leukocyte alkaline phosphatase
The diagnostic criteria for
polycythaemia vera have recently been updated by the BCSH. This replaces the
previous polycythaemia vera Study Group criteria.
JAK2-positive polycythaemia vera -
diagnosis requires both criteria to be present
|
Criteria |
Notes |
|
A1 |
High haematocrit (>0.52 in men,
>0.48 in women) OR raised red cell mass (>25% above predicted) |
|
A2 |
Mutation in JAK2 |
JAK2-negative PRV - diagnosis
requires A1 + A2 + A3 + either another A or two B criteria
|
Criteria |
Notes |
|
A1 |
Raised red cell mass (>25% above
predicted) OR haematocrit >0.60 in men, >0.56 in women |
|
A2 |
Absence of mutation in JAK2 |
|
A3 |
No cause of secondary erythrocytosis |
|
A4 |
Palpable splenomegaly |
|
A5 |
Presence of an acquired genetic
abnormality (excluding BCR-ABL) in the haematopoietic cells |
|
B1 |
Thrombocytosis (platelet count >450
* 109/l) |
|
B2 |
Neutrophil leucocytosis (neutrophil
count > 10 * 109/l in non-smokers; > 12.5*109/l in smokers) |
|
B3 |
Radiological evidence of splenomegaly |
|
B4 |
Endogenous erythroid colonies or low
serum erythropoietin |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Post-thrombotic syndrome
It is increasingly recognised that
patients may develop complications following a DVT. Venous outflow obstruction
and venous insufficiency result in chronic venous hypertension. The resulting
clinical syndrome is known as post-thrombotic syndrome. The following features
maybe seen:
·
painful, heavy calves
·
pruritus
·
swelling
·
varicose veins
·
venous ulceration
Compression stockings have in the
past been offered to patients with deep vein thrombosis to help reduce the risk
of post-thrombotic syndrome.
However, Clinical Knowledge
Summaries now state the following:
Do not offer elastic graduated compression stockings to prevent
post-thrombotic syndrome or VTE recurrence after a proximal DVT. This
recommendation does not cover the use of elastic stockings for the management
of leg symptoms after DVT.
However, once post-thrombotic
syndrome has developed compression stockings are a recommended treatment. Other
recommendations including keeping the leg elevated.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Thrombophilia: causes
Inherited
Gain of function polymorphisms
·
factor V Leiden (activated protein C resistance): most common cause of
thrombophilia
·
prothrombin gene mutation: second most common cause
Deficiencies of naturally occurring
anticoagulants
·
antithrombin III deficiency
·
protein C deficiency
·
protein S deficiency
The table below shows the
prevalence and relative risk of venous thromboembolism (VTE) of the different
inherited thrombophilias:
|
Condition |
Prevalence |
Relative risk of VTE |
|
Factor V Leiden (heterozygous) |
5% |
4 |
|
Factor V Leiden (homozygous) |
0.05% |
10 |
|
Prothrombin gene mutation
(heterozygous) |
1.5% |
3 |
|
Protein C deficiency |
0.3% |
10 |
|
Protein S deficiency |
0.1% |
5-10 |
|
Antithrombin III deficiency |
0.02% |
10-20 |
Acquired
Antiphospholipid syndrome
Drugs
·
the combined oral contraceptive pill
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:04
Tumour lysis syndrome
Tumour lysis syndrome (TLS) is a
potentially deadly condition related to the treatment of high-grade lymphomas
and leukaemias. It can occur in the absence of chemotherapy but is usually
triggered by the introduction of combination chemotherapy. On occasion, it can
occur with steroid treatment alone. Awareness of the condition is critical as
prophylactic medication can be given to prevent the potentially deadly effects
of tumour cell lysis.
Patients at high risk of TLS should
be given IV
allopurinol or IV rasburicase immediately prior to and during the
first days of chemotherapy. Rasburicase is a recombinant version of urate
oxidase, an enzyme that metabolizes uric acid to allantoin. Allantoin is much more water-soluble than uric acid and is,
therefore, more easily excreted by the kidneys. Patients in lower-risk groups
should be given oral allopurinol during chemotherapy cycles in an attempt to
avoid the condition. Rasburicase
and allopurinol should not be given together in the management of tumour lysis syndrome as this reduces the
effect of rasburicase.
TLS occurs from the breakdown of
the tumour cells and the subsequent release of chemicals from the cell. It
leads to a
high potassium and high phosphate level in the presence of a low calcium. It should be suspected in any patient presenting with an acute
kidney injury in the presence of a high phosphate and high uric acid level.
From 2004 TLS has been graded using
the Cairo-Bishop scoring system -
Laboratory tumor lysis syndrome:
abnormality in two or more of the following, occurring within three days before
or seven days after chemotherapy.
·
uric acid > 475umol/l or 25% increase
·
potassium > 6 mmol/l or 25% increase
·
phosphate > 1.125mmol/l or 25% increase
·
calcium < 1.75mmol/l or 25% decrease
Clinical tumor lysis syndrome:
laboratory tumour
lysis syndrome plus one or more of the following:
·
increased serum creatinine (1.5 times upper limit of normal)
·
cardiac arrhythmia or sudden death
·
seizure
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Abnormal coagulation
|
Cause |
Factors affected |
|
Heparin |
Prevents activation factors 2,9,10,11 |
|
Warfarin |
Affects synthesis of factors 2,7,9,10 |
|
DIC |
Factors 1,2,5,8,11 |
|
Liver disease |
Factors 1,2,5,7,9,10,11 |
Interpretation blood clotting test
results
|
Disorder |
APTT |
PT |
Bleeding time |
|
Haemophilia |
Increased |
Normal |
Normal |
|
von Willebrand's disease |
Increased |
Normal |
Increased |
|
Vitamin K deficiency |
Increased |
Increased |
Normal |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Antiphospholipid syndrome: pregnancy
Antiphospholipid syndrome is an
acquired disorder characterised by a predisposition to both venous and arterial
thromboses, recurrent fetal loss and thrombocytopenia. It may occur as a
primary disorder or secondary to other conditions, most commonly systemic lupus
erythematosus (SLE)
In pregnancy the following
complications may occur:
·
recurrent miscarriage
·
IUGR
·
pre-eclampsia
·
placental abruption
·
pre-term delivery
·
venous thromboembolism
Management
·
low-dose aspirin should be commenced once the pregnancy is confirmed on
urine testing
·
low molecular weight heparin once a fetal heart is seen on
ultrasound. This is usually discontinued at 34 weeks gestation
·
these interventions increase the live birth rate seven-fold
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Beta-thalassaemia trait
The thalassaemias are a group of
genetic disorders characterised by a reduced production rate of either alpha or
beta chains. Beta-thalassaemia trait is an autosomal recessive condition
characterised by a mild hypochromic, microcytic anaemia. It is usually asymptomatic
Features
·
mild hypochromic, microcytic anaemia - microcytosis
is characteristically disproportionate to the anaemia
·
HbA2 raised (> 3.5%)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Blood products
Whole blood fractions
|
Fraction |
Key points |
|
Packed red cells |
Used for transfusion in chronic anaemia
and cases where infusion of large volumes of fluid may result in
cardiovascular compromise. Product obtained by centrifugation of whole blood. |
|
Platelet rich plasma |
Usually administered to patients who
are thrombocytopaenic and are bleeding or require surgery. It is obtained by
low speed centrifugation. |
|
Platelet concentrate |
Prepared by high speed centrifugation
and administered to patients with thrombocytopaenia. |
|
Fresh frozen plasma |
·
Prepared from single units of blood. ·
Contains clotting factors, albumin and
immunoglobulin. ·
Unit is usually 200 to 250ml. ·
Usually used in correcting clotting deficiencies in
patients with hepatic synthetic failure who are due to undergo surgery. ·
Usual dose is 12-15ml/Kg-1. ·
It should not be used as first line therapy for
hypovolaemia. |
|
Cryoprecipitate |
·
Formed from supernatant of FFP. ·
Rich source of Factor VIII and fibrinogen. ·
Allows large concentration of factor VIII to be
administered in small volume. |
|
SAG-Mannitol Blood |
Removal of all plasma from a blood unit
and substitution with: ·
Sodium chloride ·
Adenine ·
Anhydrous glucose ·
Mannitol Up to 4 units of SAG M Blood may be
administered. Thereafter whole blood is preferred. After 8 units, clotting
factors and platelets should be considered. |
Cell saver devices
These collect patients own blood
lost during surgery and then re-infuse it. There are two main types:
·
Those which wash the blood cells prior to re-infusion. These are
more expensive to purchase and more complicated to operate. However, they
reduce the risk of re-infusing contaminated blood back into the patient.
·
Those which do not wash the blood prior to re-infusion.
Their main advantage is that they
avoid the use of infusion of blood from donors into patients and this may
reduce risk of blood borne infection. It may be acceptable to Jehovah's
witnesses. It is contraindicated in malignant disease for risk of facilitating
disease dissemination.
Blood products used in warfarin
reversal
In some surgical patients the use
of warfarin can pose specific problems and may require the use of specialised
blood products
Immediate or urgent surgery in
patients taking warfarin(1) (2):
1. Stop warfarin
2. Vitamin K (reversal within 4-24
hours)
-IV takes 4-6h to work (at least
5mg)
-Oral can take 24 hours to be
clinically effective
3. Fresh frozen plasma
Used less commonly now as 1st line
warfarin reversal
-30ml/kg-1
-Need to give at least 1L fluid in
70kg person (therefore not appropriate in fluid overload)
-Need blood group
-Only use if human prothrombin
complex is not available
4. Human Prothrombin Complex
(reversal within 1 hour)
-Bereplex 50 u/kg
-Rapid action but factor 6 short
half life, therefore give with vitamin K
References
1. Dentali, F., C. Marchesi, et al.
(2011). 'Safety of prothrombin complex concentrates for rapid anticoagulation
reversal of vitamin K antagonists. A meta-analysis.' Thromb Haemost 106(3):
429-438.
2. http://www.transfusionguidelines.org/docs/pdfs/bbt-03warfarin-reversal-flowchart-2006.pdf
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Burkitt's lymphoma
Burkitt's lymphoma is a high-grade
B-cell neoplasm. There are two major forms:
·
endemic (African) form: typically involves maxilla or mandible
·
sporadic form: abdominal (e.g. ileo-caecal) tumours are the most
common form. More common in patients with HIV
Burkitt's lymphoma is associated
with the c-myc
gene translocation, usually t(8:14). The Epstein-Barr
virus (EBV) is strongly implicated in the
development of the African form of Burkitt's lymphoma and to a lesser extent
the sporadic form.
Microscopy findings
·
'starry sky' appearance: lymphocyte sheets interspersed with
macrophages containing dead apoptotic tumour cells
Management is with chemotherapy.
This tends to produce a rapid response which may cause 'tumour lysis syndrome'. Rasburicase (a recombinant version of urate oxidase, an
enzyme which catalyses the conversion of uric acid to allantoin*) is often
given before the chemotherapy to reduce the risk of this occurring.
Complications of tumour lysis syndrome include:
·
hyperkalaemia
·
hyperphosphataemia
·
hypocalcaemia
·
hyperuricaemia
·
acute renal failure
*allantoin is 5-10 times more
soluble than uric acid, so renal excretion is more effective
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Cryoprecipitate
·
Blood product made from plasma
·
Usually transfused as 6 unit pool
·
Indications include massive haemorrhage and uncontrolled
bleeding due to haemophilia
Composition
|
Agent |
Quantity |
|
Factor VIII |
100IU |
|
Fibrinogen |
250mg |
|
von Willebrand factor |
Variable |
|
Factor XIII |
Variable |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Disseminated intravascular coagulation - diagnosis
Under homeostatic conditions,
coagulation and fibrinolysis are coupled. The activation of the coagulation
cascade yields thrombin that converts fibrinogen to fibrin; the stable fibrin
clot being the final product of hemostasis. The fibrinolytic system breaks down
fibrinogen and fibrin. Activation of the fibrinolytic system generates plasmin
(in the presence of thrombin), which is responsible for the lysis of fibrin
clots. The breakdown of fibrinogen and fibrin results in polypeptides (fibrin
degradation products). In a state of homeostasis, the presence of plasmin is
critical, as it is the central proteolytic enzyme of coagulation and is also
necessary for fibrinolysis.
In DIC, the processes of
coagulation and fibrinolysis are dysregulated, and the result is widespread
clotting with resultant bleeding. Regardless of the triggering event of DIC,
once initiated, the pathophysiology of DIC is similar in all conditions. One
critical mediator of DIC is the release of a transmembrane glycoprotein (tissue
factor =TF). TF is present on the surface of many cell types (including
endothelial cells, macrophages, and monocytes) and is not normally in contact
with the general circulation, but is exposed to the circulation after vascular
damage. For example, TF is released in response to exposure to cytokines
(particularly interleukin 1), tumour necrosis factor, and endotoxin. This plays
a major role in the development of DIC in septic conditions. TF is also
abundant in tissues of the lungs, brain, and placenta. This helps to explain
why DIC readily develops in patients with extensive trauma. Upon activation, TF
binds with coagulation factors that then triggers the extrinsic pathway (via
Factor VII) which subsequently triggers the intrinsic pathway (XII to XI to IX)
of coagulation.
Causes of DIC
·
sepsis
·
trauma
·
obstetric complications e.g. aminiotic fluid embolism or
hemolysis, elevated liver function tests, and low platelets (HELLP syndrome)
·
malignancy
Diagnosis
A typical blood picture includes:
·
low platelets
·
prolonged APTT, prothrombin and bleeding time
·
fibrin degradation products are often raised
·
schistocytes due to microangiopathic haemolytic anaemia
|
Disorder |
Prothrombin time |
APTT |
Bleeding time |
Platelet count |
|
Warfarin administration |
Prolonged |
Normal |
Normal |
Normal |
|
Aspirin administration |
Normal |
Normal |
Prolonged |
Normal |
|
Heparin |
Often normal (may be prolonged) |
Prolonged |
Normal |
Normal |
|
DIC |
Prolonged |
Prolonged |
Prolonged |
Low |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Factor V Leiden
Factor V Leiden (activated protein
C resistance) is the most common inherited thrombophilia, being present in
around 5% of the UK population.
It is due to a gain of function
mutation in the Factor V Leiden protein. The result of the mis-sense mutation
is that activated factor V (a clotting factor) is inactivated 10 times more
slowly by activated protein C than normal. This explains the alternative name
for factor V Leiden of activated protein C resistance,
Heterozygotes have a 4-5 fold risk
of venous thrombosis. Homozygotes have a 10 fold risk of venous thrombosis but
the prevalence is much lower at 0.05%.
Screening for factor V Leiden is
not recommended, even after a venous thromboembolism. The logic behind this is
that a previous thromboembolism itself is a risk factor for further events and
this should dictate specific management in the future, rather than the
particular thrombophilia identified.
The table below shows the
prevalence and relative risk of venous thromboembolism (VTE) of the different
inherited thrombophilias:
|
Condition |
Prevalence |
Relative risk of VTE |
|
Factor V Leiden (heterozygous) |
5% |
4 |
|
Factor V Leiden (homozygous) |
0.05% |
10 |
|
Prothrombin gene mutation
(heterozygous) |
1.5% |
3 |
|
Protein C deficiency |
0.3% |
10 |
|
Protein S deficiency |
0.1% |
5-10 |
|
Antithrombin III deficiency |
0.02 |
10-20 |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Haemophilia
Haemophilia is a X-linked recessive
disorder of coagulation. Up to 30% of patients have no family history of the
condition. Haemophilia A is due to a deficiency of factor VIII whilst in
haemophilia B (Christmas disease) there is a lack of factor IX
Features
·
haemoarthroses, haematomas
·
prolonged bleeding after surgery or trauma
Blood tests
·
prolonged APTT
·
bleeding time, thrombin time, prothrombin time normal
Up to 10-15% of patients with
haemophilia A develop antibodies to factor VIII treatment.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Immune thrombocytopenia (ITP) in adults
Immune (or idiopathic)
thrombocytopenic purpura (ITP) is an immune-mediated reduction in the platelet
count. Antibodies are directed against the glycoprotein IIb/IIIa or Ib-V-IX
complex.
Children with ITP usually have an
acute thrombocytopenia that may follow infection or vaccination. In contract,
adults tend to have a more chronic condition.
ITP in adults
Epidemiology
·
more common in older females
Presentation
·
may be detected incidentally following routine bloods
·
symptomatic patients may present with
o petichae, purpura
o bleeding (e.g. epistaxis)
o catastrophic bleeding (e.g.
intracranial) is not a common presentation
Management
·
first-line treatment for ITP is oral
prednisolone
·
pooled normal human immunoglobulin (IVIG) may also be used
·
splenectomy is now less commonly used
Evan's syndrome
·
ITP in association with autoimmune haemolytic anaemia (AIHA)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Macrocytic anaemia
Macrocytic anaemia can be divided
into causes associated with a megaloblastic bone marrow and those with a
normoblastic bone marrow
|
Megaloblastic
causes |
Normoblastic causes |
|
·
vitamin B12 deficiency ·
folate deficiency |
·
alcohol ·
liver disease ·
hypothyroidism ·
pregnancy ·
reticulocytosis ·
myelodysplasia ·
drugs: cytotoxics |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:05
Management of suspected haematological malignancy in
young people
Any of the following features in a
person aged 0-24 years should prompt a very urgent full blood count (within 48
hours) to investigate for leukaemia:
·
Pallor
·
Persistent fatigue
·
Unexplained fever
·
Unexplained persistent infections
·
Generalised lymphadenopathy
·
Persistent or unexplained bone pain
·
Unexplained bruising
·
Unexplained bleeding
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Myelofibrosis
Overview
·
a myeloproliferative disorder
·
thought to be caused by hyperplasia of abnormal megakaryocytes
·
the resultant release of platelet derived growth factor is
thought to stimulate fibroblasts
·
haematopoiesis develops in the liver and spleen
Features
·
e.g. elderly person with symptoms of anaemia e.g. fatigue (the
most common presenting symptom)
·
massive splenomegaly
·
hypermetabolic symptoms: weight loss, night sweats etc
Laboratory findings
·
anaemia
·
high WBC and platelet count early in the disease
·
'tear-drop' poikilocytes on blood film
·
unobtainable bone marrow biopsy - 'dry tap' therefore trephine
biopsy needed
·
high urate and LDH (reflect increased cell turnover)
|
|
|
|
|
|
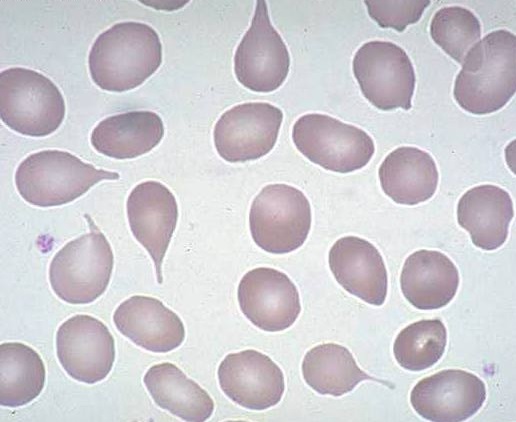
Blood film showing the typical 'tear-drop' poikilocytes
of myelofibrosis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Neutropenic sepsis
Neutropenic sepsis is a relatively
common complication of cancer therapy, usually as a consequence of
chemotherapy. It most commonly occurs 7-14 days after chemotherapy. It may be
defined as a neutrophil count of < 0.5 * 109 in a patient
who is having anticancer treatment and has one of the following:
·
a temperature higher than 38ºC or
·
other signs or symptoms consistent with clinically significant
sepsis
Prophylaxis
·
if it is anticipated that patients are likely to have a
neutrophil count of < 0.5 * 109 as a consequence
of their treatment they should be offered a fluoroquinolone
Management
·
antibiotics must be started immediately, do not wait for the WBC
·
NICE recommends starting empirical antibiotic therapy with piperacillin with tazobactam (Tazocin) immediately
·
many units add vancomycin if the patient has central venous
access but NICE do not support this approach
·
following this initial treatment patients are usually assessed
by a specialist and risk-stratified to see if they may be able to have
outpatient treatment
·
if patients are still febrile and unwell after 48 hours an
alternative antibiotic such as meropenem is often prescribed +/- vancomycin
·
if patients are not responding after 4-6 days the Christie
guidelines suggest ordering investigations for fungal infections (e.g. HRCT),
rather than just starting therapy antifungal therapy blindly
·
there may be a role for G-CSF in selected patients
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Polycythaemia
Polycythaemia may be relative,
primary (polycythaemia rubra vera) or secondary
Relative causes
·
dehydration
·
stress: Gaisbock syndrome
Primary
·
polycythaemia rubra vera
Secondary causes
·
COPD
·
altitude
·
obstructive sleep apnoea
·
excessive erythropoietin: cerebellar haemangioma, hypernephroma,
hepatoma, uterine fibroids*
To differentiate between true
(primary or secondary) polycythaemia and relative polycythaemia red cell mass
studies are sometimes used. In true polycythaemia the total red cell mass in
males > 35 ml/kg and in women > 32 ml/kg
*uterine fibroids may cause menorrhagia
which in turn leads to blood loss - polycythaemia is rarely a clinical problem
From <https://www.passmedicine.com/review/textbook.php?s=#>
Whole
blood viscosity is dependent upon Hct, red cell deformability and plasma
viscosity.
pt
should be venesected on a weekly basis initially to a Hct of around 0.45.
An
elevated Hct is associated particularly with an increased risk of cerebro
vascular accident and myocardial infarction.
The
degree of elevation of his platelet count and his history of TIA’s make
anti-platelet therapy with Aspirin and treatment to reduce his platelet count
(cyto-reductive therapy e.g. interferon or hydroxycarbamide) into the normal
range appropriate.
Anti-coagulant
therapy is not indicated as he doesn’t have atrial fibrillation to suggest this
as a cause of his transient ischaemic attacks.
Anti-coagulation therapy has no role in the
routine management of primary polycythaemia
The
risk/benefit balance of Aspirin in this situation outweighs that of Warfarin
because of the risks of bleeding associated with anti-coagulant therapy.
From <https://mle.ncl.ac.uk/cases/page/15729/>
24 December 2020
14:06
Thrombocytosis
Thrombocytosis is an abnormally
high platelet count, usually > 400 * 109/l.
Causes of thrombocytosis
·
reactive: platelets are an acute phase reactant - platelet count
can increase in response to stress such as a severe infection, surgery. Iron
deficiency anaemia can also cause a reactive thrombocytosis
·
malignancy
·
essential thrombocytosis (see below), or as part of another
myeloproliferative disorder such as chronic myeloid leukaemia or polycythaemia
rubra vera
·
hyposplenism
Essential thrombocytosis
Essential thrombocytosis is one of
the myeloproliferative disorders which overlaps with chronic myeloid leukaemia,
polycythaemia rubra vera and myelofibrosis. Megakaryocyte proliferation results
in an overproduction of platelets.
Features
·
platelet count > 600 * 109/l
·
both thrombosis (venous or arterial) and haemorrhage can be seen
·
a characteristic symptom is a burning sensation in the hands
·
a JAK2 mutation is found in around 50% of patients
Management
·
hydroxyurea (hydroxycarbamide) is widely used to reduce the
platelet count
·
interferon-α is also used in younger patients
·
low-dose aspirin may be used to reduce the thrombotic risk
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Aplastic anaemia
Characterised by pancytopenia and a
hypoplastic bone marrow
Peak incidence of acquired = 30
years old
Features
·
normochromic, normocytic anaemia
·
leukopenia, with lymphocytes relatively spared
·
thrombocytopenia
·
may be the presenting feature acute lymphoblastic or myeloid
leukaemia
·
a minority of patients later develop paroxysmal nocturnal
haemoglobinuria or myelodysplasia
Causes
·
idiopathic
·
congenital: Fanconi anaemia, dyskeratosis congenita
·
drugs: cytotoxics, chloramphenicol, sulphonamides, phenytoin, gold
·
toxins: benzene
·
infections: parvovirus, hepatitis
·
radiation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Autoimmune haemolytic anaemia
Autoimmune haemolytic anaemia
(AIHA) may be divided in to 'warm' and 'cold' types, according to at what
temperature the antibodies best cause haemolysis. It is most commonly
idiopathic but may be secondary to a lymphoproliferative disorder, infection or
drugs. AIHA is characterised by a positive direct antiglobulin test (Coombs'
test)
Warm AIHA
In warm AIHA the antibody (usually IgG) causes
haemolysis best at body temperature and haemolysis tends to occur in
extravascular sites, for example the spleen. Management options include
steroids, immunosuppression and splenectomy
Causes of warm AIHA
·
autoimmune disease: e.g. systemic
lupus erythematosus*
·
neoplasia: e.g. lymphoma, CLL
·
drugs: e.g. methyldopa
Cold AIHA
The antibody in cold AIHA is
usually IgM and causes
haemolysis best at 4 deg C. Haemolysis is mediated by complement and is more
commonly intravascular. Features may include symptoms of Raynaud's and
acrocynaosis. Patients respond less well to steroids
Causes of cold AIHA
·
neoplasia: e.g. lymphoma
·
infections: e.g. mycoplasma, EBV
*systemic lupus erythematosus can
rarely be associated with a mixed-type autoimmune haemolytic anaemia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Beta-thalassaemia major
Overview
·
absence of beta chains
·
chromosome 11
Features
·
presents in first year of life with failure to thrive and
hepatosplenomegaly
·
microcytic anaemia
·
HbA2 & HbF raised
·
HbA absent
Management
·
repeated transfusion → iron overload
·
s/c infusion of desferrioxamine
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Blood films: pathological cell forms
Pathological red cell forms
|
Abnormality |
Associated condition(s) |
Appearance |
||||
|
Target cells |
Sickle-cell/thalassaemia Iron-deficiency anaemia Hyposplenism Liver disease |
|
||||
|
'Tear-drop' poikilocytes |
Myelofibrosis |
|
||||
|
Spherocytes |
Hereditary spherocytosis Autoimmune hemolytic anaemia |
|
||||
|
Basophilic stippling |
Lead poisoning Thalassaemia Sideroblastic anaemia Myelodysplasia |
|
||||
|
Howell-Jolly bodies |
Hyposplenism |
|
||||
|
Heinz bodies |
G6PD deficiency Alpha-thalassaemia |
|
||||
|
Schistocytes ('helmet cells') |
Intravascular haemolysis Mechanical heart valve Disseminated intravascular coagulation |
|
||||
|
'Pencil' poikilocytes |
Iron deficency anaemia |
|
||||
|
Burr cells (echinocytes) |
Uraemia Pyruvate kinase deficiency |
|
||||
|
Acanthocytes |
Abetalipoproteinemia |
|
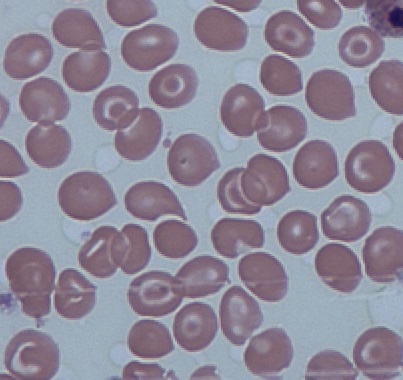
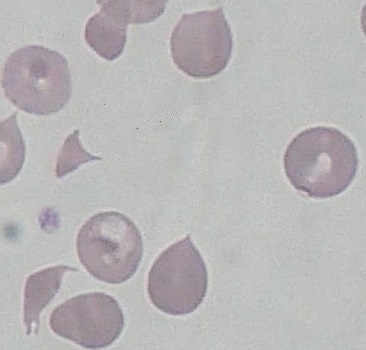
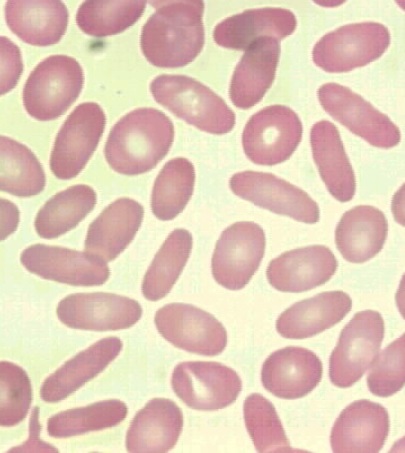
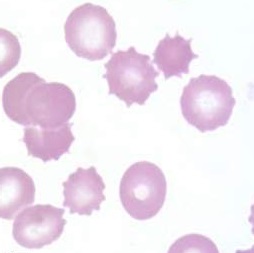
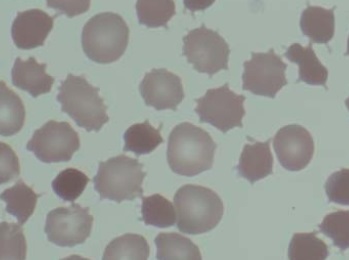
Other blood film abnormalities:
·
hypersegmented neutrophils: megaloblastic
anaemia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Graft versus host disease
Graft versus host disease (GVHD) is
a multi-system complication of allogeneic bone marrow transplantation. Less
frequently, it may also occur following solid organ transplantation or
transfusion in immunocompromised patients. The disease occurs when T cells in the donor tissue (the
graft) mount an immune response toward recipient (host) cells. It is not to be confused with transplant rejection (in which
recipient immune cells activate an immune response toward the donor tissue).
Prognosis is generally poor.
Three conditions required for
diagnosis of GVHD, known as the Billingham criteria 1:
·
The transplanted tissue contains immunologically functioning
cells
·
The recipient and donor are immunologically different
·
The recipient is immunocompromised
Estimates of incidence vary from
9-50% post allogeneic bone marrow transplant despite prophylaxis with
calcineurin inhibitors. The following principal risk factors have been
identified 2:
·
Poorly matched donor and recipient (particularly HLA)
·
Type of conditioning used prior to transplantation
·
Gender disparity between donor and recipient
·
Graft source (bone marrow or peripheral blood source associated
with higher risk than umbilical cord blood)
Acute and chronic GVHD are
considered separate syndromes:
Acute GVHD
·
Is classically defined as onset is classically within 100 days
of transplantation*
·
Usually affects the skin (>80%), liver (50%), and gastrointestinal
tract (50%)
·
Multi-organ involvement carries a worse prognosis**
Chronic GVHD
·
May occur following acute disease, or can arise de novo
·
Classically occurs after 100 days following transplantation
·
Has a more varied clinical picture: often lung and eye
involvement in addition to skin and GI, although any organ system may be
involved
Signs and symptoms - note that
diagnosis is largely clinical and based on the exclusion of other pathology:
Acute GVHD
·
Painful maculopapular rash (often neck, palms and soles),
which may progress to erythroderma or a toxic epidermal necrolysis-like
syndrome
·
Jaundice
·
Watery or bloody diarrhoea
·
Persistent nausea and vomiting
·
Can also present as a culture-negative fever
Chronic GVHD
·
Skin: Many manifestations including poikiloderma, scleroderma,
vitiligo, lichen planus
·
Eye: Often keratoconjunctivitis sicca, also corneal ulcers,
scleritis
·
GI: Dysphagia, odynophagia, oral ulceration, ileus. Oral
lichenous changes are a characteristic early sign (2)
·
Lung: my present as obstructive or restrictive pattern lung
disease
Investigations (largely dependent
on which organs are involved):
·
LFTs may demonstrate cholestatic jaundice. Hepatitis
screen/ultrasound may be useful to exclude other causes
·
Abdominal imaging may reveal air-fluid levels and small bowel
thickening ('ribbon sign')
·
Lung function testing
·
Biopsy of affected tissue may aid in diagnosis if there is
uncertainty
Management consists of
immunosuppression and supportive measures. Intravenous steroids are the
mainstay of immunosuppressive treatment in severe cases of acute GVHD. Extended
courses of steroid therapy are often needed in chronic GVHD and dose tapering
is vital. Second-line therapies include anti-TNF, mTOR inhibitors and extracorporeal
photopheresis. Excessive immunosuppression may predispose patients to
infection, and also limit the beneficial graft-versus-tumour effect of the
transplant.
Topical steroid therapy may be
sufficient in mild disease with limited cutaneous involvement.
*Please note that there is some
contention as to whether timeframe or clinical features should be used to
define acute vs chronic GVHD. Persistent, recurrent or late-onset acute GVHD
may occur, while chronic GVHD may manifest before the 100 day cutoff. As such,
diagnosis is often based on clinical manifestation as well as timeframe.
**A prognostic staging system for
acute GVHD exists based on serum bilirubin, abdominal imaging findings and
level of cutaneous involvement, but is beyond the scope of these notes.
References
1. Ferrara, J., Levine, J., Reddy,
P. & Holler, E. Graft-versus-host disease. The Lancet 373, 1550-1561
(2009).
2. Lazaryan, A. et al. Risk Factors
for Acute and Chronic Graft-versus-Host Disease after Allogeneic Hematopoietic
Cell Transplantation with Umbilical Cord Blood and Matched Sibling Donors.
Biology of Blood and Marrow Transplantation 22, 134-140 (2016).
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Granulocyte-colony stimulating factors
Recombinant human
granulocyte-colony stimulating factors are used to increase neutrophil counts
in patients who are neutropenic secondary to chemotherapy or other factors.
Examples include:
·
filgrastim
·
perfilgrastim
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Haematological malignancies: genetics
Below is a brief summary of the
common translocations associated with haematological malignancies
t(9;22) -
Philadelphia chromosome
·
present in > 95% of patients with CML
·
this results in part of the Abelson proto-oncogene being moved
to the BCR gene on chromosome 22
·
the resulting BCR-ABL gene codes for a fusion protein which has
tyrosine kinase activity in excess of normal
·
poor prognostic indicator in ALL
t(15;17)
·
seen in acute promyelocytic leukaemia (M3)
·
fusion of PML and RAR-alpha genes
t(8;14)
·
seen in Burkitt's lymphoma
·
MYC oncogene is translocated to an immunoglobulin gene
t(11;14)
·
Mantle cell lymphoma
·
deregulation of the cyclin D1 (BCL-1) gene
t(14;18)
·
follicular lymphoma
·
increased BCL-2 transcription
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Haematological malignancies: infections
Viruses
·
EBV: Hodgkin's and Burkitt's lymphoma, nasopharyngeal carcinoma
·
HTLV-1: Adult T-cell leukaemia/lymphoma
·
HIV-1: High-grade B-cell lymphoma
Bacteria
·
Helicobacter pylori: gastric lymphoma (MALT)
Protozoa
·
malaria: Burkitt's lymphoma
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Haemolytic anaemias: by cause
Hereditary haemolytic anaemias can be
subdivided into membrane, metabolism or haemoglobin defects
Hereditary causes
·
membrane: hereditary spherocytosis/elliptocytosis
·
metabolism: G6PD deficiency
·
haemoglobinopathies: sickle cell, thalassaemia
Acquired haemolytic anaemias can be
subdivided into immune and non-immune causes
Acquired: immune causes
·
autoimmune: warm/cold antibody type
·
alloimmune: transfusion reaction, haemolytic disease newborn
·
drug: methyldopa, penicillin
Acquired: non-immune causes
·
microangiopathic haemolytic anaemia (MAHA): TTP/HUS, DIC,
malignancy, pre-eclampsia
·
prosthetic cardiac valves
·
paroxysmal nocturnal haemoglobinuria
·
infections: malaria
·
drug: dapsone
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Hyposplenism
Causes
·
splenectomy
·
sickle-cell
·
coeliac disease, dermatitis herpetiformis
·
Graves' disease
·
systemic lupus erythematosus
·
amyloid
Features
·
Howell-Jolly bodies
·
siderocytes
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Iron deficiency anaemia vs. AOCD
|
|
Iron deficiency anaemia |
Anaemia of chronic disease |
|
Serum iron |
Low < 8 |
Low < 15 |
|
TIBC |
High |
Low |
|
Transferrin saturation |
Low |
Low |
|
Ferritin |
Low |
High |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Laboratory findings in haematological disease
The table below shows some very
selective laboratory findings that are commonly tested in the exam:
|
Test |
Interpretation |
|
Haptoglobin (Remember haptoglobin binds to
free haemoglobin) |
Decrease ·
intravascular haemolysis |
|
MCHC |
Increased ·
hereditary spherocytosis ·
autoimmune haemolytic anemia* Decreased ·
microcytic anaemia (e.g. iron deficiency) |
*associated with spherocytosis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Lead poisoning
Along with acute intermittent
porphyria, lead poisoning should be considered in questions giving a
combination of abdominal pain and neurological signs. Lead poisoning results in defective ferrochelatase and ALA
dehydratase function.
Features
·
abdominal pain
·
peripheral neuropathy (mainly motor)
·
fatigue
·
constipation
·
blue lines on gum margin (only 20% of adult patients,
very rare in children)
Investigations
·
the blood lead level is usually used for diagnosis. Levels
greater than 10 mcg/dl are considered significant
·
full blood count: microcytic anaemia. Blood film shows red cell
abnormalities including basophilic stippling and clover-leaf morphology
·
raised serum and urine levels of delta aminolaevulinic acid may
be seen making it sometimes difficult to differentiate from acute intermittent
porphyria
·
urinary coproporphyrin is also increased (urinary
porphobilinogen and uroporphyrin levels are normal to slightly increased)
·
in children, lead can accumulate in the
metaphysis of the bones although x-rays are not part of the standard work-up
Management - various chelating
agents are currently used:
·
dimercaptosuccinic acid (DMSA)
·
D-penicillamine
·
EDTA
·
dimercaprol
|
|
|
|
|
|
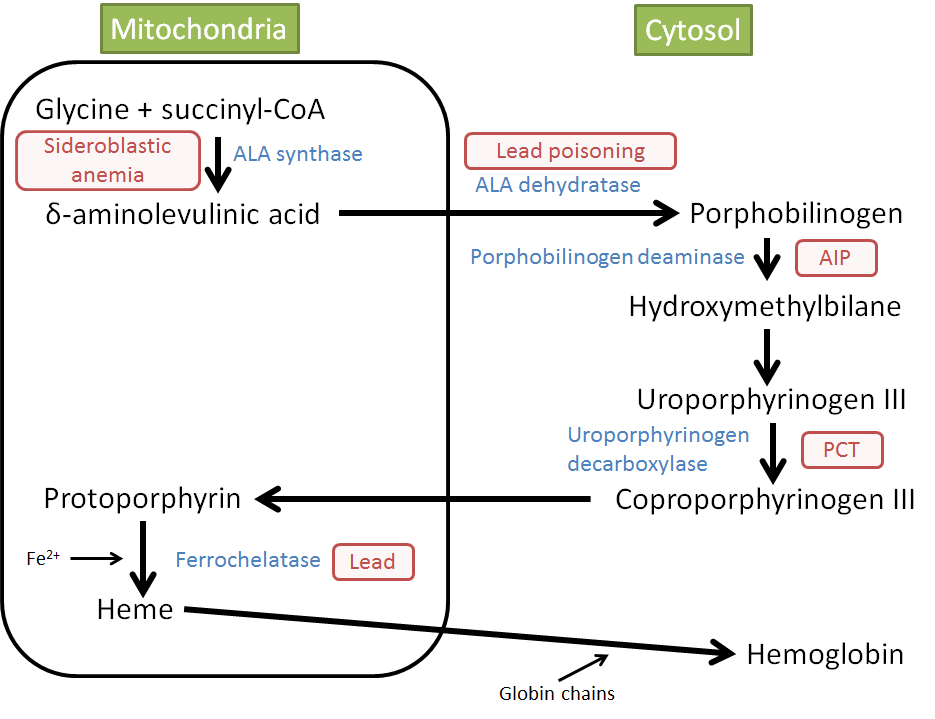
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Lymphadenopathy
There are many causes of
generalised lymphadenopathy
Infective
·
infectious mononucleosis
·
HIV, including seroconversion illness
·
eczema with secondary infection
·
rubella
·
toxoplasmosis
·
CMV
·
tuberculosis
·
roseola infantum
Neoplastic
·
leukaemia
·
lymphoma
Others
·
autoimmune conditions: SLE, rheumatoid arthritis
·
graft versus host disease
·
sarcoidosis
·
drugs: phenytoin and to a lesser extent allopurinol, isoniazid
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Microcytic anaemia
Causes
·
iron-deficiency anaemia
·
thalassaemia*
·
congenital sideroblastic anaemia
·
anaemia of chronic disease (more commonly a normocytic,
normochromic picture)
·
lead poisoning
A question sometimes seen in exams
gives a history of a normal haemoglobin level associated with a microcytosis.
In patients not at risk of thalassaemia, this should raise the possibility of
polycythaemia rubra vera which may cause an iron-deficiency secondary to
bleeding.
New onset microcytic anaemia in
elderly patients should be urgently
investigated to exclude underlying malignancy.
*in beta-thalassaemia minor the microcytosis is often disproportionate to the anaemia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Myelodysplastic syndrome
Overview
·
also known as myelodysplasia
·
acquired neoplastic disorder of hematopoietic stem cells
·
pre-leukaemia, may progress to AML
Features
·
more common with age
·
presents with bone marrow failure (anaemia, neutropaenia,
thrombocytopenia)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Myeloma
Myeloma classically causes
hypercalcaemia, pancytopenia and an AKI.
Multiple myeloma (MM) is a
haematological malignancy characterised by plasma cell proliferation. It arises
due to genetic mutations which occur as B-lymphocytes differentiate into mature
plasma cells. MM is the second most common haematological malignancy.
Presentation:
The median age at presentation is
70-years-old.
Use the mnemonicCRABBI:
·
Calcium
o Hypercalcaemia occurs as a result
of increased osteoclast activity within the bones
o This leads to constipation, nausea,
anorexia and confusion
·
Renal
o Monoclonal production of
immunoglobulins results in light chain deposition within the
renal tubules
o This causes renal damage which
presents as dehydration and increasing thirst
o Other causes of renal impairment in
myeloma include amyloidosis, nephrocalcinosis,
nephrolithiasis
·
Anaemia
o Bone marrow crowding suppresses
erythropoiesis leading to anaemia
o This causes fatigue and pallor
·
Bleeding
o bone marrow crowding also results
in thrombocytopenia which puts patients at increased risk of bleeding and
bruising
·
Bones
o Bone marrow infiltration by plasma
cells and cytokine-mediated osteoclast overactivity creates lytic bone lesions
o This may present as pain
(especially in the back) and increases the risk of fragility fractures
·
Infection
o a reduction in the production of
normal immunoglobulins results in increased susceptibility to infection
Investigations
·
Bloods will show anaemia (FBC) and thrombocytopenia (FBC);
raised urea and creatinine (U&E) and raised calcium
·
Peripheral blood film: rouleaux formation
·
Serum or urine protein electrophoresis: raised
concentrations of monoclonal IgA/IgG proteins will be present in the serum. In
the urine, they are known as Bence Jones proteins
·
Bone marrow aspiration and trephine biopsy: confirms the
diagnosis if the number of plasma cells is significantly raised
·
Whole-body MRI (or CT if MRI is not suitable) is used to survey
the skeleton for bone lesions
A common X-ray finding is a
'rain-drop' skull. This is numerous randomly placed dark spots seen on X-ray
which occur due to bone lysis.
Diagnosis
It is important to accurately
diagnose multiple myeloma, as unlike its pre-malignant counterparts (Monoclonal
gammopathy of undetermined significance and Smoldering myeloma), treatment must
begin immediately due to the risk of complications occurring as a result on
end-organ damage.
Symptomatic multiple myeloma is
defined at diagnosis by the presence of the following three factors:
·
Monoclonal plasma cells in the bone marrow >10%
·
Monoclonal protein within the serum or the urine (as determined
by electrophoresis)
·
Evidence of end-organ damage e.g. hypercalcaemia, elevated
creatinine, anaemia or lytic bone lesions/fractures
Management
Myeloma is a chronic relapsing and
remitting malignancy which is currently deemed incurable. Management aims to
control symptoms, reduce complications and prolong survival.
For those who have just been
diagnosed with symptomatic multiple myeloma, treatment begins with induction
therapy:
·
For patients who are suitable for autologous stem cell
transplantation* induction therapy consists of Bortezomib + Dexamethasone
·
For patients who are unsuitable for autologous stem cell
transplantation*, induction therapy consists of Thalidomide + an Alkylating
agent + Dexamethasone
Typically it is younger, healthier
patients who are suitable for stem cell transplantation and rigorous
chemotherapy regimes.
After completion of treatment,
patients are monitored every 3 months with blood tests and electrophoresis.
Many will achieve remission and will not need further therapy for some time.
Many patients do relapse after
initial therapy. If this occurs the 1st line recommended treatment is
Bortezomib monotherapy. Some patients may also be suitable for a repeat
autologous stem cell transplant*, but this is decided on a case-by-case basis.
Complications
A large part of multiple myeloma
treatment involves managing complications:
·
Pain: treat with analgesia (using the WHO analgesic ladder)
·
Pathological fracture: Zoledronic acid is given to prevent and
manage osteoporosis and fragility fractures as these are a large cause of
morbidity and mortality, particularly in the elderly.
·
Infection: patients receive annual influenza vaccinations. They
may also receive Immunoglobulin replacement therapy.
·
VTE prophylaxis
·
Fatigue: treat all possible underlying causes. If symptoms
persist consider an erythropoietin analogue.
*An autologous stem cell transplant
is used after high dose chemotherapy administration which targets stem cells.
It involves the removal of a patient's own stem cells prior to chemotherapy,
which are then replaced after chemotherapy. This is different from Allogenic
stem cell transplantation where stem cells are sourced from HLA matching
donors. Allogenic stem cell transplantation is currently only used as part of
clinical trials when treating multiple myeloma.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:06
Neutropaenia
Neutropaenia refers to a low
neutrophil counts, < 1.5 * 109. A normal neutophil count is 2.0 -
7.5 * 109.
It is important to recognise as it
predisposes to severe infection.
Neutropaenia may be further
subdivided as follows:
|
Severity |
Neutrophil count |
|
Mild |
1.0 - 1.5 * 109 |
|
Moderate |
0.5 - 1.0 * 109 |
|
Severe |
< 0.5 * 109 |
Causes
·
viral
o HIV
o Epstein-Barr virus
o hepatitis
·
drugs
o cytotoxics
o carbimazole
o clozapine
·
benign ethnic neutropaenia
o common in people of black African
and Afro-Caribbean ethnicity
o requires no treatment
·
haematological malignancy
o myelodysplastic malignancies
o aplastic anemia
·
rheumatological conditions
·
systemic lupus erythematosus: mechanisms include circulating
antineutrophil antibodies
·
rheumatoid arthritis: e.g. hypersplenism as in Felty's syndrome
·
severe sepsis
·
haemodialysis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Non-Hodgkin's lymphoma
Lymphoma is the malignant
proliferation of lymphocytes which accumulate in lymph nodes or other organs.
Lymphoma may be classified as either Hodgkin's lymphoma (a specific type of
lymphoma characterized by the presence of Reed-Sternberg cells) or
non-Hodgkin's lymphoma (every other type of lymphoma that is not Hodgkin's
lymphoma). Non-Hodgkin's lymphoma is the 6th most common cause of cancer in the
UK. Non-Hodgkin's lymphoma may affect either B or T-cells and can be further
classified as high grade or low grade.
Epidemiology
·
Non-Hodgkin's lymphoma is much more common than Hodgkin's
lymphoma
·
While different subtypes can affect different ages, it typically
affects the elderly with one-third of cases occurring in those over 75 years of
age
·
The incidence rate is 28 for men and 20 for females per 100,000
of the population
Risk factors
·
Elderly
·
Caucasians
·
History of viral infection (specifically Epstein-Barr virus)
·
Family history
·
Certain chemical agents (pesticides, solvents)
·
History of chemotherapy or radiotherapy
·
Immunodeficiency (transplant, HIV, diabetes mellitus)
·
Autoimmune disease (SLE, Sjogren's, coeliac disease)
Symptoms
·
Painless lymphadenopathy (non-tender, rubbery, asymmetrical)
·
Constitutional/B symptoms (fever, weight loss, night sweats,
lethargy)
·
Extranodal Disease - gastric (dyspepsia, dysphagia, weight loss,
abdominal pain), bone marrow (pancytopenia, bone pain), lungs, skin, central
nervous system (nerve palsies)
While differentiating Hodgkin's
lymphoma from non-Hodgkin's lymphoma is done by biopsy certain elements of the
clinical presentation can help point towards one rather than the other.
·
Lymphadenopathy in Hodgkin's lymphoma can experience
alcohol-induced pain in the node
·
'B' symptoms typically occur earlier in Hodgkin's lymphoma and
later in non-Hodgkin's lymphoma
·
Extra-nodal disease is much more common in non-Hodgkin's
lymphoma than in Hodgkin's lymphoma
Signs
·
Signs of weight loss
·
Lymphadenopathy (typically in the cervical, axillary or inguinal
region)
·
Palpable abdominal mass - hepatomegaly, splenomegaly, lymph
nodes
·
Testicular mass
·
Fever
Investigations
·
Excisional node biopsy is the diagnostic investigation of choice
(certain subtypes will have a classical appearance on biopsy such as Burkitt's
lymphoma having a 'starry sky' appearance)
·
CT chest, abdomen and pelvis (to assess staging)
·
HIV test (often performed as this is a risk factor for
non-Hodgkin's lymphoma)
·
FBC and blood film (patient may have a normocytic anaemia and
can help rule out other haematological malignancy such as leukaemia)
·
ESR (useful as a prognostic indicator)
·
LDH (a marker of cell turnover, useful as a prognostic
indicator)
·
Other investigations can be ordered as the clinical picture
indicates (LFT's if liver metastasis suspected, PET CT or bone marrow biopsy to
look for bone involvement, LP if neurological symptoms)
Staging
- The most common staging system
used for non-Hodgkin's lymphoma is the Ann Arbor system.
·
→ Stage 1 - One node affected
·
→ Stage 2 - More than one node affected on the same side of the
diaphragm
·
→ Stage 3 - One node affected on either side of the diaphragm
·
→ Stage 4 - Extra-nodal involvement e.g. Spleen, bone marrow or
CNS
·
The stage is combined with the letter A or B to indicate the
presence of 'B' symptoms. With the letter A indicating no B symptoms present
and B indicating any of the beta symptoms present. For example, a patient with
a single node affected and no 'B' symptoms would be stage 1A.
Management
·
Management is dependent on the specific sub-type of
non-Hodgkin's lymphoma and will typically take the form of watchful waiting,
chemotherapy or radiotherapy.
·
All patients will receive flu/pneumococcal vaccines
·
Patients with neutropenia may require antibiotic prophylaxis
Complications
·
Bone marrow infiltration causing anaemia, neutropenia or
thrombocytopenia
·
Superior vena cava obstruction
·
Metastasis
·
Spinal cord compression
·
Complications related to treatment e.g. Side effects of chemotherapy
Prognosis
·
Low-grade non-Hodgkin's lymphoma has a better prognosis
·
High-grade non-Hodgkin's lymphoma has a worse prognosis but a
higher cure rate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Normocytic anaemia
Causes of normocytic anaemia
include
·
anaemia of chronic disease
·
chronic kidney disease
·
aplastic anaemia
·
haemolytic anaemia
·
acute blood loss
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Pregnancy: DVT/PE
Overview
·
pregnancy is a hypercoagulable state
·
majority occur in last trimester
Pathophysiology
·
increase in factors VII, VIII, X and fibrinogen
·
decrease in protein S
·
uterus presses on IVC causing venous stasis in legs
Management
·
warfarin contraindicated
·
S/C low-molecular weight heparin preferred to IV heparin (less
bleeding and thrombocytopenia)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Primary immunodeficiency
Primary immunodeficiency disorders
may be classified according to which component of the immune system they
affect.
Neutrophil disorders
|
Disorder |
Underlying defect |
Notes |
|
Chronic granulomatous disease |
Lack of NADPH oxidase reduces ability
of phagocytes to produce reactive oxygen species |
Causes recurrent pneumonias
and abscesses, particularly due to catalase-positive bacteria (e.g. Staphylococcus aureus and fungi (e.g. Aspergillus) Negative nitroblue-tetrazolium test Abnormal dihydrorhodamine flow
cytometry test |
|
Chediak-Higashi syndrome |
Microtubule polymerization defect which
leads to a decrease in phagocytosis |
Affected children have 'partial
albinism' and peripheral neuropathy. Recurrent bacterial infections are seen Giant granules in neutrophils and
platelets |
|
Leukocyte adhesion deficiency |
Defect of LFA-1 integrin (CD18) protein
on neutrophils |
Recurrent bacterial infections. Delay in umbilical cord sloughing may
be seen Absence of neutrophils/pus at sites of
infection |
B-cell disorders
|
Disorder |
Underlying defect |
Notes |
|
Common variable immunodeficiency |
Many varying causes |
Hypogammaglobulinemia is seen. May
predispose to autoimmune disorders and lymphona |
|
Bruton's (x-linked) congenital
agammaglobulinaemia |
Defect in Bruton's tyrosine kinase
(BTK) gene that leads to a severe block in B cell development |
X-linked recessive. Recurrent bacterial
infections are seen Absence of B-cells with reduced
immunoglogulins of all classes |
|
Selective immunoglobulin A deficiency |
Maturation defect in B cells |
Most common primary antibody
deficiency. Recurrent sinus and respiratory infections Associated with coeliac disease and may
cause false negative
coeliac antibody screen Severe reactions to blood transfusions
may occur (anti-IgA antibodies → analphylaxis) |
T-cell disorders
|
Disorder |
Underlying defect |
Notes |
|
DiGeorge syndrome |
22q11.2 deletion, failure to develop
3rd and 4th pharyngeal pouches |
Common features include congenital
heart disease (e.g. tetralogy of Fallot), learning difficulties, hypocalcaemia,
recurrent viral/fungal diseases, cleft palate |
Combined B- and T-cell disorders
|
Disorder |
Underlying defect |
Notes |
|
Severe combined immunodeficiency |
Many varying causes. Most common
(X-linked) due to defect in the common gamma chain, a protein used in the
receptors for IL-2 and other interleukins.
Other causes include adenosine deaminase deficiency |
Recurrent infections due to viruses,
bacteria and fungi. Reduced T-cell receptor excision
circles Stem cell transplantation may be
successful |
|
Ataxic telangiectasia |
Defect in DNA repair enzymes |
Autosomal recessive. Features include cerebellar
ataxia, telangiectasia
(spider angiomas), recurrent chest infections and 10%
risk of developing malignancy, lymphoma or leukaemia |
|
Wiskott-Aldrich syndrome |
Defect in WASP gene |
X-linked recessive. Features include
recurrent bacterial infections, eczema, thrombocytopaenia. Low IgM levels Increased risk of autoimmune disorders
and malignancy |
|
Hyper IgM Syndromes |
Mutations in the CD40 gene |
Infection/Pneumocystis pneumonia, hepatitis, diarrhoea |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Sickle-cell anaemia: management
Crisis management
·
analgesia e.g. opiates
·
rehydrate
·
oxygen
·
consider antibiotics if evidence of infection
·
blood transfusion
·
exchange transfusion: e.g. if neurological complications
Longer-term management
·
Hydroxyurea (Hydroxycarbamide)
o increases the HbF levels and is
used in the prophylactic management of sickle cell anaemia to prevent painful
episodes
·
NICE CKS suggest that sickle cell patients should receive the pneumococcal polysaccharide vaccine every 5 years
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Sickle-cell crises: management
General management
·
analgesia e.g. opiates
·
rehydrate
·
oxygen
·
consider antibiotics if evidence of infection
·
blood transfusion
·
exchange transfusion: e.g. if neurological complications
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Thrombocytopenia
Causes of severe thrombocytopenia
·
ITP
·
DIC
·
TTP
·
haematological malignancy
Causes of moderate thrombocytopenia
·
heparin induced thrombocytopenia (HIT)
·
drug-induced (e.g. quinine, diuretics, sulphonamides, aspirin,
thiazides)
·
alcohol
·
liver disease
·
hypersplenism
·
viral infection (EBV, HIV, hepatitis)
·
pregnancy
·
SLE/antiphospholipid syndrome
·
vitamin B12 deficiency
Pseudothrombocytopenia has been
reported in association with the use of EDTA as an anticoagulant
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Thrombotic thrombocytopenic purpura
Pathogenesis of thrombotic
thrombocytopenic purpura (TTP)
·
abnormally large and sticky multimers of von Willebrand's factor
cause platelets to clump within vessels
·
in TTP there is a deficiency of ADAMTS13 (a metalloprotease enzyme) which breakdowns ('cleaves') large multimers of von Willebrand's factor
·
overlaps with haemolytic uraemic syndrome (HUS)
Features
·
rare, typically adult females
·
fever
·
fluctuating neuro signs (microemboli)
·
microangiopathic haemolytic anaemia
·
thrombocytopenia
·
renal failure
Causes
·
post-infection e.g. urinary, gastrointestinal
·
pregnancy
·
drugs: ciclosporin, oral contraceptive pill, penicillin,
clopidogrel, aciclovir
·
tumours
·
SLE
·
HIV
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Thymoma
Thymomas are the most common tumour
of the anterior mediastinum and is usually detected between the sixth and
seventh decades of life.
Associated with
·
myasthenia gravis (30-40% of patients with thymoma)
·
red cell aplasia
·
dermatomyositis
·
also : SLE, SIADH
Causes of death
·
compression of airway
·
cardiac tamponade
|
|
|
|
©
Image used on license from Radiopaedia |
|
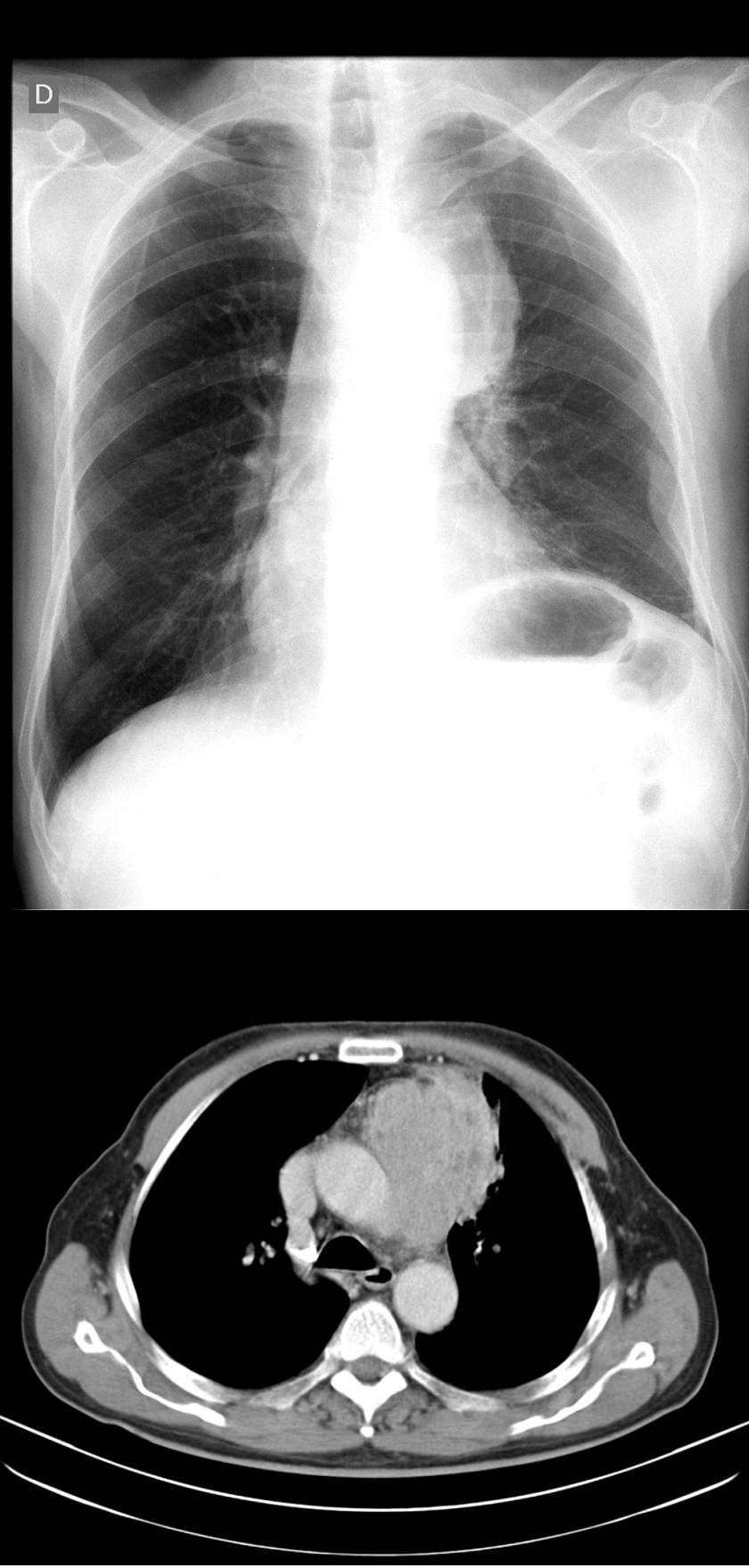
Chest x-ray and accompanying CT scan of a patient with a
thymoma. In the chest x-ray there is a partially delineated mediastinal mass
(anterior mediastinum) with regular borders, bulging the left upper mediastinal
contour.
|
|
|
|
©
Image used on license from Radiopaedia |
|
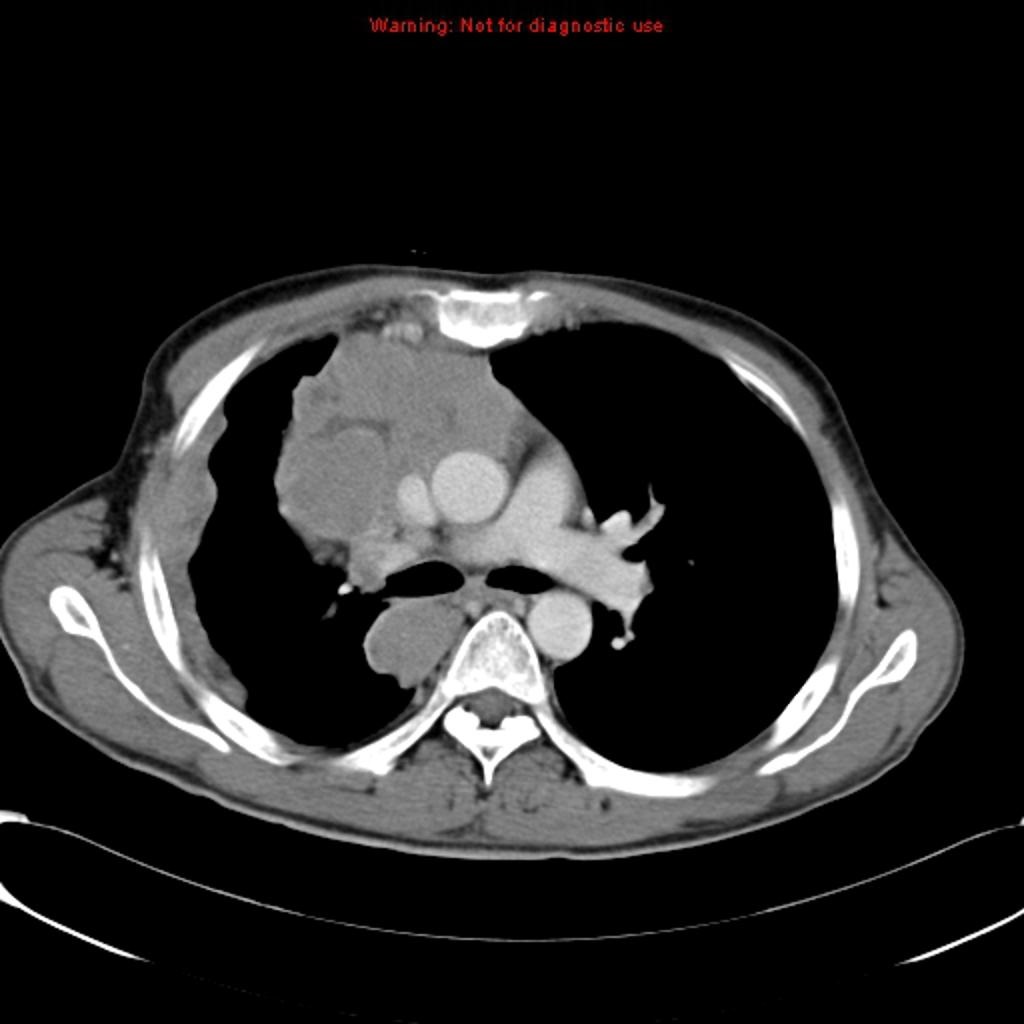
CT slice at the bifurcation of the main bronchus showing
an invasive thymoma presenting as an anterior mediastinal mass
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:07
Tranexamic acid
Tranexamic acid is a synthetic
derivative of lysine. Its primary mode of action is as an antifibrinolytic that reversibly
binds to lysine receptor sites on plasminogen or plasmin. This prevents plasmin
from binding to and degrading fibrin.
Tranexamic acid is most commonly
prescribed to help treat menorrhagia.
The role of tranexamic acid in
trauma was investigated in the CRASH 2 trial and has been shown to be of
benefit in bleeding trauma when administered in the first 3 hours. Tranexamic acid is given as an IV
bolus followed by an infusion in cases of major haemorrhage.
There is also ongoing research
looking at the role of tranexamic acid in traumatic brain injury.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:08
Waldenstrom's macroglobulinaemia
Waldenstrom's macroglobulinaemia is
an uncommon condition seen in older men. It is a lymphoplasmacytoid malignancy
characterised by the secretion of a monoclonal IgM paraprotein
Features
·
monoclonal IgM paraproteinaemia
·
systemic upset: weight loss, lethargy
·
hyperviscosity syndrome e.g. visual disturbance
o the pentameric configuration of IgM
increases serum viscosity
·
hepatosplenomegaly
·
lymphadenopathy
·
cryoglobulinaemia e.g. Raynaud's
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:49
Blood product transfusion complications
Blood product transfusion
complications may be broadly classified into the following:
·
immunological: acute haemolytic, non-haemolytic febrile,
allergic/anaphylaxis
·
infective
·
transfusion-related acute lung injury (TRALI)
·
transfusion-associated circulatory overload (TACO)
·
other: hyperkalaemia, iron overload, clotting
The table below summaries some of
the key features:
|
Reaction |
Features |
Management |
|
Non-haemolytic febrile reaction Thought to be caused by antibodies
reacting with white cell fragments in the blood product and cytokines that
have leaked from the blood cell during storage |
Fever, chills Red cell transfusion (1-2%) Platelet transfusion (10-30%) |
Slow or stop the transfusion Paracetamol Monitor |
|
Minor allergic reaction Thought to be caused by foreign plasma
proteins |
Pruritus, urticaria |
Temporarily stop the transfusion Antihistamine Monitor |
|
Anaphylaxis Can be caused by patients
with IgA deficiency who have anti-IgA antibodies |
Hypotension, dyspnoea, wheezing,
angioedema. |
Stop the transfusion IM adrenaline ABC support ·
oxygen ·
fluids |
|
Acute haemolytic reaction ABO-incompatible blood e.g. secondary
to human error |
Fever, abdominal pain, hypotension |
Stop transfusion Confirm diagnosis ·
check the identity of patient/name on blood product ·
send blood for direct Coombs test, repeat typing
and cross-matching Supportive care ·
fluid resuscitation |
|
Transfusion-associated circulatory
overload (TACO) Excessive rate of transfusion,
pre-existing heart failure |
Pulmonary oedema, hypertension |
Slow or stop transfusion Consider intravenous loop
diuretic (e.g. furosemide) and oxygen |
|
Transfusion-related acute lung injury
(TRALI) Non-cardiogenic pulmonary oedema
thought to be secondary to increased vascular permeability caused by host
neutrophils that become activated by substances in donated blood |
Hypoxia, pulmonary infiltrates on chest
x-ray, fever, hypotension |
Stop the transfusion Oxygen and supportive care |
Further information is provided
below:
Acute haemolytic transfusion
reaction
Acute haemolytic transfusion
reaction results from a mismatch of blood group (ABO) which causes massive
intravascular haemolysis. This is usually the result of red blood cell
destruction by IgM-type antibodies.
Symptoms begin minutes after the
transfusion is started and include a fever, abdominal and chest pain, agitation
and hypotension.
Treatment should include immediate
transfusion termination, generous
fluid resuscitation with saline solution and informing
the lab
Complications include disseminated
intravascular coagulation, and renal failure
Non-haemolytic febrile reaction
Febrile reactions
·
due to white blood cell HLA antibodies
·
often the result of sensitization by previous pregnancies or
transfusions
·
paracetamol may be given
Allergic/anaphylaxis reaction
Allergic reactions to blood
transfusions are caused by hypersensitivity reactions to components within the
transfusion. Symptoms typically arise within minutes of starting the
transfusion and severity can range from urticaria to anaphylaxis with
hypotension, dyspnoea, wheezing, and stridor, or angioedema.
Simple urticaria should be treated
by discontinuing the transfusion and with an antihistamine. Once the symptoms resolve, the transfusion may be continued
with no need for further workup.
More severe allergic reaction or
anaphylaxis should be treated urgently. The transfusion should be permanently
discontinued, intramuscular
adrenaline should be administered and
supportive care. Antihistamine, corticosteroids and bronchodilators should also
be considered for these patients.
Transfusion-related acute lung
injury (TRALI)
A rare but potentially fatal
complication of blood transfusion. Characterised by the development of
hypoxaemia / acute respiratory distress syndrome within 6 hours of transfusion.
Features include:
·
hypoxia
·
pulmonary infiltrates on chest x-ray
·
fever
·
hypotension
Transfusion-associated circulatory
overload (TACO)
A relatively common reaction due to
fluid overload resulting in pulmonary oedema. As well as features of pulmonary
oedema the patient may also by hypertensive,
a key difference from patients with TRALI.
Infective
Transmission of vCJD
·
although the absolute risk is very small, vCJD may be
transmitted via blood transfusion
·
a number of steps have been taken to minimise this risk, including:
o from late 1999 onward, all
donations have undergone removal of white cells (leucodepletion) in order to
reduce any vCJD infectivity present
o from 1999, plasma derivatives have
been fractionated from imported plasma rather than being sourced from UK
donors. Fresh Frozen Plasma (FFP) used for children and certain groups of
adults needing frequent transfusions is also imported
o from 2004 onward, recipients of
blood components have been excluded from donating blood
From <https://www.passmedicine.com/review/textbook.php?s=#>
Mnemonic
for transfusion reactions:
Got a bad unit
G raft
vs. Host disease
O verload
T hrombocytopaenia
A lloimmunization
B lood
pressure unstable
A cute
haemolytic reaction
D elayed
haemolytic reaction
U rticaria
N eutrophilia
I nfection
T ransfusion
associated lung injury
From <https://www.passmedicine.com/question/questions.php?q=0#>
21 December 2020
21:50
Deep vein thrombosis: diagnosis and management
NICE updated their guidelines on
the investigation and management of venous thromboembolism (VTE) in 2020. Some
of the key changes include recommending the following:
·
the use of direct oral anticoagulants (DOACs) as first-line
treatment for most people with VTE, including as interim anticoagulants before
a definite diagnosis is made
·
the use of DOACs in patients with
active cancer, as opposed to
low-molecular weight heparin as was the previous recommendation
·
routine cancer screening is no longer recommended following a
VTE diagnosis
If a patient is suspected of having
a DVT a two-level DVT Wells score should be performed:
Two-level DVT Wells score
|
Clinical
feature |
Points |
|
Active cancer (treatment ongoing,
within 6 months, or palliative) |
1 |
|
Paralysis, paresis or recent plaster
immobilisation of the lower extremities |
1 |
|
Recently bedridden for 3 days or more
or major surgery within 12 weeks requiring general or regional anaesthesia |
1 |
|
Localised tenderness along the
distribution of the deep venous system |
1 |
|
Entire leg swollen |
1 |
|
Calf swelling at least 3 cm larger than
asymptomatic side |
1 |
|
Pitting oedema confined to the
symptomatic leg |
1 |
|
Collateral superficial veins
(non-varicose) |
1 |
|
Previously documented DVT |
1 |
|
An alternative diagnosis is at least as
likely as DVT |
-2 |
Clinical probability simplified
score
·
DVT likely: 2 points or more
·
DVT unlikely: 1 point or less
If a DVT is 'likely' (2 points or more)
·
a proximal leg vein ultrasound scan should be carried out within
4 hours
o if the result is positive then a
diagnosis of DVT is made and anticoagulant treatment should start
o if the result is negative a D-dimer
test should be arranged. A negative scan and negative D-dimer makes the
diagnosis unlikely and alternative diagnoses should be considered
·
if a proximal leg vein ultrasound scan cannot be carried out
within 4 hours a D-dimer test should be performed and interim
therapeutic anticoagulation administered whilst waiting for the proximal leg vein ultrasound
scan (which should be performed within 24 hours)
o interim therapeutic anticoagulation
used to mean giving low-molecular weight heparin
o NICE updated their guidance in
2020. They now recommend using an anticoagulant that can be continued if the
result is positive.
o this means normally a direct oral
anticoagulant (DOAC) such as apixaban or rivaroxaban
·
if the scan is negative but the D-dimer
is positive:
o stop interim therapeutic
anticoagulation
o offer a repeat proximal leg vein
ultrasound scan 6 to 8 days later
If a DVT is 'unlikely' (1 point or
less)
·
perform a D-dimer test
o this should be done within 4 hours.
If not, interim therapeutic anticoagulation should be given until the result is
available
o if the result is negative then DVT
is unlikely and alternative diagnoses should be considered
o if the result is positive then a
proximal leg vein ultrasound scan should be carried out within 4 hours
o if a proximal leg vein ultrasound
scan cannot be carried out within 4 hours interim therapeutic
anticoagulation should be administered whilst waiting for the proximal leg vein
ultrasound scan (which should be performed within 24 hours)
D-dimer tests
·
NICE recommend either a point-of-care (finger prick) or
laboratory-based test
·
age-adjusted cut-offs should be used for patients > 50 years
old
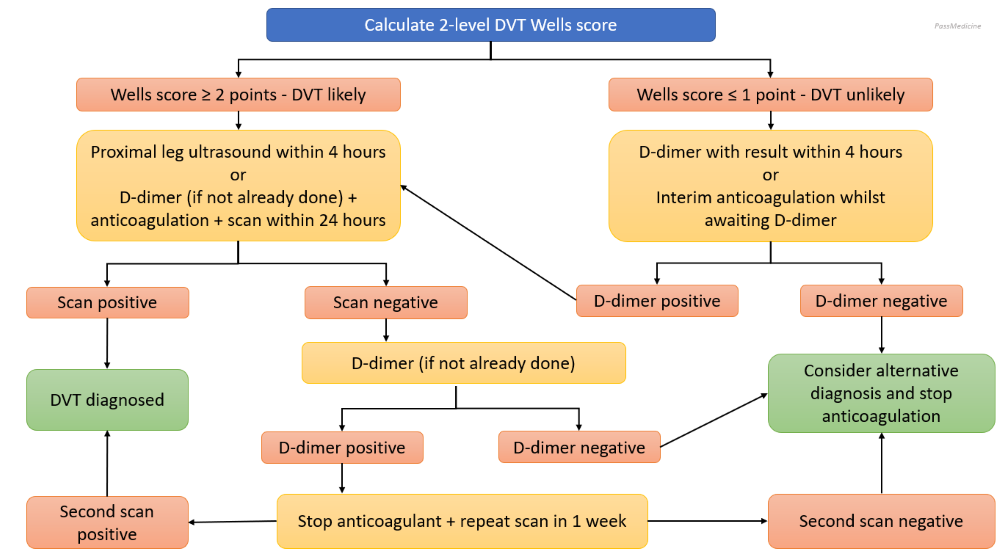
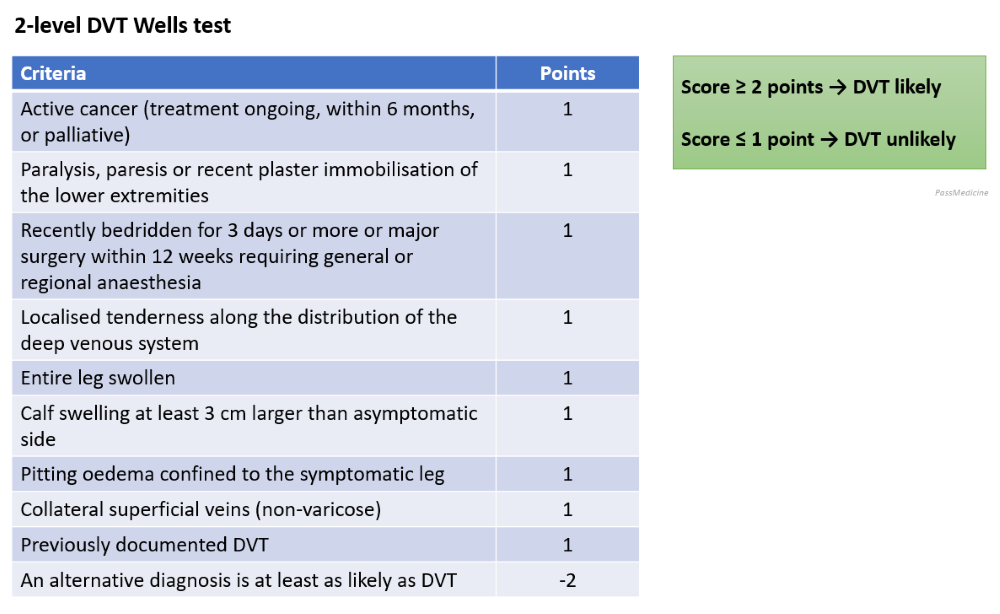
Management
The cornerstone of VTE management
is anticoagulant therapy. This was historically done with warfarin, often
preceded by heparin until the INR was stable. However, the development of
DOACs, and an evidence base supporting their efficacy, has changed modern
management.
Choice of anticoagulant
·
the big change in the 2020 guidelines was the increased use of
DOACs
·
apixaban or rivaroxaban (both DOACs) should be offered
first-line following the diagnosis of a DVT
o instead of using low-molecular
weight heparin (LMWH) until the diagnosis is confirmed, NICE now advocate using
a DOAC once a diagnosis is suspected, with this continued if the diagnosis is confirmed
o if neither apixaban or rivaroxaban
are suitable then either LMWH followed by dabigatran or edoxaban OR LMWH
followed by a vitamin K antagonist (VKA, i.e. warfarin)
·
if the patient has active cancer
o previously LMWH was recommended
o the new
guidelines now recommend using a DOAC, unless this is contraindicated
·
if renal impairment is severe (e.g. < 15/min) then LMWH,
unfractionated heparin or LMWH followed by a VKA
·
if the patient has antiphospholipid syndrome (specifically
'triple positive' in the guidance) then LMWH followed by a VKA should be used
Length of anticoagulation
·
all patients should have anticoagulation for at least 3 months
·
continuing anticoagulation after this period is partly
determined by whether the VTE was provoked or unprovoked
o a provoked VTE is due to an obvious
precipitating event e.g. immobilisation following major surgery. The
implication is that this event was transient and the patient is no longer at
increased risk
o an unprovoked VTE occurs in the
absence of an obvious precipitating event, i.e. there is a possibility that
there are unknown factors (e.g. mild thrombophilia) making the patient more at
risk from further clots
·
if the VTE was provoked the treatment is
typically stopped after the initial 3 months (3 to 6 months for people with
active cancer)
·
if the VTE was unprovoked then treatment is
typically continued for up to 3 further months (i.e. 6 months in total)
o NICE recommend that whether a
patient has a total of 3-6 months anticoagulant is based upon balancing a
person's risk of VTE recurrence and their risk of bleeding
o the HAS-BLED score can be used to
help assess the risk of bleeding
o NICE state: 'Explain to people with unprovoked DVT or PE and a low bleeding risk that
the benefits of continuing anticoagulation treatment are likely to outweigh the
risks. '. The implication of this is that in the absence of a bleeding
risk factors, patients are generally better off continuing anticoagulation for
a total of 6 months
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:40
Chronic lymphocytic leukaemia: complications
Complications
·
anaemia
·
hypogammaglobulinaemia leading
to recurrent infections
·
warm autoimmune haemolytic anaemia in
10-15% of patients
·
transformation to high-grade
lymphoma (Richter's transformation)
Richter's
transformation
Ritcher's
transformation occurs when leukaemia cells enter the lymph node and change into
a high-grade, fast-growing non-Hodgkin's lymphoma. Patients often become unwell very suddenly.
Ritcher's
transformation is indicated by one of the following symptoms:
·
lymph node swelling
·
fever without infection
·
weight loss
·
night sweats
·
nausea
·
abdominal pain
Next
question
Save my notes
Search
Go
Google
search on "Chronic lymphocytic leukaemia: complications"
Links
|
statMed.org |
00 |
|
|
Suggest linkReport broken link
Media
|
|
|
|
|
|
|
Medicosis
Perfectionalis - YouTube |
20 |
|
|
|
|
|
|
|
Medicosis
Perfectionalis - YouTube |
62 |


Suggest mediaReport broken media
Score: 30%
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
20:42
Hodgkin's lymphoma: histological classification and prognosis
Hodgkin's lymphoma is a malignant
proliferation of lymphocytes characterised by the presence of the
Reed-Sternberg cell. It has a bimodal age distributions being most common in
the third and seventh decades
Histological classification
|
Type |
Frequency |
Prognosis |
Notes |
|
Nodular sclerosing |
Most common (around 70%) |
Good prognosis |
More common in women. Associated with
lacunar cells |
|
Mixed cellularity |
Around 20% |
Good prognosis |
Associated with a large number of
Reed-Sternberg cells |
|
Lymphocyte predominant |
A*round 5% |
Best prognosis |
|
|
Lymphocyte depleted |
Rare |
Worst prognosis |
|
'B' symptoms also imply a poor
prognosis
·
weight loss > 10% in last 6 months
·
fever > 38ºC
·
night sweats
Other factors associated with a
poor prognosis identified in a 1998 NEJM paper included:
·
age > 45 years
·
stage IV disease
·
haemoglobin < 10.5 g/dl
·
lymphocyte count < 600/µl or < 8%
·
male
·
albumin < 40 g/l
·
white blood count > 15,000/µl
*Reed-Sternberg cells with nuclei
surrounded by a clear space
From <https://www.passmedicine.com/question/questions.php?q=0#>
21 December 2020
21:49
Blood films: typical pictures
Hyposplenism e.g. post-splenectomy, coeliac disease (occurs in around 30% of coeliac patients)
·
target cells
·
Howell-Jolly bodies
·
Pappenheimer bodies
·
siderotic granules
·
acanthocytes
Iron-deficiency anaemia
·
target cells
·
'pencil' poikilocytes
·
if combined with B12/folate deficiency a 'dimorphic' film occurs
with mixed microcytic and macrocytic cells
Myelofibrosis
·
'tear-drop' poikilocytes
Intravascular haemolysis
·
schistocytes
Megaloblastic anaemia
·
hypersegmented neutrophils
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:49
Blood products: FFP, cryoprecipitate and prothrombin
complex
NICE published guidelines on the
use of blood products in 2015.
Fresh frozen plasma (FFP)
·
most suited for 'clinically significant' but without 'major
haemorrhage' in patients with a prothrombin time (PT) ratio or activated
partial thromboplastin time (APTT) ratio > 1.5
·
typically 150-220 mL
·
can be used prophylactically in patients undergoing invasive
surgery where there is a risk of significant bleeding
·
In contrast to red cells, the universal donor of FFP is AB blood
because it lacks any anti-A or anti-B antibodies
Cryoprecipitate
·
contains concentrated Factor VIII:C, von Willebrand factor,
fibrinogen, Factor XIII and fibronectin, produced by further processing of
Fresh Frozen Plasma (FFP). Clinically it is most commonly used to replace
fibrinogen
·
much smaller volume than FFP, typically 15-20mL
·
most suited for patients for 'clinically significant' but
without 'major haemorrhage' who have a fibrinogen concentration < 1.5 g/L
·
example use cases include disseminated intravascular
coagulation, liver failure and hypofibrinogenaemia secondary to massive
transfusion. It may also be used in an emergency situation for haemophiliacs
(when specific factors not available) and in von Willebrand disease
·
can be used prophylactically in patients undergoing invasive
surgery where there is a risk of significant bleeding where the fibrinogen
concentration < 1.0 g/L
Prothrombin complex concentrate
·
used for the emergency reversal of anticoagulation in patients
with either severe bleeding or a head injury with suspected intracerebral
haemorrhage
·
can be used prophylactically in patients undergoing emergency
surgery depending on the particular circumstance
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
20:14
Hodgkin's lymphoma: staging
Hodgkin's lymphoma is a malignant
proliferation of lymphocytes characterised by the presence of the
Reed-Sternberg cell. It has a bimodal age distributions being most common in
the third and seventh decades
Ann-Arbor staging of Hodgkin's
lymphoma
·
I: single lymph node
·
II: 2 or more lymph nodes/regions on same side of diaphragm
·
III: nodes on both sides of diaphragm
·
IV: spread beyond lymph nodes
Each stage may be subdivided into A
or B
·
A = no systemic symptoms other than pruritus
·
B = weight loss > 10% in last 6 months, fever > 38c, night
sweats (poor prognosis)
From <https://www.passmedicine.com/question/questions.php?q=0#>
Lymphocyte-depleted
Hodgkin lymphoma is the rarest form of Hodgkin's lymphoma as well as the most aggressive . It is typically
seen in young adults aged 30-37 years of age. Risk factors include a family
history and being immunocompromised. Treatment of Lymphocyte-depleted Hodgkin
lymphoma is typically adjusted for prognostic factors and the cancer stage
(Stage IV being associated with the worst prognosis).
Negative
prognostic factors include:
·
The presence of B symptoms (night sweats,
weight loss and fever)
·
Male gender
·
Being aged >45 years old at diagnosis
·
High WCC, low Hb, high ESR or low blood albumin
From <https://www.passmedicine.com/question/questions.php?q=0#>
Acute promyelocytic
leukemia
29 December 2020
15:14
The
most common symptoms and their causes are:
·
Anaemia –
breathlessness, fatigue
·
Low white cells –
frequent, persistent infections
·
Low platelets –
bruising and/or bleeding
·
DIC –
bruising/bleeding which may be very severe
t(15;17)
·
seen in acute
promyelocytic leukaemia (M3)
·
fusion
of PML and RAR-alpha
genes
From <https://www.passmedicine.com/question/questions.php?q=0>
APL
is diagnosed by tests which may include:
·
Blood tests
·
Bone marrow samples
Other
tests may be done
Occasionally,
it is not clear from the blood film whether the abnormal cells are
promyelocytes. By examining the proteins found on the outside of the cell,
called cell markers, it is possible to identify the cells with certainty.
Another
test looks for an abnormality called PML-RARA. This is an abnormal “fusion
gene” – PML and RARA are two genes which are normally found on different
chromosomes. In APL the two chromosomes swap over part of their DNA, which
joins the PML and RARA genes together. This test is important because the main
drugs used to treat APL work directly on the PML-RARA gene; in the very rare
cases of APL without PML-RARA, other treatments can be used.
These tests may be repeated from time to time during your treatment.
This is to find out how the APL is responding to treatm
Treatment
of patients who are suspected of having APL should be treated immediately, even
before the diagnosis is made, because they can quickly develop potentially
life-threatening bleeding or blood clotting symptoms. A firm diagnosis of APL
using genetic testing can be performed later, and treatment can be discontinued
if APL is not confirmed.
Patients
with APL are generally subdivided into the following two groups according to
their white blood count as treatment recommendations can differ for each group:
·
Low- to
intermediate-risk: patients with a white blood cell count of 10,000
cells per microlitre of blood or less.
·
High-risk: patients with a
white blood cell count of more than 10,000 cells per microlitre of blood.
Treatment
of patients who are suspected of having APL should be treated immediately, even
before the diagnosis is made, because they can quickly develop potentially
life-threatening bleeding or blood clotting symptoms. A firm diagnosis of APL
using genetic testing can be performed later, and treatment can be discontinued
if APL is not confirmed.
Patients
with APL are generally subdivided into the following two groups according to
their white blood count as treatment recommendations can differ for each group:
·
Low- to
intermediate-risk: patients with a white blood cell count of 10,000
cells per microlitre of blood or less.
·
High-risk: patients with a
white blood cell count of more than 10,000 cells per microlitre of blood.
First-line
treatment
First-line treatment for APL includes all-trans retinoic acid
(ATRA), which is an active by- product of vitamin A. ATRA blocks the effect of
the PML-RARA gene that prevents the promyelocyte cells maturing into normal
white blood cells (differentiation).
ATRA
is not a chemotherapeutic drug and is called a differentiating agent. It is
given in combination with another drug in patients with APL to prevent any drug
resistance.
ATRA
can sometimes be given with chemotherapy drugs called anthracyclines.
Anthracyclines, such as daunorubicin and idarubicin, interfere with the DNA and
reproduction of white blood cells, including the leukaemia cells. ATRA is given
as a capsule, while anthracyclines are given intravenously.
In 2018, NICE approved a drug called arsenic trioxide (ATO) for
the first-line treatment of APL in previously untreated patients, with low- to
intermediate-risk disease and patients whose APL has returned (relapsed) or did
not respond to chemotherapy (refractory). ATO is also a differentiating agent
and acts in a similar way to ATRA.
Because
differentiating agents have less side effects to chemotherapy drugs, especially
anthracyclines, the combination of ATRA and ATO alone is a preferred first-line
therapy, particularly as studies found it to be at least as effective as the
combination of ATRA and anthracyclines, if not more so, with a reduced risk of
disease relapse.
Induction
treatment
To
achieve remission (induction therapy), the 2019 guidelines from the European
Leukaemia Network (European LeukemiaNet) recommend the following regimens:
·
Low-to-intermediate
risk patients: ATRA and ATO
·
High-risk patients:
Both of the following regimens achieve similar results; however, ATO is not
approved for high-risk patients by NICE as yet.
o ATRA and ATO plus a cytoreductive chemotherapy
such as cytarabine. Cytoreductive means that the chemotherapy reduces the
number of cells.
o ATRA plus anthracyclines. The most frequently
used regimen being called AIDA.
The
treatment for APL that has developed as a consequence of prior chemotherapy is
normally similar to APL associated with the PML-RARA gene, although your doctor
may choose to use a different drug in this situation.
In
addition to induction treatment, patients with APL require supportive care in
the form of blood product transfusions to maintain the platelet count and the
blood clotting indicators as normal as possible and to prevent the risk of
bleeding. Blood chemical levels (particularly potassium and magnesium which are
important for electrical conduction in the heart) will be monitored closely.
Sometimes it is necessary to also give potassium and/or magnesium supplements.
Consolidation
treatment
To
consolidate remission in patients who have not received chemotherapy-based
treatment, four courses of ATO and seven courses of ATRA are recommended. This
can usually be given as an outpatient.
For
patients who received ATRA and chemotherapy regimens, two to three courses of
anthracycline- based chemotherapy should be given for consolidation therapy.
This is usually given as an inpatient.
Maintenance
treatment
For
low- to intermediate-risk patients, maintenance treatment after consolidation
with ATO and ATRA is not recommended, but for high-risk patients on ATRA and
chemotherapy who are showing clinical benefit, maintenance may be initiated
with tablets for two years.
Second-line
treatment
First-line
treatment is generally successful in most patients with APL. However, for
patients who haven’t gone into first remission or who have relapsed,
second-line treatment options are available.
Relapse
or being refractory to first-line treatment can occur in any patient with APL,
regardless of whether they have been treated with ATRA with ATO or ATRA with
chemotherapy. However, these events are uncommon in low- to intermediate-risk
patients.
The
second-line treatment you have for relapsed or refractory APL will depend
mainly on which first- line treatment you were given. If you have had ATRA with
ATO as first-line treatment, then you will receive ATRA with chemotherapy, and
vice-versa (you will be given ATRA with ATO if you had ATRA with chemotherapy
as first-line treatment).
In
young, fit patients, an autologous stem cell transplant can be performed. With
an autologous stem cell transplant, you are given intensive chemotherapy to
destroy all the leukaemia cells. However, as the chemotherapy will also kill
your own bone marrow cells, you are given a transplant of your own healthy stem
cells which were collected before the intensive chemotherapy. However, in
patients who were responding well to ATO and then relapsed, a transplant is not
always necessary.
24 December 2020
13:54
Primary hyperaldosteronism
Primary hyperaldosteronism was
previously thought to be most commonly caused by an adrenal adenoma, termed
Conn's syndrome. However, recent studies have shown that bilateral idiopathic adrenal
hyperplasia is the cause in up to 70% of cases.
Differentiating between the two is important as this determines treatment.
Adrenal carcinoma is an extremely rare cause of primary hyperaldosteronism.
Features
·
hypertension
·
hypokalaemia
o e.g. muscle weakness
o this is a classical feature in
exams but studies suggest this is seen in only 10-40% of patients
·
alkalosis
Investigations
·
the 2016 Endocrine Society recommend that a plasma aldosterone/renin ratio is the first-line
investigation in suspected primary hyperaldosteronism
o should show high aldosterone levels
alongside low renin levels (negative feedback due to sodium retention from
aldosterone)
·
following this a high-resolution CT abdomen and adrenal vein
sampling is used to differentiate between unilateral and bilateral sources of aldosterone
excess
·
Adrenal Venous Sampling (AVS) can be done to identify the gland
secreting excess hormone in primary hyperaldosteronism
Management
·
adrenal adenoma: surgery
·
bilateral adrenocortical hyperplasia: aldosterone
antagonist e.g. spironolactone
|
|
|
|
©
Image used on license from Radiopaedia |
|

CT abdomen showing a right-sided adrenal adenoma in a
patient who presented with hypertension and hypokalaemia. The adenoma can be
seen 'next to' or 'below' the liver.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:54
SGLT-2 inhibitors
SGLT-2 inhibitors reversibly inhibit
sodium-glucose co-transporter 2 (SGLT-2) in the renal proximal convoluted
tubule to reduce
glucose reabsorption and increase urinary glucose excretion.
Examples include canagliflozin,
dapagliflozin and empagliflozin.
Important adverse effects include
·
urinary and genital infection (secondary to glycosuria). Fournier’s gangrene has also been reported
·
normoglycaemic ketoacidosis
·
increased risk of lower-limb amputation: feet should be closely
monitored
Patients taking SGLT-2 drugs often lose weight, which can be beneficial in type 2 diabetes mellitus.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:54
Graves' disease: features
Graves' disease is the most common
cause of thyrotoxicosis. It is typically seen in women aged 30-50 years.
Features
·
typical features of thyrotoxicosis
·
specific signs limited to Grave's (see below)
Features seen in Graves' but not in
other causes of thyrotoxicosis
·
eye signs (30% of patients)
o exophthalmos
o ophthalmoplegia
·
pretibial myxoedema
·
thyroid acropachy, a triad of:
o digital clubbing
o soft tissue swelling of the hands
and feet
o periosteal new bone formation
Autoantibodies
·
TSH receptor stimulating antibodies (90%)
·
anti-thyroid peroxidase antibodies (75%)
From <https://www.passmedicine.com/review/textbook.php?s=#>
Corneal involvement in Grave's disease indicates severe eye
pathology
Important for meLess important
The
severity of Grave's eye disease can be graded using the mnemonic NOSPECS
·
No signs / symptoms
·
Only signs (e.g: upper
lid retraction)
·
Signs & symptoms
(including soft-tissue involvement)
·
Proptosis
·
Extra-ocular muscle
involvement
·
Corneal involvement
·
Sight loss due to
optic nerve involvement
Therefore
the correct answer is corneal involvement.
From <https://www.passmedicine.com/question/questions.php?q=0#>
24 December 2020
13:55
Primary hyperparathyroidism
In exams, primary
hyperparathyroidism is stereotypically seen in elderly females with an
unquenchable thirst and an inappropriately normal or raised parathyroid hormone
level. It is most commonly due to a solitary adenoma
Causes of primary
hyperparathyroidism
·
80%: solitary adenoma
·
15%: hyperplasia
·
4%: multiple adenoma
·
1%: carcinoma
Features - 'bones, stones,
abdominal groans and psychic moans'
·
polydipsia, polyuria
·
peptic ulceration/constipation/pancreatitis
·
bone pain/fracture
·
renal stones
·
depression
·
hypertension
Associations
·
hypertension
·
multiple endocrine neoplasia: MEN I and II
Investigations
·
raised calcium, low phosphate
·
PTH may be raised or (inappropriately, given
the raised calcium) normal
·
technetium-MIBI subtraction scan
·
pepperpot skull is a characteristic X-ray finding of hyperparathyroidism
Treatment
·
the definitive management is total
parathyroidectomy
·
conservative management may be offered if the calcium level is
less than 0.25 mmol/L above the upper limit of normal AND the patient is >
50 years AND there is no evidence of end-organ damage
·
calcimimetic agents such as cinacalcet are sometimes used in
patients who are unsuitable for surgery
|
|
|
|
©
Image used on license from Radiopaedia |
|

Bilateral hand radiographs in a middle-aged woman
demonstrating generalised osteopenia, erosion of the terminal phalangeal tufts
(acro-osteolysis) and subperiosteal resorption of bone particularly the radial
aspects of the 2nd and 3rd middle phalanges. These changes are consistent with
a diagnosis of hyperparathyroidism.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:55
|
|
|||
|
|
Addison's
disease Autoimmune destruction of the adrenal glands is the commonest cause of primary hypoadrenalism in the UK,
accounting for 80% of cases. This is termed Addison's disease and results in reduced cortisol and aldosterone being produced. Features ·
lethargy, weakness,
anorexia, nausea & vomiting, weight loss, 'salt-craving' ·
hyperpigmentation
(especially palmar creases)*, vitiligo, loss of pubic hair in women, hypotension, hypoglycaemia ·
hyponatraemia and
hyperkalaemia may be seen ·
crisis: collapse,
shock, pyrexia Other causes of hypoadrenalism Primary causes ·
tuberculosis ·
metastases (e.g. bronchial carcinoma) ·
meningococcal septicaemia
(Waterhouse-Friderichsen syndrome) ·
HIV ·
antiphospholipid
syndrome Secondary causes ·
pituitary disorders
(e.g. tumours, irradiation, infiltration) Exogenous glucocorticoid therapy *Primary Addison's is associated with
hyperpigmentation whereas secondary adrenal insufficiency is not From <https://www.passmedicine.com/review/textbook.php?s=#>
hyperpigmentation could be caused by the stimulant
effect of excess ACTH on the melanocytes to produce melanin Investigation ACTH
stimulation test (Short synacthen (tetracosactide) test) How
it is done: Baseline
cortisol and ACTH levels are performed. Synthetic ACTH 0.25mg is given IM or
IV. 30 and 60 minutes after the injection, blood samples are drawn for
cortisol levels. Cortisol
usually increase >600 after 30 minutes Management: Glucocorticoid
replacement with hydrocortisone and fludrocortisone to replace
mineralocorticoid Patient
may present with adrenal crisis if undiagnosed with appreciable mortality. An
acute adrenal crisis can manifest with vomiting, abdominal pain, and
hypovolaemic shock |
||
|
|
|
||
|
|
24 December 2020
13:55
Cushing's syndrome: investigations
Investigations are divided into
confirming Cushing's syndrome and then localising the lesion. A hypokalaemic metabolic
alkalosis may be seen, along with impaired
glucose tolerance. Ectopic ACTH secretion (e.g. secondary to small cell lung
cancer) is characteristically associated with very low potassium levels. An
insulin stress test is used to differentiate between true Cushing's and
pseudo-Cushing's
Tests to confirm Cushing's syndrome
The two most commonly used tests
are:
·
overnight dexamethasone suppression test (most sensitive)
·
24 hr urinary free cortisol
Localisation tests
The first-line localisation is 9am
and midnight plasma ACTH (and cortisol) levels. If ACTH is suppressed then a
non-ACTH dependent cause is likely such as an adrenal adenoma
Both low- and high-dose
dexamethasone suppression tests may be used to localise the pathology resulting
in Cushing's syndrome. These tests may be interpreted as follows:
|
Cortisol
following low-dose dexamethasone |
Cortisol following high-dose dexamethasone |
ACTH |
Interpretation |
|
↓ |
↓ |
↔ |
Normal |
|
↔ |
↔ |
↓ |
Cushing's syndrome due to other causes
(e.g. adrenal adenomas) |
|
↔ |
↓ |
↑ |
Cushing's disease (i.e. pituitary adenoma → ACTH secretion) |
|
↔ |
↔ |
↑ |
Ectopic ACTH syndrome likely |
CRH stimulation
·
if pituitary source then cortisol rises
·
if ectopic/adrenal then no change in cortisol
Petrosal sinus sampling of ACTH may
be needed to differentiate between pituitary and ectopic ACTH secretion
From <https://www.passmedicine.com/review/textbook.php?s=#>
Suppression
after high dose dexamethasone indicates pituitary source
High ACTH excludes adrenal source
Needs
pituitary imaging, preferably MRI Corticotrophin releasing hormone test can be
used to confirm pituitary source in difficult cases if imaging inconclusive.
Should see an exaggerated ACTH and cortisol response at 30 mins post injection.
Inferior petrosal sinus sampling will help confirm pituitary source
If
pituitary adenoma identified then transsphenoidal surgery ± radiotherapy first
choice
24 December 2020
13:55
Diabetes mellitus: sick day rules
The following are key messages that
should be given to all patients with diabetes if they become unwell:
·
Increase frequency of blood glucose monitoring to four hourly or
more frequently
·
Encourage fluid intake aiming for at least 3 litres in 24hrs
·
If unable to take struggling to eat may need sugary drinks to
maintain carbohydrate intake
·
It is useful to educate patients so that they have a box of
'sick day supplies' that they can access if they become unwell
·
Access to a mobile phone has been shown to reduce progression of
ketosis to diabetic ketoacidosis
If a patient is taking oral
hypoglycaemic medication, they should be advised to continue taking their
medication even if they are not eating much. Remember that the stress response
to illness increases cortisol levels pushing blood sugars high even without
much oral intake. The possible exception is with metformin, which should be
stopped if a patient is becoming dehydrated because of the potential impact
upon renal function.
If a patient is on insulin, they
must not stop it due to the risk of diabetic ketoacidosis. They should continue
their normal insulin regime but ensure that they are checking their blood
sugars frequently. Patients should be able to check their ketone levels and if
these are raised and blood sugars are also raised they may need to give
corrective doses of insulin. The corrective dose to be given varies by patient,
but a rule of thumb would be total daily insulin dose divided by 6 (maximum 15
units). NHS Scotland have produced a useful flowsheet for patients to follow:
http://www.diabetesinscotland.org.uk/ketocard/ketosheet.pdf
Possible indications that a patient
might require admission to hospital would include:
·
Suspicion of underlying illness requiring hospital treatment eg
myocardial infarction
·
Inability to keep fluids down - admit if persisting more than a
few hours
·
Persistent diarrhoea
·
Significant ketosis in an insulin dependent diabetic despite
additional insulin
·
Blood glucose persistently >20mmol/l despite additional
insulin
·
Patient unable to manage adjustments to usual diabetes
management
·
Lack of support at home e.g. a patient who lives alone and is at
risk of becoming unconscious
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:55
Hypercalcaemia: causes
Two conditions account for 90% of
cases of hypercalcaemia:
·
1. Primary hyperparathyroidism: commonest cause in
non-hospitalised patients
·
2. Malignancy: the commonest cause in hospitalised patients. This
may be due to number of processes, including; bone
metastases, myeloma, PTHrP from squamous cell lung cancer
Other causes include
·
sarcoidosis*
·
vitamin D intoxication
·
acromegaly
·
thyrotoxicosis
·
Milk-alkali syndrome
·
drugs: thiazides, calcium containing antacids
·
dehydration
·
Addison's disease
·
Paget's disease of the bone**
*other causes of granulomas may
lead to hypercalcaemia e.g. Tuberculosis and histoplasmosis
**usually normal in this condition
but hypercalcaemia may occur with prolonged immobilisation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Thyroid function tests
The interpretation of thyroid
function tests is usually straightforward:
|
Diagnosis |
TSH |
Free T4 |
Notes |
|
Thyrotoxicosis (e.g. Graves' disease) |
Low |
High |
In T3 thyrotoxicosis the free T4 will
be normal |
|
Primary hypothyroidism (primary
atrophic hypothyroidism) |
High |
Low |
|
|
Secondary hypothyroidism |
Low |
Low |
Replacement steroid therapy is required
prior to thyroxine |
|
Sick euthyroid syndrome* |
Low** |
Low |
Common in hospital inpatients T3 is particularly low in these
patients |
|
Subclinical hypothyroidism |
High |
Normal |
|
|
Poor compliance with thyroxine |
High |
Normal |
|
|
Steroid therapy |
Low |
Normal |
|
|
|
|
|
|
|
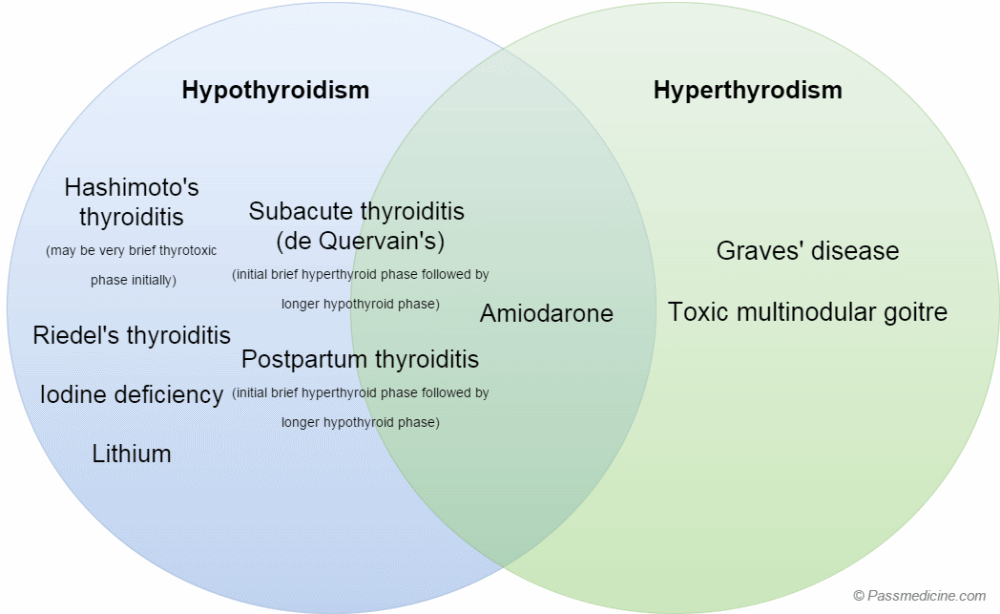
Venn diagram showing how different causes of thyroid
dysfunction may manifest. Note how many causes of hypothyroidism may have an
initial thyrotoxic phase.
*now referred to as non-thyroidal
illness
**TSH may be normal in some cases
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Diabetes mellitus: a very basic introduction
Diabetes mellitus is one of the
most common conditions encountered in clinical practice and represents a
significant burden on the health systems of the developed world. It is now
estimated that 8% of the total NHS budget is now spent on managing patients
with diabetes mellitus.
What is diabetes mellitus?
Diabetes mellitus may be defined as
a chronic condition characterised by abnormally raised levels of blood glucose.
Why is the management of diabetes
mellitus so important?
Before the advent of insulin
therapy untreated type 1 diabetes would usually result in death. Poorly treated
type 1 diabetes mellitus can still result in significant morbidity and
mortality (as a result of diabetic ketoacidosis). However, the main focus of
diabetes management now is reducing the incidence of macrovascular (ischaemic
heart disease, stroke) and microvascular (eye, nerve and kidney damage)
complications.
|
Type |
Notes |
|
Type 1 diabetes mellitus (T1DM) |
Autoimmune disorder where the
insulin-producing beta cells of the islets of Langerhans in the pancreas are
destroyed by the immune system This results in an absolute deficiency
of insulin resulting in raised glucose levels Patients tend to develop T1DM in
childhood/early adult life and typically present unwell, possibly in diabetic
ketoacidosis |
|
Type 2 diabetes mellitus (T2DM) |
This is the most common cause of
diabetes in the developed world. It is caused by a relative deficiency
of insulin due to an excess of adipose tissue.
In simple terms there isn't enough insulin to 'go around' all the excess fatty
tissue, leading to blood glucose creeping up. |
|
Prediabetes |
This term is used for patients
who don't yet meet the criteria for a formal diagnosis of T2DM to be made but
are likely to develop the condition over the next few years. They, therefore, require closer monitoring and
lifestyle interventions such as weight loss |
|
Gestational diabetes |
Some pregnant develop raised
glucose levels during pregnancy. This
is important to detect as untreated it may lead to adverse outcomes for the
mother and baby |
|
Maturity onset diabetes of the young
(MODY) |
A group of inherited genetic disorders
affecting the production of insulin. Results in younger patients developing
symptoms similar to those with T2DM, i.e. asymptomatic hyperglycaemia with
progression to more severe complications such as diabetic ketoacidosis |
|
Latent autoimmune diabetes of adults
(LADA) |
The majority of patients with
autoimmune-related diabetes present younger in life. There are however a
small group of patients who develop such problems later in life. These patients are often misdiagnosed as having
T2DM |
|
Other types |
Any pathological process which damages
the insulin-producing cells of the pancreas may cause diabetes to develop.
Examples include chronic pancreatitis and haemochromatosis. Drugs may also cause raised glucose
levels. A common example is glucocorticoids which commonly result in raised
blood glucose levels |
Symptoms and signs
The presentation of diabetes
mellitus depends very much on the type:
|
Type
1 DM |
Type 2 DM |
|
Weight loss Polydipsia Polyuria May present with diabetic ketoacidosis ·
abdominal pain ·
vomiting ·
reduced consciousness level |
Often picked up incidentally on routine
blood tests Polydipsia Polyuria |
Remember that the polyuria and
polydipsia are due to water being 'dragged' out of the body due to the osmotic
effects of excess blood glucose being excreted in the urine (glycosuria).
Investigations
There are 4 main ways to check
blood glucose:
·
a finger-prick bedside glucose monitor
·
a one-off blood glucose. This may either be fasting or
non-fasting
·
a HbA1c. This measures the amount of glycosylated haemoglobin
and represents the average blood glucose over the past 2-3 months
·
a glucose tolerance test. In this test, a fasting blood glucose
is taken after which a 75g glucose load is taken. After 2 hours a second blood
glucose reading is then taken
The diagnostic criteria are
determined by WHO.
If the patient is symptomatic:
·
fasting glucose greater than or equal to 7.0 mmol/l
·
random glucose greater than or equal to 11.1 mmol/l (or after
75g oral glucose tolerance test)
If the patient is asymptomatic the
above criteria apply but must be demonstrated on two separate occasions.
In 2011 WHO released supplementary
guidance on the use of HbA1c for the diagnosis of diabetes:
·
a HbA1c of greater than or equal to 6.5% (48 mmol/mol) is
diagnostic of diabetes mellitus
·
a HbAlc value of less than 6.5% does not exclude diabetes (i.e.
it is not as sensitive as fasting samples for detecting diabetes)
·
in patients without symptoms, the test must be repeated to
confirm the diagnosis
·
it should be remembered that misleading HbA1c results can be
caused by increased red cell turnover
|
|
|
|
|
|
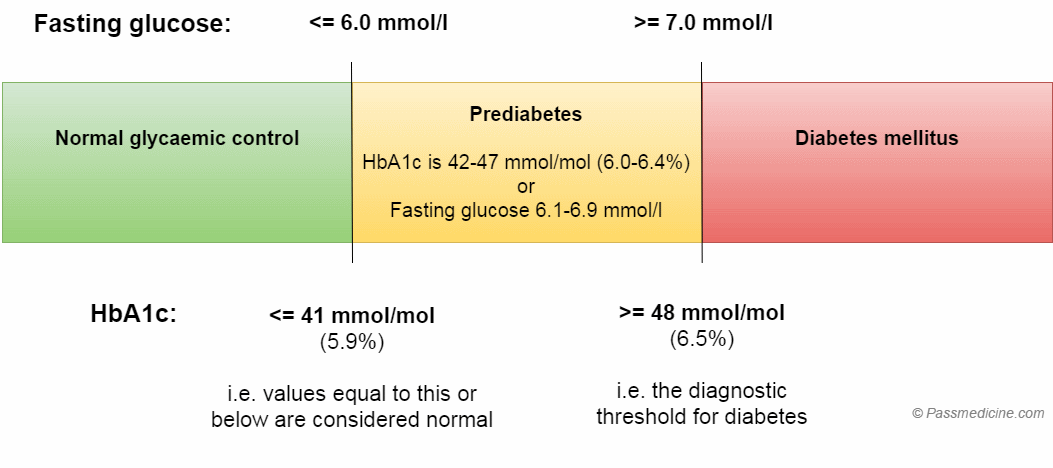
Diagram showing the spectrum of diabetes diagnosis
Management
The principle of managing diabetes
mellitus are as follows:
·
drug therapy to normalise blood glucose levels
·
monitoring for and treating any complications related to
diabetes
·
modifying any other risk factors for other conditions such as
cardiovascular disease
Type 1 diabetes
·
patients always require insulin to control the blood sugar
levels. This is because there is an absolute deficiency of insulin with no
pancreatic tissue left to stimulate with drugs
·
different types of insulin are available according to their
duration of action
Type 2 diabetes
·
the majority of patients with type 2 diabetes are controlled
using oral medication
·
the first-line drug for the vast majority of patients is
metformin
·
second-line drugs include sulfonylureas, gliptins and
pioglitazone. Please see the table below for further information
·
if oral medication is not controlling the blood glucose to a
sufficient degree then insulin is used
The table below shows some of the
main drugs used in the management of diabetes mellitus:
|
Drug
class |
Mechanism of action |
Route |
Main side-effects |
Notes |
|
Insulin |
Direct replacement for endogenous
insulin |
Subcutaneous |
Hypoglycaemia Weight gain Lipodystrophy |
Used in all patients with T1DM and some
patients with poorly controlled T2DM Can be classified according to source
(analogue, human sequence and porcine) and duration of action (short,
immediate, long-acting) |
|
Metformin |
Increases insulin sensitivity Decreases hepatic gluconeogenesis |
Oral |
Gastrointestinal upset Lactic acidosis* |
First-line medication in the management
of T2DM Cannot be used in patients with an eGFR
of < 30 ml/min |
|
Sulfonylureas |
Stimulate pancreatic beta cells to
secrete insulin |
Oral |
Hypoglycaemia Weight gain Hyponatraemia |
Examples include gliclazide and
glimepiride |
|
Thiazolidinediones |
Activate PPAR-gamma receptor in
adipocytes to promote adipogenesis and fatty acid uptake |
Oral |
Weight gain Fluid retention |
Only currently available
thiazolidinedione is pioglitazone |
|
DPP-4 inhibitors (-gliptins) |
Increases incretin levels which inhibit
glucagon secretion |
Oral |
Generally well tolerated but increased
risk of pancreatitis |
|
|
SGLT-2 inhibitors (-gliflozins) |
Inhibits reabsorption of glucose in the
kidney |
Oral |
Urinary tract infection |
Typically result in weight loss |
|
GLP-1 agonists (-tides) |
Incretin mimetic which inhibits
glucagon secretion |
Subcutaneous |
Nausea and vomiting Pancreatitis |
Typically result in weight loss |
NICE provide guidelines on how drug
therapy should be used in T2DM:
|
|
|
|
|
|
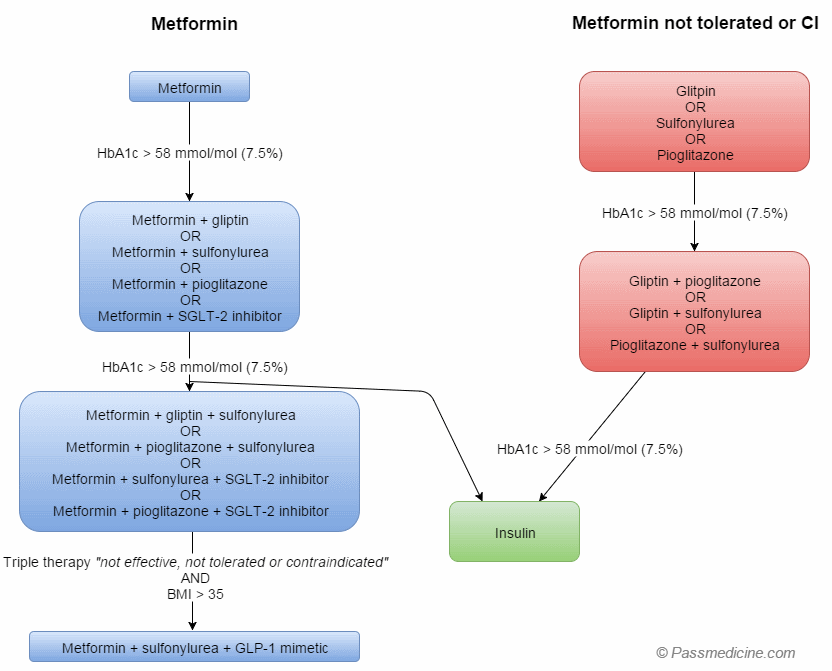
*common in exams, much less common
in clinical practice
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Diabetic neuropathy
Diabetes typically leads to sensory loss and not motor loss in peripheral neuropathy. Painful diabetic
neuropathy is a common problem in clinical practice.
NICE updated it's guidance on the
management of neuropathic pain in 2013. Diabetic neuropathy is now managed in
the same way as other forms of neuropathic pain:
·
first-line treatment: amitriptyline, duloxetine,
gabapentin or pregabalin
·
if the first-line drug treatment does not work try one of the
other 3 drugs
·
tramadol may be used as 'rescue therapy' for exacerbations of
neuropathic pain
·
topical capsaicin may be used for localised neuropathic pain
(e.g. post-herpetic neuralgia)
·
pain management clinics may be useful in
patients with resistant problems
Gastrointestinal autonomic
neuropathy
Gastroparesis
·
symptoms include erratic blood glucose control, bloating and vomiting
·
management options include metoclopramide, domperidone or erythromycin (prokinetic agents)
Chronic diarrhoea
·
often occurs at night
Gastro-oesophageal reflux disease
·
caused by decreased lower esophageal sphincter (LES) pressure
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Parathyroid glands and disorders of calcium metabolism
Hyperparathyroidism
|
Disease
type |
Hormone profile |
Clinical features |
Cause |
|
Primary hyperparathyroidism |
·
PTH (Elevated) ·
Ca2+ (Elevated) ·
Phosphate (Low) ·
Urine calcium : creatinine clearance ratio >
0.01 |
·
May be asymptomatic if mild ·
Recurrent abdominal pain (pancreatitis, renal
colic) ·
Changes to emotional or cognitive state |
Most cases due to solitary adenoma
(80%), multifocal disease occurs in 10-15% and parathyroid carcinoma in 1% or
less |
|
Secondary hyperparathyroidism |
·
PTH (Elevated) ·
Ca2+ (Low or normal) ·
Phosphate (Elevated) ·
Vitamin D levels (Low) |
·
May have few symptoms ·
Eventually may develop bone disease, osteitis
fibrosa cystica and soft tissue calcifications |
Parathyroid gland hyperplasia occurs as
a result of low calcium, almost always in a setting of chronic renal failure |
|
Tertiary hyperparathyroidism |
·
Ca2+ (Normal or high) ·
PTH (Elevated) ·
Phosphate levels (Decreased or Normal) ·
Vitamin D (Normal or decreased) ·
Alkaline phosphatase (Elevated) |
·
Metastatic calcification ·
Bone pain and / or fracture ·
Nephrolithiasis ·
Pancreatitis |
Occurs as a result of ongoing
hyperplasia of the parathyroid glands after correction of underlying renal
disorder, hyperplasia of all 4 glands is usually the cause |
Differential diagnoses
It is important to consider the
rare but relatively benign condition of benign familial hypocalciuric
hypercalcaemia, caused by an autosomal dominant genetic disorder. Diagnosis is
usually made by genetic testing and concordant biochemistry (urine calcium :
creatinine clearance ratio <0.01-distinguished from primary
hyperparathyroidism).
Treatment
Primary hyperparathyroidism
Indications for surgery
·
Elevated serum Calcium > 1mg/dL above normal
·
Hypercalciuria > 400mg/day
·
Creatinine clearance < 30% compared with normal
·
Episode of life threatening hypercalcaemia
·
Nephrolithiasis
·
Age < 50 years
·
Neuromuscular symptoms
·
Reduction in bone mineral density of the femoral neck, lumbar
spine, or distal radius of more than 2.5 standard deviations below peak bone
mass (T score lower than -2.5)
Secondary hyperparathyroidism
Usually managed with medical therapy.
Indications for surgery in
secondary (renal) hyperparathyroidism:
·
Bone pain
·
Persistent pruritus
·
Soft tissue calcifications
Tertiary hyperparathyroidism
Allow 12 months to elapse following
transplant as many cases will resolve
The presence of an autonomously
functioning parathyroid gland may require surgery. If the culprit gland can be
identified then it should be excised. Otherwise total parathyroidectomy and
re-implantation of part of the gland may be required.
References
1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art
Surgical Management. Surg
Clin North Am 2009 Oct;89(5):1227-39.
2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J Endocrinol 2011; 2011: 251410.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Pregnancy: thyroid problems
In pregnancy, there is an increase in the levels of
thyroxine-binding globulin (TBG). This causes an increase in the levels of total
thyroxine but does not affect the free thyroxine level.
Thyrotoxicosis
Untreated thyrotoxicosis increases
the risk of fetal loss, maternal heart failure and premature labour
Graves' disease is the most common
cause of thyrotoxicosis in pregnancy. It is also recognised that activation of
the TSH receptor by HCG may also occur - often termed transient gestational
hyperthyroidism. HCG levels will fall in the second and third trimester
Management
·
propylthiouracil has traditionally been the antithyroid drug of
choice
·
however, propylthiouracil is associated with an increased risk
of severe hepatic injury
·
therefore NICE Clinical Knowledge Summaries advocate the
following: 'Propylthiouracil is used in
the first trimester of pregnancy in place of carbimazole, as the latter drug
may be associated with an increased risk of congenital abnormalities. At the
beginning of the second trimester, the woman should be switched back to
carbimazole'
·
maternal free thyroxine levels should be kept in the upper third
of the normal reference range to avoid fetal hypothyroidism
·
thyrotrophin receptor stimulating antibodies should be checked
at 30-36 weeks gestation - helps to determine the risk of neonatal thyroid
problems
·
block-and-replace regimes should not be used in pregnancy
·
radioiodine therapy is contraindicated
Hypothyroidism
Key points
·
thyroxine is safe during pregnancy
·
serum thyroid-stimulating hormone measured in each trimester and
6-8 weeks post-partum
·
women require an increased dose of thyroxine during pregnancy
o by up to 50% as early as 4-6 weeks of pregnancy
·
breastfeeding is safe whilst on thyroxine
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Addison's disease: management
Patients who have Addison's disease
are usually given both glucocorticoid and mineralocorticoid replacement
therapy.
This usually means that patients
take a combination of:
·
hydrocortisone: usually given in 2 or 3 divided doses. Patients
typically require 20-30 mg per day, with the majority given in the morning dose
·
fludrocortisone
Patient education is important:
·
emphasise the importance of not missing glucocorticoid doses
·
consider MedicAlert bracelets and steroid cards
·
discuss how to adjust the glucocorticoid dose during an
intercurrent illness (see below)
Management of intercurrent illness
·
in simple terms the glucocorticoid dose should be doubled
·
the Addison's Clinical Advisory Panel have produced guidelines
detailing particular scenarios - please see the CKS link for more details
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:58
Subacute (De Quervain's) thyroiditis
Subacute thyroiditis (also known as
De Quervain's thyroiditis and subacute granulomatous thyroiditis) is thought to
occur following viral infection and typically presents with hyperthyroidism.
There are typically 4 phases;
·
phase 1 (lasts 3-6 weeks): hyperthyroidism, painful goitre, raised ESR
·
phase 2 (1-3 weeks): euthyroid
·
phase 3 (weeks - months): hypothyroidism
·
phase 4: thyroid structure and function goes back to normal
Investigations
·
thyroid scintigraphy: globally reduced uptake of
iodine-131
Management
·
usually self-limiting - most patients do not require treatment
·
thyroid pain may respond to aspirin or other NSAIDs
·
in more severe cases steroids are used, particularly if
hypothyroidism develops
|
|
|
|
|
|
Venn diagram showing how different causes of thyroid
dysfunction may manifest. Note how many causes of hypothyroidism may have an
initial thyrotoxic phase.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Hyperosmolar hyperglycaemic state
Hyperosmolar hyperglycaemic state
(HHS) is a medical emergency which is extremely difficult to manage and has a
significant associated mortality. Hyperglycaemia results in osmotic diuresis,
severe dehydration, and electrolyte deficiencies. HHS typically presents in the
elderly with type 2 diabetes mellitus (T2DM), however the incidence in younger
adults is increasing. It can be the initial presentation of T2DM.
It is extremely important to
differentiate HHS from diabetic ketoacidosis (DKA) as the management is
different, and treatment of HHS with insulin (e.g. as part of a DKA protocol)
can result in adverse outcomes. The first 24 hours of treatment is very labour
intensive so these patients are best managed in either a medical high
dependency unit.
HHS has a higher mortality than DKA
and may be complicated by vascular complications such as myocardial infarction,
stroke or peripheral arterial thrombosis. Seizures, cerebral oedema and central
pontine myelinolysis (CPM) are uncommon but documented complications of HHS.
Whilst DKA presents within hours of onset, HHS comes on over many days, and
consequently the dehydration and metabolic disturbances are more extreme.
Pathophysiology
·
Hyperglycaemia results in osmotic diuresis with associated loss
of sodium and potassium
·
Severe volume depletion results in a significant raised serum
osmolarity (typically > than 320 mosmol/kg), resulting in hyperviscosity of
blood.
·
Despite these severe electrolyte losses and total body volume
depletion, the typical patient with HHS, may not look as dehydrated as they
are, because hypertonicity leads to preservation of intravascular volume.
Clinical features
·
General: fatigue, lethargy, nausea and vomiting
·
Neurological: altered level of consciousness, headaches,
papilloedema, weakness
·
Haematological: hyperviscosity (may result in myocardial
infarctions, stroke and peripheral arterial thrombosis)
·
Cardiovascular: dehydration, hypotension, tachycardia
Diagnosis
·
1. Hypovolaemia
·
2. Marked Hyperglycaemia (>30 mmol/L) without significant ketonaemia
or acidosis
·
3. Significantly raised serum osmolarity (> 320 mosmol/kg)
·
Note: A precise definition of HHS does not exist, however the
above 3 criteria are helpful in distinguishing between HHS and DKA. It is also
important to remember that a mixed HHS / DKA picture can occur.
Management
The goals of management of HHS can
be summarised as follows:
·
1. Normalise the osmolality (gradually)
·
2. Replace fluid and electrolyte losses
·
3. Normalise blood glucose (gradually)
Fluid replacement
·
Fluid losses in HHS are estimated to be between 100 - 220 ml/kg
(e.g. 10-22 litres in an individual weighing 100 kg).
·
The rate of rehydration will be determined by assessing the
combination of initial severity and any pre-existing co-morbidities (e.g. heart
failure and chronic kidney disease). Caution is needed, particularly in the
elderly, where too rapid rehydration may precipitate heart failure but
insufficient may fail to reverse an acute kidney injury.
·
Intravenous (IV) 0.9% sodium chloride solution is the first line
fluid for restoring total body fluid.
·
It is important to remember that isotonic 0.9% sodium chloride
solution is already relatively hypotonic compared to the serum in someone with
HHS. Therefore in most cases it is very effective at restoring normal serum
osmolarity.
·
If the serum osmolarity is not declining despite positive
balance with 0.9% sodium chloride, then the fluid should be switched to 0.45%
sodium chloride solution which is more hypotonic relative to the HHS patients
serum osmolarity
·
IV fluid replacement should aim to achieve a positive balance of
3-6 litres by 12 hours and the remaining replacement of estimated fluid losses
within the next 12 hours.
·
Existing guidelines encourage vigorous initial fluid replacement
and this alone (without insulin) will result in a gradual decline in plasma
glucose and serum osmolarity. A rapid decline is potentially harmful (see
below) therefore insulin should NOT be used in the first instance unless there
is significant ketonaemia or acidosis
·
The aim of treatment should be to replace approximately 50% of
estimated fluid loss within the first 12 hours and the remainder in the following
12 hours. However this is just a guide, and clinical judgement should be
applied, particularly in patient with co-morbidities such as heart failure and
chronic kidney disease (which may limit the speed of correction).
Monitoring response to treatment
·
The key parameter in managing HHS is the osmolality to which
glucose and sodium are the main contributors. Rapid changes of serum osmolarity
are dangerous and can result in cardiovascular collapse and central pontine
myelinolysis (CPM).
·
Guidelines suggest that serum osmolarity, sodium and glucose
levels should be plotted on a graph to permit appreciation of the rate of
change. They should be plotted hourly initially.
·
Not all laboratories have readily available access to serum
osmolarity measurements. If not available then a calculated osmolarity can be
estimated with 2Na + glucose + urea
·
Fluid replacement alone (without insulin) will gradually lower
blood glucose which will reduce osmolality
·
A reduction of serum osmolarity will cause a shift of water into
the intracellular space. This inevitably results in a rise in serum sodium (a
fall in blood glucose of 5.5 mmol/L will result in a 2.4 mmol/L rise in
sodium). This is not necessarily an indication to give hypotonic solutions. If
the inevitable rise in serum Na+ is much greater than 2.4 mmol/L for each 5.5
mmol/L fall in blood glucose this would suggest insufficient fluid replacement.
Rising sodium is only a concern if the osmolality is NOT declining
concurrently.
·
Rapid changes must be avoided. A safe rate of fall of plasma
glucose of between 4 and 6 mmol/hr is recommended. The rate of fall of plasma
sodium should not exceed 10 mmol/L in 24 hours.
·
A target blood glucose of between 10 and 15 mmol/L is a
reasonable goal.
·
Complete normalisation of electrolytes and osmolality may take
up to 72 hours.
Insulin
·
Fluid replacement alone with 0.9% sodium chloride solution will
result in a gradual decline of blood glucose and osmolarity
·
Because most patients with HHS are insulin sensitive (e.g. it
usually occurs in T2DM), administration of insulin can result in a rapid
decline of serum glucose and thus osmolarity.
·
Insulin treatment prior to adequate fluid replacement may result
in cardiovascular collapse as the water moves out of the intravascular space,
with a resulting decline in intravascular volume.
·
A steep decline in serum osmolarity may also precipitate CPM.
·
Measurement of ketones is essential for determining if insulin
is required.
·
If significant ketonaemia is present (3β-hydroxy butyrate is
more than 1 mmol/L) this indicates relative hypoinsulinaemia and insulin should
be started at time zero (e.g. mixed DKA / HHS picture). The recommended insulin
dose is a fixed rate intravenous insulin infusion given at 0.05 units per kg
per hour.
·
If significant ketonaemia is not present (3β-hydroxy butyrate is
less than 1 mmol/L) then do NOT start insulin.
Potassium
·
Patients with HHS are potassium deplete but less acidotic than
those with DKA so potassium shifts are less pronounced
·
Hyperkalaemia can be present with acute kidney injury
·
Patients on diuretics may be profoundly hypokalaemic
·
Potassium should be replaced or omitted as required
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Hypoglycaemia
Causes
·
insulinoma - increased ratio of proinsulin to insulin
·
self-administration of insulin/sulphonylureas
·
liver failure
·
Addison's disease
·
alcohol
Other possible causes in children
·
nesidioblastosis - beta cell hyperplasia
Physiological response to
hypoglycaemia
·
hormonal response: the first response of the body is decreased
insulin secretion. This is followed by increased glucagon
secretion. Growth hormone
and cortisol are also released but later
·
sympathoadrenal response: increased catecholamine-mediated
(adrenergic) and acetylcholine-mediated (cholinergic) neurotransmission in the
peripheral autonomic nervous system and in the central nervous system
From <https://www.passmedicine.com/review/textbook.php?s=#>
Causes
of hypoglycaemia can be remembered by the mnemonic EXPLAIN
·
Exogenous drugs
(typically sulfonylureas or insulin)
·
Pituitary
insufficiency
·
Liver failure
·
Addison's disease
·
Islet cell tumours
(insulinomas)
·
Non-pancreatic
neoplasms
From <https://www.passmedicine.com/question/questions.php?q=0>
EXPLAIN:
·
Exogenous drugs such
alcohol, aspirin poisoning, pentamidine, quinine sulfate, ACE-inhibitor
·
Pituitary
insufficiency
·
Liver failure
·
Addison's disease
·
Islet cell tumours eg
insulinoma
·
Non-pancreatic
neoplasms
From <https://www.passmedicine.com/question/questions.php?q=0>
From <https://www.passmedicine.com/question/questions.php?q=0>
24 December 2020
13:59
MODY
·
MODY is a rare form of
diabetes often termed monogenic with an autosomal dominant inheritance.
The key features of MODY
are:
·
Being diagnosed with
diabetes under the age of 25.
·
Absence of
ketoacidosis
·
Having a parent with
diabetes, with diabetes in two or more generations.
·
Not necessarily
requiring insulin.
MODY is very rare
compared with type 1 and type 2 diabetes – experts estimate that only 1–2% of
people with diabetes (20-40,000 people) in the UK have it. But because MODY is
so rare, doctors may not be aware of it, so it’s estimated that about 90% of
people with it are mistakenly diagnosed with type 1 or type 2 diabetes at first.
There are many genes
identified with MODY. Some of the known genes are
HNF 1 Alpha, HNF 4
Alpha, HNF 1 Beta and Glucokinase
Maturity-onset diabetes of the young (MODY) is characterised by
the development of type 2 diabetes mellitus in patients < 25 years old. It
is typically inherited as an autosomal
dominant condition. Over six different genetic mutations have so
far been identified as leading to MODY.
It is thought that around 1-2% of patients with diabetes
mellitus have MODY, and around 90% are misclassified as having either type 1 or
type 2 diabetes mellitus.
MODY 3
·
60% of cases
·
due to a defect in the HNF-1 alpha gene
·
is associated with an increased risk of HCC
MODY 2
·
20% of cases
·
due to a defect in the glucokinase gene
MODY 5
·
rare
·
due to a defect in the HNF-1 beta gene
·
liver and renal cysts
Features of MODY
·
typically develops in patients < 25 years
·
a family history of early onset diabetes is often present
·
ketosis is not a feature at presentation
·
patients with the most common form are very sensitive to
sulfonylureas, insulin is not usually necessary
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Myxoedema coma
Myxoedema coma typically presents
with confusion and hypothermia.
Myxoedema coma is a medical
emergency requiring treatment with
·
IV thyroid replacement
·
IV fluid
·
IV corticosteroids (until the possibility of
coexisting adrenal insufficiency has been excluded)
·
electrolyte imbalance correction
·
sometimes rewarming
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Pituitary adenoma
A pituitary adenoma is a benign
tumour of the pituitary gland. They are common (10% of all people1) but in most
cases will never be found (asymptomatic) or are found as an incidental finding.
They account for around 10% of adult brain tumours2.
It is recommended that all patients with
a pituitary incidentaloma, including those without symptoms, undergo clinical
and laboratory evaluations for hormone hypersecretion and hypopituitarism.
Pituitary adenomas can be
classified according to:
·
size (a microadenoma is <1cm and a macroadenoma is >1cm)
·
hormonal status (a secretory/functioning adenoma
produces and excess of a particular hormone and a non-secretory/functioning
adenoma does not produce a hormone to excess)
Prolactinomas are the most common
type and they produce an excess of prolactin. After prolactinomas,
non-secreting adenomas are the next most common, then GH secreting and then
ACTH secreting adenomas.
Pituitary adenomas typically cause
symptoms by:
·
excess of a hormone (e.g. Cushing’s disease due to excess ACTH,
acromegaly due to excess GH or amenorrhea and galactorrhea due to excess
prolactin)
·
depletion of a hormone(s) (due to compression
of the normal functioning pituitary gland)
o non-functioning tumours, therefore,
present with generalised hypopituitarism
·
stretching of the dura within/around pituitary fossa (causing
headaches)
·
compression of the optic chiasm (causing a bitemporal hemianopia due to crossing nasal fibers)
Alternatively, pituitary adenomas,
particularly microadenomas, can be an incidental finding on neuroimaging and
therefore called a ‘pituitary incidentaloma’.
Investigation requires:
·
a pituitary blood profile (including: GH, prolactin, ACTH, FH, LSH
and TFTs)
·
formal visual field testing
·
MRI brain with contrast
Differential diagnoses include:
·
pituitary hyperplasia
·
craniopharyngioma
·
meningioma
·
brain metastases
·
lymphoma
·
hypophysitis
·
vascular malformation (e.g. aneurysm)
Treatment may include a combination
of:
·
hormonal therapy (e.g. bromocriptine is the first line treatment
for prolactinomas)
·
surgery (e.g. transsphenoidal transnasal hypophysectomy)
o e.g. if progression
in size
·
radiotherapy
From <https://www.passmedicine.com/review/textbook.php?s=#>
criteria
for surgical removal of a pituitary mass:
·
A visual field deficit
due to the lesion.
·
Other visual abnormalities,
such as ophthalmoplegia or neurological compromise due to compression by the
lesion.
·
Lesion abutting or
compressing the optic nerves or chiasm on MRI.
·
Pituitary apoplexy
with visual disturbance.
·
Hypersecreting tumours
other than prolactinomas
From <https://www.passmedicine.com/question/questions.php?q=0>
24 December 2020
13:59
Prolactin and galactorrhoea
Prolactin is secreted by the anterior pituitary gland with
release being controlled by a wide variety of physiological factors. Dopamine acts as the primary prolactin releasing inhibitory
factor and hence dopamine agonists such as bromocriptine may be used to control
galactorrhoea. It is important to differentiate the causes of galactorrhoea
(due to the actions of prolactin on breast tissue) from those of gynaecomastia
Features of excess prolactin
·
men: impotence, loss of libido, galactorrhoea
·
women: amenorrhoea, galactorrhoea
Causes of raised prolactin
·
prolactinoma
·
pregnancy
·
oestrogens
·
physiological: stress, exercise, sleep
·
acromegaly: 1/3 of patients
·
polycystic ovarian syndrome
·
primary hypothyroidism (due to thyrotrophin releasing hormone
(TRH) stimulating prolactin release)
Drug causes of raised prolactin
·
metoclopramide, domperidone
·
phenothiazines
·
haloperidol
·
very rare: SSRIs, opioids
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Sick euthyroid syndrome
In sick euthyroid syndrome (now
referred to as non-thyroidal illness) it is often said that everything (TSH,
thyroxine and T3) is low. In the majority of cases however the TSH level is within the
>normal range (inappropriately normal given
the low thyroxine and T3).
Changes are reversible upon
recovery from the systemic illness and hence no treatment is
usually needed.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Thyroid disorders: a very basic introduction
Disorders of thyroid function are
very commonly encountered in clinical practice. Around 2% of the UK population
has hypothyroidism (an under active thyroid gland) whilst around 1% have
thyrotoxicosis (an over active gland). Both hypothyroidism and hyperthyrodism
(also known as thyrotoxicosis) are around 10 times more common in women than
men.
Structure and function
The thyroid gland is one of the
largest endocrine organs in the body. It is a bi-lobed structure which is found
in the anterior neck. As with many endocrine organs, it is part of a
hypothalamus-pituitary-end organ system with negative feedback cycles to
maintain normal circulating levels of the hormone, in this case thyroxine and triiodothyronine.
On a simple level the hypothalamus
secretes thyrotropin-releasing hormone (TRH) which stimulates the anterior
pituitary to secrete thyroid-stimulating hormone (TSH). This then acts on the
thyroid gland increasing the production of thyroxine (T4) and triiodothyronine
(T3), the two main thyroid hormones. These then act on a wide variety of
tissues, helping to regulate the use of energy sources, protein synthesis, and
controls the body's sensitivity to other hormones.
How are thyroid problems
classified?
Hypothyroidism may be classified as
follows:
·
primary hypothyroidism: there is a problem with the thyroid
gland itself, for example an autoimmune disorder affecting thyroid tissue (see
below)
·
secondary hypothyroidism: usually due to a disorder with the
pituitary gland (e.g.pituitary apoplexy) or a lesion compressing the pituitary
gland
·
congenital hypothyroidism: due to a problem with thyroid
dysgenesis or thyroid dyshormonogenesis
Whilst there are a number of causes
thyrotoxicosis the vast majority are primary in nature. Congenital
thyrotoxicosis is not seen and secondary hyperthyroidism is rare, account for
less than 1% of cases.
What causes thyroid problems?
The majority of thyroid problems
seen in the developed world are a consequence of autoimmunity.
The table below shows the different
autoimmune problems which cause thyroid dysfunction:
|
|
Hypothyroidism |
Thyrotoxicosis |
|
Most common cause |
Hashimoto's thyroiditis ·
most common cause in the developed world ·
autoimmune disease, associated with type 1 diabetes
mellitus, Addison's or pernicious anaemia ·
may cause transient thyrotoxicosis in the acute
phase ·
5-10 times more common in women |
Graves' disease ·
most common cause of thyrotoxicosis ·
as well as typically features of thyrotoxicosis
other features may be seen including thyroid eye disease |
|
Other causes |
Subacute thyroiditis (de Quervain's) ·
associated with a painful goitre and raised ESR Riedel thyroiditis ·
fibrous tissue replacing the normal thyroid
parenchyma ·
causes a painless goitre Postpartum thyroiditis Drugs ·
lithium ·
amiodarone Iodine deficiency ·
the most common cause of hypothyroidism in the
developing world |
Toxic multinodular goitre ·
autonomously functioning thyroid nodules that
secrete excess thyroid hormones Drugs ·
amiodarone |
It should be remembered that a lot
of the conditions mentioned above don't always cause either hypothyroidism or
hyperthyroidism, there is sometimes some overlap, as shown below:
|
|
|
|
|
|
Venn diagram showing how different causes of thyroid
dysfunction may manifest. Note how many causes of hypothyroidism may have an
initial thyrotoxic phase.
Symptoms and signs
Thyroid disorders can present in a
large variety of ways. Often (but not always) the symptoms present are the
opposite depending on whether the thyroid gland is under or over active, for
example hypothyroidism may result in weight gain whilst thyrotoxicosis normally
leads to weight loss
|
Feature |
Hypothyroidism |
Thyrotoxicosis |
|
General |
Weight gain Lethargy Cold intolerance |
Weight loss 'Manic', restlessness Heat intolerance |
|
Cardiac |
- |
Palpitations, may even provoke arrhythmias e.g. atrial
fibrillation |
|
Skin |
Dry (anhydrosis), cold, yellowish skin Non-pitting oedema (e.g. hands, face) Dry, coarse scalp hair, loss of lateral
aspect of eyebrows |
Increased sweating Pretibial myxoedema: erythematous,
oedematous lesions above the lateral malleoli Thyroid acropachy: clubbing |
|
Gastrointestinal |
Constipation |
Diarrhoea |
|
Gynaecological |
Menorrhagia |
Oligomenorrhea |
|
Neurological |
Decreased deep tendon reflexes Carpal tunnel syndrome |
Anxiety Tremor |
Investigations and diagnosis
The principle investigation is
'thyroid function tests', or TFTs for short:
·
these primarily look at serum TSH and T4 levels
·
T3 can be measured but is only useful clinically in a small
number of cases
·
remember that TSH and T4 levels will often be 'opposite' in
cases of primary hypo- or hyperthyroidism. For example in hypothyroidism the T4
level is low (i.e. not enough thyroxine) but the TSH level is high, because the
hypothalamus/pituitary has detected low levels of T4 and is trying to get the
thyroid gland to produce more
·
TSH levels are more sensitive than T4 levels for monitoring
patients with existing thyroid problems and are often used to guide treatment
The table below shows how thyroid
function tests are interpreted:
|
Diagnosis |
TSH |
Free T4 |
Notes |
|
Thyrotoxicosis (e.g. Graves' disease) |
Low |
High |
|
|
Primary hypothyroidism (e.g. Hashimoto's thyroiditis) |
High |
Low |
|
|
Secondary hypothyroidism |
Low |
Low |
|
|
Sick euthyroid syndrome |
Low |
Low |
Common in hospital inpatients. Changes
are reversible upon recovery from the systemic illness and no treatment is
usually needed |
|
Subclinical hypothyroidism |
High |
Normal |
This is a common finding and represents
patients who are 'on the way' to developing hypothyroidism but still have
normal thyroxine levels. Note how the TSH levels, as mentioned above, are a
more sensitive and early marker of thyroid problems |
|
Poor compliance with
thyroxine |
High |
Normal |
Patients who are poorly compliant may
only take their thyroxine in the days before a routine blood test. The
thyroxine levels are hence normal but the TSH 'lags' and reflects longer term
low thyroxine levels |
A number of thyroid autoantibodies
can be tested for (remember the majority of thyroid disorders are autoimmune).
The 3 main types are:
·
Anti-thyroid peroxidase (anti-TPO) antibodies
·
TSH receptor antibodies
·
Thyroglobulin antibodies
There is significant overlap
between the type of antibodies present and particular diseases, but generally
speaking TSH
receptor antibodies are present in around 90-100% of patients with Graves'
disease and anti-TPO
antibodies are seen in around 90% of patients with Hashimoto's thyroiditis.
Other tests include:
·
nuclear scintigraphy; toxic multinodular goitre reveals patchy
uptake
Treatment
This clearly depends on the cause.
For patients with hypothyrodism thyroxine is given in the form of levothyroxine
to replace the underlying deficiency.
Patients with thyrotoxicosis may be
treated with:
·
propranolol: this is often used at the time of diagnosis to
control thyrotoxic symptoms such as tremor
·
carbimazole: blocks thyroid peroxidase from coupling and
iodinating the tyrosine residues on thyroglobulin → reducing thyroid hormone
production. Agranulocytosis is an important adverse effect to be aware of
·
radioiodine treatment
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Acromegaly: management
Trans-sphenoidal surgery is the
first-line treatment for acromegaly in the majority of patients.
If a pituitary tumour is inoperable
or surgery unsuccessful then medication may be indicated:
·
somatostatin analogue
o directly inhibits the release of
growth hormone
o for example octreotide
o effective in 50-70% of patients
·
pegvisomant
o GH receptor antagonist - prevents
dimerization of the GH receptor
o once daily s/c administration
o very effective - decreases IGF-1
levels in 90% of patients to normal
o doesn't reduce tumour volume
therefore surgery still needed if mass effect
·
dopamine agonists
o for example bromocriptine
o the first effective medical
treatment for acromegaly, however now superseded by somatostatin analogues
o effective only in a minority of
patients
External irradiation is sometimes
used for older patients or following failed surgical/medical treatment
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Addison's disease: investigations
In a patient with suspected
Addison's disease the definite investigation is an ACTH stimulation test (short
Synacthen test). Plasma cortisol is measured
before and 30 minutes after giving Synacthen 250ug IM. Adrenal autoantibodies
such as anti-21-hydroxylase may also be demonstrated.
If an ACTH stimulation test is not
readily available (e.g. in primary care) then sending a 9 am serum cortisol can
be useful:
·
> 500 nmol/l makes Addison's very unlikely
·
< 100 nmol/l is definitely abnormal
·
100-500 nmol/l should prompt a ACTH stimulation test to be
performed
Associated electrolyte
abnormalities are seen in around one-third of undiagnosed patients:
·
hyperkalaemia
·
hyponatraemia
·
hypoglycaemia
·
metabolic acidosis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:59
Carbimazole
Carbimazole is used in the
management of thyrotoxicosis. It is typically given in high doses for 6 weeks
until the patient becomes euthyroid before being reduced.
Mechanism of action
·
blocks thyroid peroxidase from coupling and iodinating the
tyrosine residues on thyroglobulin → reducing thyroid hormone production
·
in contrast propylthiouracil as well as this central mechanism
of action also has a peripheral action by inhibiting 5'-deiodinase which
reduces peripheral conversion of T4 to T3
Adverse effects
·
agranulocytosis
·
crosses the placenta, but may be used in low doses during
pregnancy
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Cushing's syndrome: causes
It should be noted that exogenous
causes of Cushing's syndrome (e.g. glucocorticoid therapy) are far more common
than endogenous ones.
ACTH dependent causes
·
Cushing's disease (80%): pituitary
tumour secreting ACTH producing adrenal hyperplasia
·
ectopic ACTH production (5-10%): e.g. small
cell lung cancer is the most common causes
ACTH independent causes
·
iatrogenic: steroids
·
adrenal adenoma (5-10%)
·
adrenal carcinoma (rare)
·
Carney complex: syndrome including cardiac myxoma
·
micronodular adrenal dysplasia (very rare)
Pseudo-Cushing's
·
mimics Cushing's
·
often due to alcohol excess or severe depression
·
causes false positive dexamethasone suppression test or 24 hr
urinary free cortisol
·
insulin stress test may be used to differentiate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
DVLA: diabetes mellitus
Until recently people with diabetes
who used insulin could not hold a HGV licence. The DVLA changed the rules in
October 2011. The following standards need to be met (and also apply to
patients using other hypoglycaemic inducing drugs such as sulfonylureas):
·
there has not been any severe hypoglycaemic event in the
previous 12 months
·
the driver has full hypoglycaemic awareness
·
the driver must show adequate control of the condition by
regular blood glucose monitoring*, at least twice daily and at times relevant
to driving
·
the driver must demonstrate an understanding of the risks of
hypoglycaemia
·
here are no other debarring complications of diabetes
From a practical point of view
patients on insulin who want to apply for a Group 2 (HGV) licence need to
complete a VDIAB1I form.
Other specific points for group 1
drivers:
·
if on insulin then patient can drive a car as long as they have
hypoglycaemic awareness, not more than one episode of hypoglycaemia requiring
the assistance of another person within the preceding 12 months and no relevant
visual impairment. Drivers are normally contacted by DVLA
·
if on tablets or exenatide no need to notify DVLA. If tablets
may induce hypoglycaemia (e.g. sulfonylureas) then there must not have been
more than one episode of hypoglycaemia requiring the assistance of another
person within the preceding 12 months
·
if diet controlled alone then no requirement to inform DVLA
*to demonstrate adequate control,
the Secretary of State's Honorary Medical Advisory Panel on Diabetes Mellitus
has recommended that applicants will need to have used blood glucose meters
with a memory function to measure and record blood glucose levels for at least
3 months prior to submitting their application
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Hypothyroidism: features
General
·
Weight gain
·
Lethargy
·
Cold intolerance
Skin
·
Dry (anhydrosis), cold, yellowish skin
·
Non-pitting oedema (e.g. hands, face)
·
Dry, coarse scalp hair, loss of lateral aspect of eyebrows
Gastrointestinal
·
Constipation
Gynaecological
·
Menorrhagia
Neurological
·
Decreased deep tendon reflexes
·
Carpal tunnel syndrome
A hoarse voice is also occasionally
noted.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Kallmann's syndrome
Kallmann's syndrome is a recognised
cause of delayed puberty secondary to hypogonadotropic hypogonadism. It is
usually inherited as an X-linked recessive trait. Kallmann's syndrome is
thought to be caused by failure
of GnRH-secreting neurons to migrate to the hypothalamus.
The clue given in many questions is
lack of smell (anosmia) in a boy with delayed puberty.
Features
·
'delayed puberty'
·
hypogonadism, cryptorchidism
·
anosmia
·
sex hormone levels are low
·
LH, FSH levels are inappropriately low/normal
·
patients are typically of normal or above average height
Cleft lip/palate and visual/hearing
defects are also seen in some patients
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Klinefelter's syndrome
Klinefelter's syndrome is
associated with karyotype
47, XXY.
Features
·
often taller than average
·
lack of secondary sexual characteristics
·
small, firm testes
·
infertile
·
gynaecomastia - increased incidence of breast cancer
·
elevated gonadotrophin levels but low
testosterone
Diagnosis is by karyotype (chromosomal analysis).
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Obesity: therapeutic options
The management of obesity consists
of a step-wise approach:
·
conservative: diet, exercise
·
medical
·
surgical
Orlistat is a pancreatic lipase inhibitor used in the management of obesity. Adverse effects include
faecal urgency/incontinence and flatulence. A lower dose version is now
available without prescription ('Alli'). NICE have defined criteria for the use
of orlistat. It should only be prescribed as part of an overall plan for
managing obesity in adults who have:
·
BMI of 28 kg/m^2 or more with associated risk factors, or
·
BMI of 30 kg/m^2 or more
·
continued weight loss e.g. 5% at 3 months
·
orlistat is normally used for < 1 year
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Prediabetes and impaired glucose regulation
Prediabetes is a term which is
increasingly used where there is impaired glucose levels which are above the
normal range but not high enough for a diagnosis of diabetes mellitus. The term
includes patients who have been labelled as having either impaired fasting
glucose (IFG) or impaired glucose tolerance (IGT). Diabetes UK estimate that
around 1 in 7 adults in the UK have prediabetes. Many individuals with
prediabetes will progress on to developing type 2 diabetes mellitus (T2DM) and
they are therefore at greater risk of microvascular and macrovascular
complications.
Terminology
·
Diabetes UK currently recommend using the term prediabetes when
talking to patients and impaired glucose regulation when talking to other
healthcare professionals
·
research has shown that the term 'prediabetes' has the most
impact and is most easily understood
Identification of patients with
prediabetes
·
NICE recommend using a validated computer based risk assessment
tool for all adults aged 40 and over, people of South Asian and Chinese descent
aged 25-39, and adults with conditions that increase the risk of type 2 diabetes
·
patients identified at high risk should have a blood sample
taken
·
a fasting plasma glucose of 6.1-6.9 mmol/l or an HbA1c level of
42-47 mmol/mol (6.0-6.4%) indicates high risk
|
|
|
|
|
|
Diagram showing the spectrum of diabetes diagnosis
Management
·
lifestyle modification: weight loss, increased exercise, change
in diet
·
at least yearly follow-up with blood tests is recommended
·
NICE recommend metformin for adults at high risk 'whose blood glucose measure (fasting plasma glucose or HbA1c)
shows they are still progressing towards type 2 diabetes, despite their
participation in an intensive lifestyle-change programme'
Impaired fasting glucose and
impaired glucose tolerance
There are two main types of IGR:
·
impaired fasting glucose (IFG) - due to hepatic insulin
resistance
·
impaired glucose tolerance (IGT) - due to muscle insulin
resistance
·
patients with IGT are more likely to develop T2DM and
cardiovascular disease than patients with IFG
Definitions
·
a fasting glucose greater than or equal to 6.1 but less than 7.0
mmol/l implies impaired fasting glucose (IFG)
·
impaired glucose tolerance (IGT) is defined as fasting plasma
glucose less than 7.0 mmol/l and OGTT 2-hour value greater than or equal to 7.8
mmol/l but less than 11.1 mmol/l
·
people with IFG should then be offered an oral glucose tolerance
test to rule out a diagnosis of diabetes. A result below 11.1 mmol/l but above
7.8 mmol/l indicates that the person doesn't have diabetes but does have IGT
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Subclinical hypothyroidism
Basics
·
TSH raised but T3, T4 normal
·
no obvious symptoms
Significance
·
risk of progressing to overt hypothyroidism is 2-5% per year
(higher in men)
·
risk increased by the presence of thyroid
autoantibodies
Management
Not all patients require treatment.
NICE Clinical Knowledge Summaries (CKS) have produced guidelines. Note that not
all patients will fall within the age boundaries given and hence these are
guidelines in the broader sense.
TSH is between 4 - 10mU/L and the
free thyroxine level is within the normal range
·
if < 65 years with symptoms suggestive of hypothyroidism,
give a trial of levothyroxine. If there is no improvement in symptoms, stop
levothyroxine
·
'in older people (especially those aged over 80 years) follow a
'watch and wait' strategy, generally avoiding hormonal treatment'
·
if asymptomatic people, observe and repeat thyroid function in 6
months
TSH is > 10mU/L and the free
thyroxine level is within the normal range
·
start treatment (even if asymptomatic) with levothyroxine if
<= 70 years
·
'in older people (especially those aged over
80 years) follow a 'watch and wait' strategy, generally avoiding hormonal treatment'
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Sulfonylureas
Sulfonylureas are oral
hypoglycaemic drugs used in the management of type 2 diabetes mellitus. They
work by increasing
pancreatic insulin secretion and hence are only effective if
functional B-cells are present. On a molecular level they bind to an ATP-dependent K+(KATP) channel on the cell membrane of pancreatic beta cells.
Common adverse effects
·
hypoglycaemic episodes (more common with long-acting
preparations such as chlorpropamide)
·
weight gain
Rarer adverse effects
·
hyponatraemia secondary to syndrome of inappropriate ADH secretion
·
bone marrow suppression
·
hepatotoxicity (typically cholestatic)
·
peripheral neuropathy
Sulfonylureas should be avoided in breastfeeding and pregnancy.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Thyroid eye disease
Thyroid eye disease affects between
25-50% of patients with Graves' disease.
Pathophysiology
·
it is thought to be caused by an autoimmune response against an
autoantigen, possibly the TSH receptor → retro-orbital inflammation
·
the inflammation results in glycosaminoglycan and collagen
deposition in the muscles
Prevention
·
smoking is the most important modifiable risk factor for the
development of thyroid eye disease
·
radioiodine treatment may increase the inflammatory symptoms
seen in thyroid eye disease. In a recent study of patients with Graves' disease
around 15% developed, or had worsening of, eye disease. Prednisolone may help
reduce the risk
Features
·
the patient may be eu-, hypo- or hyperthyroid at the time of
presentation
·
exophthalmos
·
conjunctival oedema
·
optic disc swelling
·
ophthalmoplegia
·
inability to close the eyelids may lead to sore, dry eyes. If
severe and untreated patients can be at risk of exposure keratopathy
Management
·
topical lubricants may be needed to help prevent corneal
inflammation caused by exposure
·
steroids
·
radiotherapy
·
surgery
Monitoring patients with
established thyroid eye disease
For patients with established
thyroid eye disease the following symptoms/signs should indicate the need for
urgent review by an ophthalmologist (see EUGOGO guidelines):
·
unexplained deterioration in vision
·
awareness of change in intensity or quality of colour vision in
one or both eyes
·
history of eye suddenly 'popping out' (globe subluxation)
·
obvious corneal opacity
·
cornea still visible when the eyelids are closed
·
disc swelling
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Toxic multinodular goitre
Toxic multinodular goitre describes
a thyroid gland that contains a number of autonomously functioning thyroid
nodules resulting in hyperthyroidism.
Nuclear scintigraphy reveals patchy
uptake.
The treatment of choice is radioiodine therapy.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:00
Acromegaly: investigations
Growth hormone (GH) levels vary
during the day and are therefore not diagnostic.
Serum IGF-1
levels have now overtaken the oral glucose tolerance test (OGTT) with
serial GH measurements as the first-line test. The OGTT test is recommended to confirm the diagnosis if IGF-1 levels are raised.
The Endocrine Society guidelines
suggest the following:
1.1 We recommend measurement of IGF-1 levels in patients
with typical clinical manifestations of acromegaly, especially those with acral
and facial features.
...
1.5 In patients with elevated or equivocal serum IGF-1
levels, we recommend confirmation of the diagnosis by finding lack of
suppression of GH to < 1 μg/L following documented hyperglycemia during an
oral glucose load.
Serum IGF-1 may also be used to
monitor disease
Oral glucose tolerance test
·
in normal patients GH is suppressed to < 2 mu/L with
hyperglycaemia
·
in acromegaly there is no suppression of GH
·
may also demonstrate impaired glucose tolerance which is
associated with acromegaly
A pituitary MRI may demonstrate a
pituitary tumour.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Combined deficiency of magnesium and calcium
Magnesium is required for both PTH
secretion and its action on target tissues. Hypomagnesaemia may both cause
hypocalcaemia and render patients unresponsive to treatment with calcium and
vitamin D supplementation.
Magnesium is the fourth most
abundant cation in the body. The body contains 1000mmol, with half contained in
bone and the remainder in muscle, soft tissues and extracellular fluid. There
is no one specific hormonal control of magnesium and various hormones including
PTH and aldosterone affect the renal handling of magnesium.
Magnesium and calcium interact at a
cellular level also and as a result decreased magnesium will tend to affect the
permeability of cellular membranes to calcium, resulting in hyperexcitability.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Congenital adrenal hyperplasia
Overview
·
group of autosomal recessive disorders
·
affect adrenal steroid biosynthesis
·
in response to resultant low cortisol levels the anterior
pituitary secretes high levels of ACTH
·
ACTH stimulates the production of adrenal androgens that may
virilize a female infant
Cause
·
21-hydroxylase deficiency (90%)
·
11-beta hydroxylase deficiency (5%)
·
17-hydroxylase deficiency (very rare)
|
|
|
|
Image
sourced from Wikipedia |
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Diabetes mellitus: Ramadan
We know that type 2 diabetes
mellitus is more common in people of Asian ethnicity and a significant
proportion of those patients in the UK will be Muslim. The BMJ published an
excellent and comprehensive review of this issue in 20101.
It is important that we can give
appropriate advice to Muslim patients to allow them safely observe their fast.
This is particularly important from 2014 as Ramadan is due to fall in the long
days of the summer months for several years henceforth.
Clearly it is a personal decision
whether a patient decides to fast. It may however be worthwhile exploring the
fact that people with chronic conditions are exempt from fasting or may be able
to delay fasting to the shorter days of the winter months. It is however known
that many Muslim patients with diabetes do not class themselves as having a
chronic/serious condition which should exempt them from fasting. Around 79% of Muslim patients with type 2 diabetes mellitus fast Ramadan2.There is an
excellent patient information leaflet from Diabetes UK and the Muslim Council
of Britain which explores these options in more detail.
If a patient with type 2 diabetes
mellitus does decide to fast:
·
they should try and and eat a meal containing long-acting
carbohydrates prior to sunrise (Suhoor)
·
patients should be given a blood glucose monitor to allow them
to check their glucose levels, particularly if they feel unwell
·
for patients taking metformin the expert consensus is that the
dose should be split one-third before sunrise (Suhoor) and two-thirds after sunset (Iftar)
·
expert consensus also recommends switching once-daily
sulfonylureas to after sunset. For patients taking twice-daily preparations
such as gliclazide it is recommended that a larger proportion of the dose is
taken after after sunset
·
no adjustment is needed for patients taking pioglitazone
1. Management of people with
diabetes wanting to fast during Ramadan BMJ 2010;340:c3053
2. Salti I et al. Results of the
Epidemiology of Diabetes and Ramadan (EPIDIAR) study. Diabetes Care
2004;27:2306-11.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Graves' disease: management
Despite many trials there is no
clear guidance on the optimal management of Graves' disease. Treatment options
include titration of anti-thyroid drugs (ATDs, for example carbimazole),
block-and-replace regimes, radioiodine treatment and surgery. Propranolol is
often given initially to block adrenergic effects
ATD titration
·
carbimazole is started at 40mg and reduced gradually to maintain
euthyroidism
·
typically continued for 12-18 months
·
patients following an ATD titration regime have been shown to
suffer fewer side-effects than those on a block-and-replace regime
Block-and-replace
·
carbimazole is started at 40mg
·
thyroxine is added when the patient is euthyroid
·
treatment typically lasts for 6-9 months
The major complication of
carbimazole therapy is agranulocytosis
Radioiodine treatment
·
contraindications include pregnancy (should be avoided for 4-6
months following treatment) and age < 16 years. Thyroid eye disease is a
relative contraindication, as it may worsen the condition
·
the proportion of patients who become hypothyroid depends on the
dose given, but as a rule the majority of patient will require thyroxine
supplementation after 5 years
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Growth hormone therapy
NICE guidance recommended growth
hormone therapy for the following indications
·
proven growth hormone deficiency
·
Turner's syndrome
·
Prader-Willi syndrome
·
chronic renal insufficiency before puberty
Key points
·
given by subcutaneous injection
·
treatment should be discontinued if there is a poor response in
the first year of therapy
Adverse effects
·
headache
·
benign intracranial hypertension
·
fluid retention
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Hypoparathyroidism
Primary hypoparathyroidism
·
decrease PTH secretion
·
e.g. secondary to thyroid surgery*
·
low calcium, high phosphate
·
treated with alfacalcidol
The main symptoms of
hypoparathyroidism are secondary to hypocalcaemia:
·
tetany: muscle twitching, cramping and spasm
·
perioral paraesthesia
·
Trousseau's sign: carpal spasm if the brachial artery occluded
by inflating the blood pressure cuff and maintaining pressure above systolic
·
Chvostek's sign: tapping over parotid causes facial muscles to
twitch
·
if chronic: depression, cataracts
·
ECG: prolonged QT interval
Pseudohypoparathyroidism
·
target cells being insensitive to PTH
·
due to abnormality in a G protein
·
associated with low IQ, short stature, shortened 4th and 5th
metacarpals
·
low calcium, high phosphate, high PTH
·
diagnosis is made by measuring urinary cAMP and phosphate levels
following an infusion of PTH. In hypoparathyroidism this will cause an increase
in both cAMP and phosphate levels. In pseudohypoparathyroidism type I neither
cAMP nor phosphate levels are increased whilst in pseudohypoparathyroidism type
II only cAMP rises.
Pseudopseudohypoparathyroidism
·
similar phenotype to pseudohypoparathyroidism but normal
biochemistry
*this may seem an oxymoron, but
most medical textbooks classify hypoparathyroidism which is secondary to
surgery as being 'primary hypoparathyroidism'
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Hypothyroidism: causes
Hypothyroidism affects around 1-2%
of women in the UK and is around 5-10 times more common in females than males.
Primary hypothyroidism
Hashimoto's thyroiditis
·
most common cause
·
autoimmune disease, associated with IDDM, Addison's or
pernicious anaemia
·
may cause transient thyrotoxicosis in the acute phase
·
5-10 times more common in women
Subacute thyroiditis (de
Quervain's)
Riedel thyroiditis
After thyroidectomy or radioiodine
treatment
Drug therapy (e.g. lithium,
amiodarone or anti-thyroid drugs such as carbimazole)
Dietary iodine deficiency
|
|
|
|
|
|
Venn diagram showing how different causes of thyroid
dysfunction may manifest. Note how many causes of hypothyroidism may have an
initial thyrotoxic phase.
Secondary hypothyroidism (rare)
From pituitary failure
Other associated conditions
·
Down's syndrome
·
Turner's syndrome
·
coeliac disease
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Insulin
Insulin is a peptide hormone,
produced by beta cells of the pancreas, and is central to regulating
carbohydrate and fat metabolism in the body. Insulin causes cells in the liver,
skeletal muscles, and fat tissue to absorb glucose from the blood. In the liver
and skeletal muscles, glucose is stored as glycogen, and in fat cells
(adipocytes) it is stored as triglycerides.
Structure
The human insulin protein is
composed of 51 amino acids, and has a molecular weight of 5808 Da. It is a
dimer of an A-chain and a B-chain, which are linked together by disulfide
bonds.
Synthesis
Pro-insulin is formed by the rough endoplasmic
reticulum in pancreatic beta cells. Then pro-insulin is cleaved to form insulin
and C-peptide. Insulin is stored in secretory granules and released in response
to Ca2+.
Function
Basics
·
Secreted in response to hyperglycaemia
·
Glucose utilisation and glycogen synthesis
·
Inhibits lipolysis
·
Reduces muscle protein loss
·
Increases cellular uptake of potassium (via stimulation of Na+/K+ ATPase pump)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Insulin stress test
Basics
·
used in investigation of hypopituitarism
·
IV insulin given, GH and cortisol levels measured
·
with normal pituitary function GH and cortisol should rise
Contraindications
·
epilepsy
·
ischaemic heart disease
·
adrenal insufficiency
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Insulin therapy
Insulin therapy revolutionised the
management of diabetes mellitus when it was developed in the 1920's. It is
still the only available treatment for type 1 diabetes mellitus (T1DM) and is
widely used in type 2 diabetes mellitus (T2DM) where oral hypoglycaemic agents
fail to gain adequate control.
It can sometimes seem daunting to understand
the various types of insulin but it is important you have a basic grasp to
avoid potential harm to patients.
Classification of insulin
By manufacturing process
·
porcine: extracted and purified from pig pancreas
·
human sequence insulin: either produced by enzyme modification
of porcine insulin (emp) or biosynthetically by recombinant DNA using bacteria
(crb, prb) or yeast (pyr)
·
analogues
By duration of action
|
|
Onset |
Peak |
Duration |
|
Rapid-acting insulin analogues |
5 mins |
1 hour |
3-5 hours |
|
Short-acting insulin |
30 mins |
3 hours |
6-8 hours |
|
Intermediate-acting insulin |
2 hours |
5-8 hours |
12-18 hours |
|
Long-acting insulin analogues |
1-2 hours |
Flat profile |
Up to 24 hours |
|
Premixed preparations |
- |
- |
- |
Patients often require a mixture of
preparations (e.g. both short and long acting) to ensure stable glycaemic
control throughout the day.
Rapid-acting insulin analogues
·
the rapid-acting human insulin analogues act faster and have a
shorter duration of action than soluble insulin (see below)
·
may be used as the bolus dose in 'basal-bolus' regimes
(rapid/short-acting 'bolus' insulin before meals with intermediate/long-acting
'basal' insulin once or twice daily)
·
insulin aspart: NovoRapid
·
insulin lispro: Humalog
Short-acting insulins
·
soluble insulin examples: Actrapid (human, pyr), Humulin S
(human, prb)
·
may be used as the bolus dose in 'basal-bolus' regimes
Intermidate-acting insulins
·
isophane insulin
·
many patients use isophane insulin in a premixed formulation
with
Long-acting insulins
·
insulin determir (Levemir): given once or twice daily
·
insulin glargine (Lantus): given once daily
Premixed preparations
·
combine intermediate acting insulin with either a rapid-acting
insulin analogue or soluble insulin
·
Novomix 30: 30% insulin aspart (rapid-acting), 70% insulin
aspart protamine (intermediate-acting)
·
Humalog Mix25: 25% insulin lispro (rapid-acting), 75% insulin
lispro protamine (intermediate-acting); Humalog Mix50: 50% insulin lispro, 50%
insulin lispro protamine
·
Humulin M3: biphasic isophane insulin (human, prb) - 30% soluble
(short-acting), 70% isophane (intermediate-acting)
·
Insuman Comb 15: biphasic isophane insulin 9human, prb) - 30%
soluble (short-acting), 70% isophane (intermediate-acting)
Administration of insulin
The vast majority of patients
administer insulin subcutaneously. It is important to rotate injection sites to
prevent lipodystrophy. Insulin pumps are available ('continuous subcutaneous
insulin infusions') which delivers a continuous basal infusion and a
patient-activated bolus dose at meal times.
Intravenous insulin is used for
patients who are acutely unwell, for example with diabetic ketoacidosis.
Inhaled insulin is available but not widely used and oral insulin analogues are
in development but have considerable technical hurdles to clear.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Insulinoma
An insulinoma is a neuroendocrine
tumour deriving mainly from pancreatic Islets of Langerhans cells
Basics
·
most common pancreatic endocrine tumour
·
10% malignant, 10% multiple
·
of patients with multiple tumours, 50% have MEN-1
Features
·
of hypoglycaemia: typically early in morning or just before
meal, e.g. diplopia, weakness etc
·
rapid weight gain may be seen
·
high insulin, raised proinsulin:insulin ratio
·
high C-peptide
Diagnosis
·
supervised, prolonged fasting (up to 72 hours)
·
CT pancreas
Management
·
surgery
·
diazoxide and somatostatin if patients are not candidates for
surgery
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
Prolactinoma
Prolactinomas are a type of
pituitary adenoma, a benign tumour of the pituitary gland.
Pituitary adenomas can be
classified according to:
·
size (a microadenoma is <1cm and a macroadenoma is
>1cm)
·
hormonal status (a secretory/functioning adenoma
produces and excess of a particular hormone and a non-secretory/functioning
adenoma does not produce a hormone to excess)
Prolactinomas are the most common
type and they produce an excess of prolactin.
Features of excess prolactin
·
men: impotence, loss of libido, galactorrhoea
·
women: amenorrhoea, infertility, galactorrhoea, osteoporosis
Diagnosis
·
MRI
Management
·
in the majority of cases, symptomatic patients are treated
medically with dopamine agonists (e.g. cabergoline, bromocriptine)
which inhibit the release of prolactin from the pituitary gland
·
surgery is performed for patients who cannot tolerate or fail to
respond to medical therapy. A trans-sphenoidal approach is generally preferred
unless there is a significant extra-pituitary extension
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:01
PTH
A hormone is a chemical messenger
which is secreted by an endocrine gland and designed to generate a specific
response by binding to a cellular receptor. This receptor may be intracellular
(commonly steroid hormone receptors) or on the cell surface membrane.
Parathyroid hormone (PTH) is a
polypeptide hormone secreted from the parathyroid gland. It has an important
role in calcium homeostasis. It acts on cell-surface receptors to generate a
coordinated response throughout the body and maintain blood calcium within a
narrow range.
It is vital that calcium does not
rise too high or fall too low, as hyper- and hypo- calcaemia can have serious
consequences. Calcium enters the body through the intestines and leaves through
urine and faeces. The main reservoir of calcium in the body is the bone,
containing about 1 kg of complexed calcium and phosphate. In the blood, calcium
exists in three main forms:
·
free calcium
·
bound to albumin
·
complexed with anions
It is free calcium which is
physiologically active and can travel into cells to exert a function.
Structure and function
PTH, a single-chain polypeptide
containing 84 amino acids, is secreted from the Chief cells of the parathyroid
glands, located on the posterior aspect of the thyroid. It is generated in
response to low levels of calcium in the blood, where it travels to effector
organs to increase levels of the electrolyte back to normal concentrations.
Effector organs associated with PTH
include the bone and kidney:
·
At the bone PTH acts to increase the activity
of osteoclastic cells, which are responsible for bone resorption. In this way,
the bone releases some of its calcium, and phosphate, stores into the
bloodstream.
·
At the kidney PTH as two actions. One is to
increase the hydroxylation and activation of vitamin D in the proximal
convoluted tubules. Another in to increase calcium reabsorption from the distal
convoluted tubules and increase phosphate excretion.
Active vitamin D has a similar
action to PTH, however, it is a steroid hormone. One of its unique actions is
to increase dietary calcium absorption from the intestine by increasing
expression of calcium-binding hormone.
Regulation
While PTH is very important in
maintaining adequate levels of calcium in the bloodstream, it is equally as
important that its actions don't cause hypercalcaemia. Regulation is therefore
vital. This is achieved through a negative feedback loop:
·
calcium levels in the blood fall, which is detected by the
parathyroid gland
·
chief cells secrete PTH into the blood
·
calcium is released from bone and reabsorbed from the renal
tubules, causing its level to rise
·
increased calcium levels are detected by the parathyroid gland,
which decreases PTH secretion
Clinical relevance
Primary hyperparathyroidism is a
condition in which the parathyroid gland is overactive. This is often due to
hyperplasia, an adenoma or malignancy. Symptoms of hypercalcaemia develop,
which includes renal calculi, constipation, polyuria, abdominal pain and low
mood. One treatment is surgical removal of the glands.
PTHrp is a
polypeptide which has a similar structure to PTH, hence its name 'related
peptide'. It can be secreted from cancer cells, notably squamous cell bronchial
carcinoma, to cause hypercalcaemia. PTHrp has all the same effects as PTH,
however it cannot activate vitamin D.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:02
Stress response: Endocrine and metabolic changes
·
Surgery precipitates hormonal and metabolic changes causing the
stress response.
·
Stress response is associated with: substrate mobilization,
muscle protein loss, sodium and water retention, suppression of anabolic hormone
secretion, activation of the sympathetic nervous system, immunological and
haematological changes.
·
The hypothalamic-pituitary axis and the sympathetic nervous
systems are activated and there is a failure of the normal feedback mechanisms
of control of hormone secretion.
A summary of the hormonal changes
associated with the stress response:
|
Increased |
Decreased |
No Change |
|
Growth hormone |
Insulin |
Thyroid stimulating hormone |
|
Cortisol |
Testosterone |
Luteinizing hormone |
|
Renin |
Oestrogen |
Follicle stimulating hormone |
|
Adrenocorticotrophic hormone (ACTH) |
|
|
|
Aldosterone |
|
|
|
Prolactin |
|
|
|
Antidiuretic hormone |
|
|
|
Glucagon |
|
|
Sympathetic nervous system
·
Stimulates catecholamine release
·
Causes tachycardia and hypertension
Pituitary gland
·
ACTH and growth hormone (GH) is stimulated by hypothalamic
releasing factors, corticotrophin releasing factor (CRF) and somatotrophin (or
growth hormone releasing factor)
·
Perioperative increased prolactin secretion occurs by release of
inhibitory control
·
Secretion of thyroid stimulating hormone (TSH), luteinizing
hormone (LH) and follicle stimulating hormone (FSH) does not change
significantly
·
ACTH stimulates cortisol production within a few minutes of the
start of surgery. More ACTH is produced than needed to produce a maximum
adrenocortical response.
Cortisol
·
Significant increases within 4-6 hours of surgery (>1000 nmol
litre-1).
·
The usual negative feedback mechanism fails and concentrations
of ACTH and cortisol remain persistently increased.
·
The magnitude and duration of the increase correlate with the
severity of stress and the response is not abolished by the administration of
corticosteroids.
·
The metabolic effects of cortisol are enhanced:
Skeletal muscle protein breakdown
to provide gluconeogenic precursors and amino acids for protein synthesis in
the liver
Stimulation of lipolysis
'Anti-insulin effect'
Mineralocorticoid effects
Anti-inflammatory effects
Growth hormone
·
Increased secretion after surgery has a minor role
·
Most important for preventing muscle protein breakdown and
promote tissue repair by insulin growth factors
Alpha Endorphin
·
Increased
Antidiuretic hormone
·
An important vasopressor and enhances haemostasis
·
Renin is released causing the conversion of angiotensinogen to
angiotensin I
·
Angiotensin II formed by ACE on angiotensin 1, which causes the
secretion of aldosterone from the adrenal cortex. This increases sodium
reabsorption at the distal convoluted tubule
Insulin
·
Release inhibited by stress
·
Occurs via the inhibition of the beta cells in the pancreas by
the α2-adrenergic inhibitory effects of catecholamines
·
Insulin resistance by target cells occurs later
·
The perioperative period is characterized by a state of
functional insulin deficiency
Thyroxine (T4) and
tri-iodothyronine (T3)
·
Circulating concentrations are inversely correlated with
sympathetic activity and after surgery there is a reduction in thyroid hormone
production, which normalises over a few days.
Metabolic effect of endocrine
response
Carbohydrate metabolism
·
Hyperglycaemia is a main feature of the metabolic response to
surgery
·
Due to increase in glucose production and a reduction in glucose
utilization
·
Catecholamines and cortisol promote glycogenolysis and
gluconeogenesis
·
Initial failure of insulin secretion followed by insulin
resistance affects the normal responses
·
The proportion of the hyperglycaemic response reflects the
severity of surgery
·
Hyperglycaemia impairs wound healing and increase infection
rates
Protein metabolism
·
Initially there is inhibition of protein anabolism, followed
later, if the stress response is severe, by enhanced catabolism
·
The amount of protein degradation is influenced by the type of
surgery and also by the nutritional status of the patient
·
Mainly skeletal muscle protein is affected
·
The amino acids released form acute phase proteins (fibrinogen,
C reactive protein, complement proteins, a2-macroglobulin, amyloid A and
ceruloplasmin) and are used for gluconeogenesis
·
Nutritional support has little effect on preventing catabolism
Lipid metabolism
Increased catecholamine, cortisol
and glucagon secretion, and insulin deficiency, promotes lipolysis and ketone
body production.
Salt and water metabolism
·
ADH causes water retention, concentrated urine, and potassium
loss and may continue for 3 to 5 days after surgery
·
Renin causes sodium and water retention
Cytokines
·
Glycoproteins
·
Interleukins (IL) 1 to 17, interferons, and tumour necrosis
factor
·
Synthesized by activated macrophages, fibroblasts, endothelial
and glial cells in response to tissue injury from surgery or trauma
·
IL-6 main cytokine associated with surgery. Peak 12 to 24 h
after surgery and increase by the degree of tissue damage Other effects of
cytokines include fever, granulocytosis, haemostasis, tissue damage limitation
and promotion of healing.
Modifying the response
·
Opioids suppress hypothalamic and pituitary hormone secretion
·
At high doses the hormonal response to pelvic and abdominal
surgery is abolished. However, such doses prolong recovery and increase the
need for postoperative ventilatory support
·
Spinal anaesthesia can reduce the glucose, ACTH, cortisol, GH
and epinephrine changes, although cytokine responses are unaltered
·
Cytokine release is reduced in less invasive surgery
·
Nutrition prevents the adverse effects of the stress response.
Enteral feeding improves recovery
·
Growth hormone and anabolic steroids may improve outcome
·
Normothermia decreases the metabolic response
References
Deborah Burton, Grainne Nicholson,
and George Hall
Endocrine and metabolic response to
surgery .
Contin Educ Anaesth Crit Care Pain
(2004) 4(5): 144-147 doi:10.1093/bjaceaccp/mkh040
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:02
Subclinical hyperthyroidism
Subclinical hyperthyroidism is an
entity which is gaining increasing recognition. It is defined as:
·
normal serum free thyroxine and triiodothyronine levels
·
with a thyroid stimulating hormone (TSH) below normal range
(usually < 0.1 mu/l)
Causes
·
multinodular goitre, particularly in elderly females
·
excessive thyroxine may give a similar biochemical picture
The importance in recognising
subclinical hyperthyroidism lies in the potential effect on the cardiovascular
system (atrial fibrillation) and bone metabolism (osteoporosis). It may also
impact on quality of life and increase the likelihood of dementia
Management
·
TSH levels often revert to normal - therefore levels must be
persistently low to warrant intervention
·
a reasonable treatment option is a therapeutic trial of low-dose
antithyroid agents for approximately 6 months in an effort to induce a
remission
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:02
Sulfonylureas: side-effects
Common adverse effects
·
hypoglycaemic episodes (more common with long acting
preparations such as chlorpropamide)
·
weight gain
Rarer adverse effects
·
syndrome of inappropriate ADH secretion
·
bone marrow suppression
·
liver damage (cholestatic)
·
peripheral neuropathy
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:02
Thyrotoxicosis: causes and investigation
Graves' disease accounts for around
50-60% of cases of thyrotoxicosis.
Causes
·
Graves' disease
·
toxic nodular goitre
·
acute phase of subacute (de Quervain's) thyroiditis
·
acute phase of post-partum thyroiditis
·
acute phase of Hashimoto's thyroiditis (later results in
hypothyroidism)
·
amiodarone therapy
Investigation
·
TSH down, T4 and T3 up
·
thyroid autoantibodies
·
other investigations are not routinely done but includes isotope
scanning
|
|
|
|
|
|
Venn diagram showing how different causes of thyroid
dysfunction may manifest. Note how many causes of hypothyroidism may have an
initial thyrotoxic phase.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:02
Thyrotoxicosis: features
General
·
Weight loss
·
'Manic', restlessness
·
Heat intolerance
Cardiac
·
palpitations, tachycardia
·
high-output cardiac failure may occur in elderly patients, a reversible cardiomyopathy can rarely develop
Skin
·
Increased sweating
·
Pretibial myxoedema: erythematous, oedematous lesions above the
lateral malleoli
·
Thyroid acropachy: clubbing
Gastrointestinal
·
Diarrhoea
Gynaecological
·
Oligomenorrhea
Neurological
·
Anxiety
·
Tremor
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
20:56
Diabetes mellitus: management of type 2
NICE updated its guidance on the
management of type 2 diabetes mellitus (T2DM) in 2015. Key points are listed
below:
·
HbA1c targets have changed. They are now dependent on what
antidiabetic drugs a patient is receiving and other factors such as frailty
·
there is more flexibility in the second stage of treating
patients (i.e. after metformin has been started) - you now have a choice of 4
oral antidiabetic agents
It's worthwhile thinking of the
average patient who is taking metformin for T2DM, you can titrate up metformin
and encourage lifestyle changes to aim for a HbA1c of 48 mmol/mol (6.5%), but should only add a second drug if the HbA1c rises to 58 mmol/mol (7.5%)
Dietary advice
·
encourage high fibre, low glycaemic index sources of
carbohydrates
·
include low-fat dairy products and oily fish
·
control the intake of foods containing saturated fats and trans
fatty acids
·
limited substitution of sucrose-containing foods for other
carbohydrates is allowable, but care should be taken to avoid excess energy intake
·
discourage use of foods marketed specifically at people with
diabetes
·
initial target weight loss in an overweight person is 5-10%
HbA1c targets
This is area which has changed in
2015
·
individual targets should be agreed with patients to encourage
motivation
·
HbA1c should be checked every 3-6 months until stable, then 6
monthly
·
NICE encourage us to consider relaxing targets on 'a case-by-case basis, with particular consideration for people
who are older or frail, for adults with type 2 diabetes'
·
in 2015 the guidelines changed so HbA1c targets are now
dependent on treatment:
Lifestyle or single drug treatment
|
Management
of T2DM |
HbA1c target |
|
Lifestyle |
48 mmol/mol (6.5%) |
|
Lifestyle + metformin |
48 mmol/mol (6.5%) |
|
Includes any drug which may cause
hypoglycaemia (e.g. lifestyle + sulfonylurea) |
53 mmol/mol (7.0%) |
Practical examples
·
a patient is newly diagnosed with HbA1c and wants to try
lifestyle treatment first. You agree a target of 48 mmol/mol (6.5%)
·
you review a patient 6 months after starting metformin. His
HbA1c is 51 mmol/mol (6.8%). You increase his metformin from 500mg bd to 500mg
tds and reinforce lifestyle factors
Patient already on treatment
|
Management
of T2DM |
HbA1c target |
|
Already on one drug, but HbA1c has
risen to 58 mmol/mol (7.5%) |
53 mmol/mol (7.0%) |
Drug treatment
The 2015 NICE guidelines introduced
some changes into the management of type 2 diabetes. There are essentially two
pathways, one for patients who can tolerate metformin, and one for those who
can't:
|
|
|
|
|
|
Tolerates metformin:
·
metformin is still first-line and should be offered if the HbA1c
rises to 48 mmol/mol (6.5%)* on lifestyle interventions
·
if the HbA1c has risen to 58 mmol/mol (7.5%) then a second drug
should be added from the following list:
o sulfonylurea
o gliptin
o pioglitazone
o SGLT-2 inhibitor
·
if despite this the HbA1c rises to, or remains above 58 mmol/mol (7.5%) then
triple therapy with one of the following combinations should be offered:
o metformin + gliptin + sulfonylurea
o metformin + pioglitazone +
sulfonylurea
o metformin + sulfonylurea + SGLT-2
inhibitor
o metformin + pioglitazone + SGLT-2
inhibitor
o OR insulin therapy should be
considered
Criteria for glucagon-like peptide1
(GLP1) mimetic (e.g. exenatide)
·
if triple therapy is not effective, not tolerated or
contraindicated then NICE advise that we consider combination therapy with
metformin, a sulfonylurea and a glucagonlike peptide1 (GLP1) mimetic if:
o BMI >= 35 kg/m² and specific
psychological or other medical problems associated with obesity or
o BMI < 35 kg/m² and for whom
insulin therapy would have significant occupational implications or
weight loss would benefit other
significant obesity related comorbidities
·
only continue if there is a reduction of at least 11 mmol/mol
[1.0%] in HbA1c and a weight loss of at least 3% of initial body weight in 6
months
Practical examples
·
you review an established type 2 diabetic on maximum dose
metformin. Her HbA1c is 55 mmol/mol (7.2%). You do not add another drug as she
has not reached the threshold of 58 mmol/mol (7.5%)
·
a type 2 diabetic is found to have a HbA1c of 62 mmol/mol (7.8%)
at annual review. They are currently on maximum dose metformin. You elect to
add a sulfonylurea
Cannot tolerate metformin or
contraindicated
·
if the HbA1c rises to 48 mmol/mol (6.5%)* on lifestyle
interventions, consider one of the following:
o sulfonylurea
o gliptin
o pioglitazone
·
if the HbA1c has risen to 58 mmol/mol (7.5%) then a one of the
following combinations should be used:
o gliptin + pioglitazone
o gliptin + sulfonylurea
o pioglitazone + sulfonylurea
·
if despite this the HbA1c rises to, or remains above 58 mmol/mol
(7.5%) then consider insulin therapy
Starting insulin
·
metformin should be continued. In terms of other drugs NICE
advice: 'Review the continued need for
other blood glucose lowering therapies'
·
NICE recommend starting with human NPH insulin (isophane,
intermediate acting) taken at bed-time or twice daily according to need
Risk factor modification
Hypertension
·
blood pressure targets are the same as for
patients without type 2 diabetes (see table below)
·
ACE inhibitors are first-line
|
|
Clinic BP |
ABPM / HBPM |
|
Age < 80 years |
140/90 mmHg |
135/85 mmHg |
|
Age > 80 years |
150/90 mmHg |
145/85 mmHg |
Antiplatelets
·
should not be offered unless a patient has existing
cardiovascular disease
Lipids
·
following the 2014 NICE lipid modification guidelines only
patients with a 10-year cardiovascular risk > 10% (using QRISK2) should be
offered a statin. The first-line statin of choice is atorvastatin 20mg on
|
|
|
|
|
|

Graphic showing choice of statin.
*this is a bit confusing because
isn't the diagnostic criteria for T2DM HbA1c 48 mmol/mol (6.5%)? So shouldn't
all patients be offered metformin at diagnosis? Our interpretation of this is
that some patients upon diagnosis will elect to try lifestyle measures, which
may reduce their HbA1c below this level. If it then rises to the diagnostic
threshold again metformin should be offered
From <https://www.passmedicine.com/question/questions.php?q=0#>
21 December 2020
21:48
Diabetic ketoacidosis
Diabetic ketoacidosis (DKA) may be
a complication existing type 1 diabetes mellitus or be the first presentation,
accounting for around 6% of cases. Rarely, under conditions of extreme stress,
patients with type
2 diabetes mellitus may also develop DKA.
Whilst DKA remains a serious
condition mortality rates have decreased from 8% to under 1% in the past 20
years.
Pathophysiology
·
DKA is caused by uncontrolled lipolysis (not proteolysis) which
results in an excess of free fatty acids that are ultimately converted to
ketone bodies
The most common precipitating
factors of DKA are infection, missed insulin doses and myocardial infarction.
Features
·
abdominal pain
·
polyuria, polydipsia, dehydration
·
Kussmaul respiration (deep hyperventilation)
·
Acetone-smelling breath ('pear drops' smell)
Diagnostic criteria
|
American
Diabetes Association (2009) |
Joint British Diabetes Societies (2013) |
|
Key points ·
glucose > 13.8 mmol/l ·
pH < 7.30 ·
serum bicarbonate <18 mmol/l ·
anion gap > 10 ·
ketonaemia |
Key points ·
glucose > 11 mmol/l or known diabetes mellitus ·
pH < 7.3 ·
bicarbonate < 15 mmol/l ·
ketones > 3 mmol/l or
urine ketones ++ on dipstick |
Management
·
fluid replacement: most patients with DKA are deplete around 5-8
litres. Isotonic saline is used initially. Please see an example fluid regime
below.
·
insulin: an intravenous infusion should be started at 0.1
unit/kg/hour. Once blood glucose is < 15 mmol/l an infusion of 5% dextrose
should be started
·
correction of hypokalaemia
·
long-acting insulin should be continued,
short-acting insulin should be stopped
JBDS example of fluid replacement
regime for patient with a systolic BP on admission 90mmHg and over
|
Fluid |
Volume |
|
0.9% sodium chloride 1L |
1000ml over 1st hour |
|
0.9% sodium chloride 1L with potassium
chloride |
1000ml over next 2 hours |
|
0.9% sodium chloride 1L with potassium
chloride |
1000ml over next 2 hours |
|
0.9% sodium chloride 1L with potassium
chloride |
1000ml over next 4 hours |
|
0.9% sodium chloride 1L with potassium
chloride |
1000ml over next 4 hours |
|
0.9% sodium chloride 1L with potassium
chloride |
1000ml over next 6 hours |
Please note that slower infusion
may be indicated in young adults (aged 18-25 years) as they are at greater risk
of cerebral oedema.
JBDS potassium guidelines
|
Potassium
level in first 24 hours (mmol/L) |
Potassium replacement in mmol/L of
infusion solution |
|
Over 5.5 |
Nil |
|
3.5-5.5 |
40 |
|
Below 3.5 |
Senior review as additional potassium
needs to be given |
Complications of DKA and its
treatment
·
gastric stasis
·
thromboembolism
·
arrhythmias secondary to hyperkalaemia/iatrogenic hypokalaemia
·
iatrogenic due to incorrect fluid therapy: cerebral oedema*, hypokalaemia, hypoglycaemia
·
acute respiratory distress syndrome
·
acute kidney injury
* children/young adults
are particularly vulnerable to cerebral oedema following
fluid resuscitation in DKA and often need 1:1 nursing to monitor
neuro-observations, headache, irritability, visual disturbance, focal neurology
etc. It usually occurs 4-12 hours following commencement of treatment but can
present at any time. If there is any suspicion a CT head and senior review
should be sought
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
16:16
Diabetes mellitus (type 2): diagnosis
The diagnosis of type 2 diabetes
mellitus can be made by either a plasma glucose or a HbA1c sample. Diagnostic
criteria vary according to whether the patient is symptomatic (polyuria,
polydipsia etc) or not.
If the patient is symptomatic:
·
fasting glucose greater than or equal to 7.0
mmol/l
·
random glucose greater than or equal to 11.1
mmol/l (or after 75g
oral glucose tolerance test)
If the patient is asymptomatic the
above criteria apply but must be demonstrated on two separate occasions.
|
|
|
|
|
|
Diagram showing the spectrum of diabetes diagnosis
In 2011 WHO released supplementary
guidance on the use of HbA1c on the diagnosis of diabetes:
·
a HbA1c of greater than or equal to 48
mmol/mol (6.5%) is
diagnostic of diabetes mellitus
·
a HbAlc value of less than 48 mmol/mol (6.5%) does not exclude
diabetes (i.e. it is not as sensitive as fasting samples for detecting
diabetes)
·
in patients without symptoms, the test must be repeated to
confirm the diagnosis
·
it should be remembered that misleading HbA1c results can be
caused by increased red cell turnover (see below)
Conditions where HbA1c may not be used for
diagnosis:
·
haemoglobinopathies
·
haemolytic anaemia
·
untreated iron deficiency anaemia
·
suspected gestational diabetes
·
children
·
HIV
·
chronic kidney disease
·
people taking medication that may cause hyperglycaemia (for
example corticosteroids)
Impaired fasting glucose and
impaired glucose tolerance
A fasting glucose greater than or
equal to 6.1 but less than 7.0 mmol/l implies impaired fasting glucose (IFG)
Impaired glucose tolerance (IGT) is
defined as fasting plasma glucose less than 7.0 mmol/l and OGTT 2-hour value
greater than or equal to 7.8 mmol/l but less than 11.1 mmol/l
Diabetes UK suggests:
·
'People with IFG should then be offered an oral glucose
tolerance test to rule out a diagnosis of diabetes. A result below 11.1 mmol/l
but above 7.8 mmol/l indicates that the person doesn't have diabetes but does
have IGT.'
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:48
Addisonian crisis
Causes
·
sepsis or surgery causing an acute exacerbation of chronic
insufficiency (Addison's, Hypopituitarism)
·
adrenal haemorrhage eg Waterhouse-Friderichsen syndrome
(fulminant meningococcemia)
·
steroid withdrawal
Management
·
hydrocortisone 100 mg im or iv
·
1 litre normal saline infused over 30-60 mins or with dextrose
if hypoglycaemic
·
continue hydrocortisone 6 hourly until the patient is stable. No
fludrocortisone is required because high cortisol exerts weak mineralocorticoid
action
·
oral replacement may begin after 24 hours and be reduced to
maintenance over 3-4 days
From <https://www.passmedicine.com/review/textbook.php?s=#>
Features
of an addisonian crisis:
·
Hyponatraemia
·
Hyperkalaemia
·
Hypoglycaemia
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
19:10
Corticosteroids
Corticosteroids are amongst the
most commonly prescribed therapies in clinical practice. They are used both
systemically (oral or intravenous) or locally (skin creams, inhalers, eye
drops, intra-articular). They augment and in some cases replace the natural
glucocorticoid and mineralocorticoid activity of endogenous steroids.
The relative glucocorticoid and
mineralocorticoid activity of commonly used steroids is shown below:
|
Minimal
glucocorticoid activity, very high mineralocorticoid activity, |
Glucocorticoid activity, high
mineralocorticoid activity, |
Predominant glucocorticoid activity,
low mineralocorticoid activity |
Very high glucocorticoid activity,
minimal mineralocorticoid activity |
|
Fludrocortisone |
Hydrocortisone |
Prednisolone |
Dexamethasone Betmethasone |
Side-effects
The side-effects of corticosteroids
are numerous and represent the single greatest limitation on their usage.
Side-effects are more common with systemic and prolonged therapy.
Glucocorticoid side-effects
·
endocrine: impaired glucose regulation, increased
appetite/weight gain, hirsutism, hyperlipidaemia
·
Cushing's syndrome: moon face, buffalo hump, striae
·
musculoskeletal: osteoporosis, proximal
myopathy, avascular necrosis of the femoral head
·
immunosuppression: increased susceptibility
to severe infection, reactivation of tuberculosis
·
psychiatric: insomnia, mania, depression, psychosis
·
gastrointestinal: peptic ulceration, acute
pancreatitis
·
ophthalmic: glaucoma, cataracts
·
suppression of growth in children
·
intracranial hypertension
·
neutrophilia
Mineralocorticoid side-effects
·
fluid retention
·
hypertension
Selected points on the use of corticosteroids:
·
patients on long-term steroids should have their doses doubled
during intercurrent illness
·
the BNF suggests gradual withdrawal of systemic corticosteroids
if patients have: received more than 40mg prednisolone daily for more than one
week, received more than 3 weeks treatment or recently received repeated
courses
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
20:51
Phaeochromocytoma
Pheochromocytoma
Phaeochromocytoma is a rare
catecholamine secreting tumour. About 10% are familial and may be associated
with MEN type II, neurofibromatosis and von Hippel-Lindau syndrome
Basics
·
bilateral in 10%
·
malignant in 10%
·
extra-adrenal in 10% (most common site = organ of Zuckerkandl,
adjacent to the bifurcation of the aorta)
Features are typically
episodic
·
hypertension (around 90% of cases, may be sustained)
·
headaches
·
palpitations
·
sweating
·
anxiety
Tests
·
24 hr urinary collection of metanephrines (sensitivity
97%*)
·
this has replaced a 24 hr urinary collection of catecholamines (sensitivity 86%)
Surgery is the definitive
management. The patient must first however be stabilized with medical
management:
·
alpha-blocker (e.g. phenoxybenzamine), given before a
·
beta-blocker (e.g. propranolol)
*BMJ 2012; 344 doi: http://dx.doi.org/10.1136/bmj.e1042
(Published 20 February 2012
Labetalol
has both alpha and beta action
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
18:01
Thyroid cancer
Features of hyperthyroidism or
hypothyroidism are not commonly seen in patients with thyroid malignancies as
they rarely secrete thyroid hormones
Main points
|
Type |
Percentage |
|
|
Papillary |
70% |
Often young females - excellent
prognosis |
|
Follicular |
20% |
|
|
Medullary |
5% |
Cancer of parafollicular (C) cells,
secrete calcitonin, part of MEN-2 |
|
Anaplastic |
1% |
Not responsive to treatment, can cause
pressure symptoms |
|
Lymphoma |
Rare |
Associated with Hashimoto's
thyroiditis |
Management of papillary and
follicular cancer
·
total thyroidectomy
·
followed by radioiodine (I-131) to kill residual cells
·
yearly thyroglobulin levels to detect early recurrent disease
Further information
|
Type |
Notes |
|
Papillary carcinoma |
·
Usually contain a mixture of papillary and
colloidal filled follicles ·
Histologically tumour has papillary projections and
pale empty nuclei ·
Seldom encapsulated ·
Lymph node metastasis predominate ·
Haematogenous metastasis rare |
|
Follicular adenoma |
·
Usually present as a solitary thyroid nodule ·
Malignancy can only be excluded on formal
histological assessment |
|
Follicular carcinoma |
·
May appear macroscopically encapsulated,
microscopically capsular invasion is seen. Without this finding the lesion is
a follicular adenoma. ·
Vascular invasion predominates ·
Multifocal disease raree |
|
Medullary carcinoma |
·
C cells derived from neural crest and not thyroid
tissue ·
Serum calcitonin levels often raised ·
Familial genetic disease accounts for up to 20%
cases ·
Both lymphatic and haematogenous metastasis are
recognised, nodal disease is associated with a very poor prognosis. |
|
Anaplastic carcinoma |
·
Most common in elderly females ·
Local invasion is a common feature ·
Treatment is by resection where possible,
palliation may be achieved through isthmusectomy and radiotherapy.
Chemotherapy is ineffective. |
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:48
Diabetes mellitus: management of type 1
The long-term management of type 1
diabetics is an important and complex process requiring the input of many
different clinical specialties and members of the healthcare team. A diagnosis of
type 1 diabetes can still reduce the life expectancy of patients by 13 years
and the micro and macrovascular complications are well documented.
NICE released guidelines on the
diagnosis and management of type 1 diabetes in 2015. We've only highlighted a
very select amount of the guidance here which will be useful for any clinician
looking after a patient with type 1 diabetes.
HbA1c
·
should be monitored every 3-6 months
·
adults should have a target of HbA1c level of 48 mmol/mol (6.5%)
or lower. NICE do however recommend taking into account factors such as the
person's daily activities, aspirations, likelihood of complications,
comorbidities, occupation and history of hypoglycaemia
Self-monitoring of blood glucose
·
recommend testing at least 4 times a day, including before each
meal and before bed
·
more frequent monitoring is recommended if frequency of
hypoglycaemic episodes increases; during periods of illness; before, during and
after sport; when planning pregnancy, during pregnancy and while breastfeeding
Blood glucose targets
·
5-7 mmol/l on waking and
·
4-7 mmol/l before meals at other times of the day
Type of insulin
·
offer multiple daily injection basal–bolus insulin regimens,
rather than twice‑daily mixed insulin regimens, as the insulin injection
regimen of choice for all adults
·
twice‑daily insulin detemir is the regime of choice. Once-daily
insulin glargine or insulin detemir is an alternative
·
offer rapid‑acting insulin analogues injected before meals,
rather than rapid‑acting soluble human or animal insulins, for mealtime insulin
replacement for adults with type 1 diabetes
Metformin
·
NICE recommend considering adding metformin if the BMI >= 25
kg/m²
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
19:45
Diabetes mellitus: GLP-1 drugs
A number of drugs to treat diabetes
mellitus have become available in recent years. Much research has focused
around the role of glucagon-like peptide-1 (GLP-1), a hormone released by the
small intestine in response to an oral glucose load
Whilst it is well known that
insulin resistance and insufficient B-cell compensation occur other effects are
also seen in type 2 diabetes mellitus (T2DM). In normal physiology an oral
glucose load results in a greater release of insulin than if the same load is given
intravenously - this known as the incretin effect. This effect is largely
mediated by GLP-1 and is known to be decreased in T2DM.
Increasing GLP-1 levels, either by
the administration of an analogue (glucagon-like peptide-1, GLP-1 mimetics,
e.g. exenatide) or inhibiting its breakdown (dipeptidyl peptidase-4 ,DPP-4
inhibitors - the gliptins), is therefore the target of two recent classes of
drug.
Glucagon-like peptide-1 (GLP-1)
mimetics (e.g. exenatide)
Exenatide is an example of a glucagon-like peptide-1 (GLP-1)
mimetic. These drugs increase insulin secretion and inhibit
glucagon secretion. One of the major advances of GLP-1 mimetics is that they
typically result in weight loss, in contrast to many medications such as
insulin, sulfonylureas and thiazolidinediones. They are sometimes used in combination with insulin
in T2DM to minimise weight gain.
Exenatide must be given by
subcutaneous injection within 60 minutes before the morning and evening meals.
It should not be given after a meal.
Liraglutide is the other GLP-1
mimetic currently available. One the main advantages of liraglutide over
exenatide is that it only needs to be given once a day.
Both exenatide and liraglutide may
be combined with metformin and a sulfonylurea. Standard release exenatide is
also licensed to be used with basal insulin alone or with metformin. Please see
the BNF for a more complete list of licensed indications.
NICE state the following:
Consider adding exenatide to metformin and a
sulfonylurea if:
·
BMI >= 35 kg/m² in people of European descent and there are
problems associated with high weight, or
·
BMI < 35 kg/m² and insulin is unacceptable because of
occupational implications or weight loss would benefit other comorbidities.
NICE like patients to have achieved
a > 11 mmol/mol (1%) reduction in HbA1c and 3% weight loss after 6 months to
justify the ongoing prescription of GLP-1 mimetics.
The major adverse effect of GLP-1
mimetics is nausea
and vomiting. The Medicines and Healthcare products Regulatory
Agency has issued specific warnings on the use of exenatide, reporting that is
has been linked to severe
pancreatitis in some patients.
Dipeptidyl peptidase-4 (DPP-4)
inhibitors (e.g. Vildagliptin, sitagliptin)
Key points
·
DPP-4 inhibitors increase levels of incretins
(GLP-1 and GIP)
·
oral preparation
·
trials to date show that the drugs are relatively well tolerated
with no increased incidence of hypoglycaemia
·
do not cause weight gain
NICE guidelines on DPP-4 inhibitors
·
NICE suggest that a DPP-4 inhibitor might be preferable to a
thiazolidinedione if further weight gain would cause significant problems, a
thiazolidinedione is contraindicated or the person has had a poor response to a
thiazolidinedione
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
19:14
Glycosylated haemoglobin
Glycosylated haemoglobin (HbA1c) is
the most widely used measure of long-term glycaemic control in diabetes
mellitus. HbA1c is produced by the glycosylation of haemoglobin at a rate
proportional to the glucose concentration. The level of HbA1c therefore is
dependant on
·
red blood cell lifespan
·
average blood glucose concentration
A number of conditions can
interfere with accurate HbA1c interpretation:
|
Lower-than-expected
levels of HbA1c (due
to reduced red blood cell lifespan) |
Higher-than-expected levels of HbA1c (due to increased red blood cell lifespan) |
|
Sickle-cell anaemia GP6D deficiency Hereditary
spherocytosis |
Vitamin B12/folic acid deficiency Iron-deficiency anaemia Splenectomy |
HbA1c is generally thought to
reflect the blood glucose over the previous '3 months' although there is some
evidence it is weighed more strongly to glucose levels of the past 2-4 weeks.
NICE recommend 'HbA1c
should be checked every 3-6 months until stable, then 6 monthly'.
The relationship between HbA1c and
average blood glucose is complex but has been studied by the Diabetes Control
and Complications Trial (DCCT). A new internationally standardised method for
reporting HbA1c has been developed by the International Federation of Clinical
Chemistry (IFCC). This will report HbA1c in mmol per mol of haemoglobin without
glucose attached.
|
HBA1c (%) |
Average plasma glucose (mmol/l) |
IFCC-HbA1c (mmol/mol) |
|
5 |
5.5 |
|
|
6 |
7.5 |
42 |
|
7 |
9.5 |
53 |
|
8 |
11.5 |
64 |
|
9 |
13.5 |
75 |
|
10 |
15.5 |
|
|
11 |
17.5 |
|
|
12 |
19.5 |
|
From the above we can see that
average plasma glucose = (2 * HbA1c) - 4.5
Next question
Save my notes
Search
Go
Google search on
"Glycosylated haemoglobin"
Links
|
DocStoc |
20 |
|
|
Suggest linkReport broken link
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:48
Gynaecomastia
Gynaecomastia describes an abnormal
amount of breast tissue in males and is usually caused by an increased
oestrogen:androgen ratio. It is important to differentiate the causes of
galactorrhoea (due to the actions of prolactin on breast tissue) from those of
gynaecomastia
Causes of gynaecomastia
·
physiological: normal in puberty
·
syndromes with androgen deficiency: Kallman's, Klinefelter's
·
testicular failure: e.g. mumps
·
liver disease
·
testicular cancer e.g. seminoma secreting hCG
·
ectopic tumour secretion
·
hyperthyroidism
·
haemodialysis
·
drugs: see below
Drug causes of gynaecomastia
·
spironolactone (most common drug cause)
·
cimetidine
·
digoxin
·
cannabis
·
finasteride
·
GnRH agonists e.g. goserelin, buserelin
·
oestrogens, anabolic steroids
Very rare drug causes of gynaecomastia
·
tricyclics
·
isoniazid
·
calcium channel blockers
·
heroin
·
busulfan
·
methyldopa
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
20:23
Hypothyroidism: management
Key points
·
initial starting dose of levothyroxine should be lower in
elderly patients and those with ischaemic heart disease. The BNF recommends
that for patients with cardiac disease, severe hypothyroidism or patients over
50 years the initial starting dose should be 25mcg od with dose slowly
titrated. Other patients should be started on a dose of 50-100mcg od
·
following a change in thyroxine dose thyroid function tests
should be checked after 8-12 weeks
·
the therapeutic goal is 'normalisation' of the thyroid
stimulating hormone (TSH) level. As the majority of unaffected people have a
TSH value 0.5-2.5 mU/l it is now thought preferable to aim for a TSH in this
range
·
women with established hypothyroidism who become pregnant should
have their dose increased 'by at least 25-50 micrograms levothyroxine'* due to
the increased demands of pregnancy. The TSH should be monitored carefully,
aiming for a low-normal value
·
there is no evidence to support combination therapy with
levothyroxine and liothyronine
Side-effects of thyroxine therapy
·
hyperthyroidism: due to over treatment
·
reduced bone mineral density
·
worsening of angina
·
atrial fibrillation
Interactions
·
iron, calcium carbonate
o absorption of levothyroxine
reduced, give at least 4 hours apart
*source: NICE Clinical Knowledge
Summaries
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
19:12
Multiple endocrine neoplasia
The table below summarises the
three main types of multiple endocrine neoplasia (MEN). MEN is inherited as an
autosomal dominant disorder.
Men-2 Men-1
|
MEN
type I |
MEN type IIa |
MEN type IIb |
|
3 P's Parathyroid
(95%): hyperparathyroidism due to parathyroid hyperplasia Pituitary
(70%) Pancreas
(50%): e.g. insulinoma, gastrinoma (leading to recurrent peptic ulceration) Also: adrenal and thyroid |
Medullary thyroid cancer (70%) 2 P's Parathyroid
(60%) Phaeochromocytoma |
Medullary thyroid cancer 1 P Phaeochromocytoma Marfanoid body habitus Neuromas |
|
MEN1 gene Most common presentation =
hypercalcaemia |
RET oncogene |
RET oncogene |
|
|
|
|
|
|

Venn diagram showing the different types of MEN and
their associated features
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:48
Thiazolidinediones
Thiazolidinediones are a class of
agents used in the treatment of type 2 diabetes mellitus. They are agonists to the PPAR-gamma
receptor and reduce peripheral insulin resistance.
Rosiglitazone was withdrawn in 2010 following concerns about the cardiovascular
side-effect profile.
The PPAR-gamma receptor is an
intracellular nuclear receptor. It's natural ligands are free fatty acids and
it is thought to control adipocyte differentiation and function.
Adverse effects
·
weight gain
·
liver impairment: monitor LFTs
·
fluid retention - therefore contraindicated in heart failure. The risk of fluid retention is
increased if the patient also takes insulin
·
recent studies have indicated an increased risk of fractures
·
bladder cancer: recent studies have shown an increased risk of bladder
cancer in patients taking pioglitazone (hazard ratio 2.64)
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
19:53

Tuesday, 22 December 2020
23:33
Hashimoto's thyroiditis
Hashimoto's thyroiditis (chronic
autoimmune thyroiditis) is an autoimmune disorder of the thyroid gland. It is
typically associated with hypothyroidism although there may be a transient
thyrotoxicosis in the acute phase. It is 10 times more common in women
Features
·
features of hypothyroidism
·
goitre: firm, non-tender
·
anti-thyroid peroxidase (TPO) and also anti-thyroglobulin (Tg)
antibodies
Associations
·
other autoimmune conditions e.g. coeliac disease, type
1 diabetes mellitus, vitiligo
·
Hashimoto's thyroiditis is associated with the development
of MALT lymphoma
|
|
|
|
|
|
Venn diagram showing how different causes of thyroid
dysfunction may manifest. Note how many causes of hypothyroidism may have an
initial thyrotoxic phase.
21 December 2020
21:48
Thyroid storm
Thyroid storm is a rare but
life-threatening complication of thyrotoxicosis. It is typically seen in
patients with established thyrotoxicosis and is rarely seen as the presenting
feature. Iatrogenic thyroxine excess does not usually result in thyroid storm.
Precipitating events:
·
thyroid or non-thyroidal surgery
·
trauma
·
infection
·
acute iodine load e.g. CT contrast media
Clinical features include:
·
fever > 38.5ºC
·
tachycardia
·
confusion and agitation
·
nausea and vomiting
·
hypertension
·
heart failure
·
abnormal liver function test - jaundice may be seen clinically
Management:
·
symptomatic treatment e.g. paracetamol
·
treatment of underlying precipitating event
·
beta-blockers: typically IV propranolol
·
anti-thyroid drugs: e.g. methimazole or propylthiouracil
·
Lugol's iodine
·
dexamethasone - e.g. 4mg IV qds - blocks the conversion of T4 to
T3
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
20:52
Insulin therapy: side-effects
Hypoglycaemia
·
patients should be taught the signs of hypoglycaemia: sweating,
anxiety, blurred vision, confusion, aggression
·
conscious patients should take 10-20g of a short-acting
carbohydrate (e.g. a glass of Lucozade or non-diet drink, three or more glucose
tablets, glucose gel)
·
every person treated with insulin should have a glucagon kit for emergencies
where the patient is not able to orally ingest a short-acting carbohydrate
·
patients who have frequent hypoglycaemic episodes may develop
reduced awareness. If this develops then allowing glycaemic control to slip for
a period of time may restore their awareness
·
beta-blockers reduce hypoglycaemic awareness
Lipodystrophy
·
typically presents as atrophy/lumps of
subcutaneous fat
·
can be prevented by rotating the injection site
·
may cause erractic insulin absorption
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
17:06
Graves' disease: features
Graves' disease is the most common
cause of thyrotoxicosis. It is typically seen in women aged 30-50 years.
Features
·
typical features of thyrotoxicosis
·
specific signs limited to Grave's (see below)
Features seen in Graves' but not in
other causes of thyrotoxicosis
·
eye signs (30% of patients)
o exophthalmos
o ophthalmoplegia
·
pretibial myxoedema
·
thyroid acropachy, a triad of:
o digital clubbing
o soft tissue swelling of the hands
and feet
o periosteal new bone formation
Autoantibodies
·
TSH receptor stimulating antibodies (90%)
·
anti-thyroid peroxidase antibodies (75%)
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
17:08
SGLT-2 inhibitors
SGLT-2 inhibitors reversibly inhibit
sodium-glucose co-transporter 2 (SGLT-2) in the renal proximal convoluted
tubule to reduce
glucose reabsorption and increase urinary glucose excretion.
Examples include canagliflozin,
dapagliflozin and empagliflozin.
Important adverse effects include
·
urinary and genital infection (secondary to glycosuria). Fournier’s gangrene has also been reported
·
normoglycaemic ketoacidosis
·
increased risk of lower-limb amputation: feet should be closely
monitored
Patients taking SGLT-2 drugs often lose weight, which can be beneficial in type 2 diabetes mellitus.
From <https://www.passmedicine.com/question/questions.php?q=0>
Wednesday, 23 December 2020
00:27
Myxoedema coma
Myxoedema coma
typically presents with confusion and hypothermia.
Myxoedema coma is a medical
emergency requiring treatment with
·
IV thyroid replacement
·
IV fluid
·
IV corticosteroids (until the possibility of
coexisting adrenal insufficiency has been excluded)
·
electrolyte imbalance correction
·
sometimes rewarming
22 December 2020
19:28
Diabetes mellitus: management of type 1
The long-term management of type 1
diabetics is an important and complex process requiring the input of many
different clinical specialties and members of the healthcare team. A diagnosis
of type 1 diabetes can still reduce the life expectancy of patients by 13 years
and the micro and macrovascular complications are well documented.
NICE released guidelines on the
diagnosis and management of type 1 diabetes in 2015. We've only highlighted a
very select amount of the guidance here which will be useful for any clinician
looking after a patient with type 1 diabetes.
HbA1c
·
should be monitored every 3-6 months
·
adults should have a target of HbA1c level of 48 mmol/mol (6.5%)
or lower. NICE do however recommend taking into account factors such as the
person's daily activities, aspirations, likelihood of complications,
comorbidities, occupation and history of hypoglycaemia
Self-monitoring of blood glucose
·
recommend testing at least 4 times a day, including before each
meal and before bed
·
more frequent monitoring is recommended if frequency of
hypoglycaemic episodes increases; during periods of illness; before, during and
after sport; when planning pregnancy, during pregnancy and while breastfeeding
Blood glucose targets
·
5-7 mmol/l on waking and
·
4-7 mmol/l before meals at other times of the day
Type of insulin
·
offer multiple daily injection basal–bolus insulin regimens,
rather than twice‑daily mixed insulin regimens, as the insulin injection
regimen of choice for all adults
·
twice‑daily insulin detemir is the regime of choice. Once-daily
insulin glargine or insulin detemir is an alternative
·
offer rapid‑acting insulin analogues injected before meals,
rather than rapid‑acting soluble human or animal insulins, for mealtime insulin
replacement for adults with type 1 diabetes
Metformin
·
NICE recommend considering adding metformin if the BMI >= 25
kg/m²
From <https://www.passmedicine.com/question/questions.php?q=0>
31 December 2020
19:58
Levothyroxine not
associated with diabetes
31 December 2020
20:05
Levothyroxine
is not associated with inducing diabetes. In patients with diabetes starting thyroxine,
doses of antidiabetic drugs including insulin may need to be increased.
From <https://www.passmedicine.com/question/questions.php?q=0#>
24 December 2020
14:25
Haematuria
The management of patients with
haematuria is often difficult due to the absence of widely followed guidelines.
It is sometimes unclear whether patients are best managed in primary care, by
urologists or by nephrologists.
The terminology surrounding
haematuria is changing. Microscopic or dipstick positive haematuria is
increasingly termed non-visible haematuria whilst macroscopic haematuria is
termed visible haematuria. Non-visible haematuria is found in around 2.5% of
the population.
Causes of transient or spurious
non-visible haematuria
·
urinary tract infection
·
menstruation
·
vigorous exercise (this normally settles after around 3 days)
·
sexual intercourse
Causes of persistent non-visible
haematuria
·
cancer (bladder, renal, prostate)
·
stones
·
benign prostatic hyperplasia
·
prostatitis
·
urethritis e.g. Chlamydia
·
renal causes: IgA nephropathy, thin basement membrane disease
Spurious causes - red/orange urine,
where blood is not present on dipstick
·
foods: beetroot, rhubarb
·
drugs: rifampicin, doxorubicin
Management
Current evidence does not support
screening for haematuria. The incidence of non-visible haematuria is similar in
patients taking aspirin/warfarin to the general population hence these patients
should also be investigated.
Testing
·
urine dipstick is the test of choice for detecting haematuria
·
persistent non-visible haematuria is often defined as blood
being present in 2 out of 3 samples tested 2-3 weeks apart
·
renal function, albumin:creatinine (ACR) or protein:creatinine
ratio (PCR) and blood pressure should also be checked
·
urine microscopy may be used but time to analysis significantly
affects the number of red blood cells detected
NICE urgent cancer referral
guidelines were updated in 2015.
Urgent referral (i.e. within 2
weeks)
Aged >= 45 years AND:
·
unexplained visible haematuria without urinary tract infection,
or
·
visible haematuria that persists or recurs after successful
treatment of urinary tract infection
Aged >= 60 years AND have
unexplained nonvisible haematuria and either dysuria or a raised white cell
count on a blood test
Non-urgent referral
Aged 60 >= 60 years with
recurrent or persistent unexplained urinary tract infection
Since the investigation (or not) of
non-visible haematuria is such as a common dilemma a number of guidelines have
been published. They generally agree with NICE guidance, of note:
·
patients under the age of 40 years with normal renal function,
no proteinuria and who are normotensive do not need to be referred and may be
managed in primary care
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Hyperkalaemia: management
Untreated hyperkalaemia may cause
life-threatening arrhythmias. Precipitating factors should be addressed (e.g.
acute renal failure) and aggravating drugs stopped (e.g. ACE inhibitors).
Management may be categorised by the aims of treatment
Stabilisation of the cardiac
membrane
·
intravenous calcium gluconate
o does NOT lower serum potassium
levels
Short-term shift in potassium from
extracellular to intracellular fluid compartment
·
combined insulin/dextrose infusion
·
nebulised salbutamol
Removal of potassium from the body
·
calcium resonium (orally or enema)
o enemas are more effective than oral
as potassium is secreted by the rectum
·
loop diuretics
·
dialysis
o haemofiltration/haemodialysis
should be considered for patients with AKI with persistent hyperkalaemia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Diabetes insipidus
Diabetes insipidus (DI) is a
condition characterised by either a deficiency of antidiuretic hormone, ADH,
(cranial DI) or an insensitivity to antidiuretic hormone (nephrogenic DI).
Causes of cranial DI
·
idiopathic
·
post head injury
·
pituitary surgery
·
craniopharyngiomas
·
histiocytosis X
·
DIDMOAD is the association of cranial Diabetes Insipidus,
Diabetes Mellitus, Optic Atrophy and Deafness (also known as Wolfram's
syndrome)
·
haemochromatosis
Causes of nephrogenic DI
·
genetic: the more common form affects the vasopression (ADH)
receptor, the less common form results from a mutation in the gene that encodes
the aquaporin 2 channel
·
electrolytes: hypercalcaemia, hypokalaemia
·
drugs: demeclocycline, lithium
·
tubulo-interstitial disease: obstruction, sickle-cell,
pyelonephritis
Features
·
polyuria
·
polydipsia
Investigation
·
high plasma osmolality, low urine osmolality
·
a urine osmolality of >700 mOsm/kg excludes diabetes
insipidus
·
water deprivation test
Management
·
nephrogenic diabetes insipidus: thiazides, low salt/protein diet
- central diabetes insipidus can be
treated with desmopressin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Haemolytic uraemic syndrome
Haemolytic uraemic syndrome is
generally seen in young children and produces a triad of:
·
acute kidney injury
·
microangiopathic haemolytic anaemia
·
thrombocytopenia
Most cases are secondary (termed
'typical HUS'):
·
classically Shiga toxin-producing Escherichia coli (STEC)
0157:H7 ('verotoxigenic', 'enterohaemorrhagic'). This is the
most common cause in children, accounting for over 90% of cases
·
pneumococcal infection
·
HIV
·
rare: systemic lupus erythematosus, drugs, cancer
Primary HUS ('atypical') is due to
complement dysregulation.
Investigations
·
full blood count: anaemia, thrombocytopaenia, fragmented blood
film
·
U&E: acute kidney injury
·
stool culture
o looking for evidence of STEC
infection
o PCR for Shiga toxins
Management
·
treatment is supportive e.g. Fluids, blood transfusion and
dialysis if required
·
there is no role for antibiotics, despite the preceding diarrhoeal illness in many patients
·
the indications for plasma exchange in HUS are complicated. As a
general rule plasma exchange is reserved for severe cases of HUS not associated
with diarrhoea
·
eculizumab (a C5 inhibitor monoclonal antibody) has evidence of
greater efficiency than plasma exchange alone in the treatment of adult
atypical HUS
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Minimal change disease
Minimal change disease nearly
always presents as nephrotic syndrome, accounting for 75% of cases in children
and 25% in adults.
The majority of cases are
idiopathic, but in around 10-20% a cause is found:
·
drugs: NSAIDs, rifampicin
·
Hodgkin's lymphoma, thymoma
·
infectious mononucleosis
Pathophysiology
·
T-cell and cytokine-mediated damage to the glomerular basement
membrane → polyanion loss
·
the resultant reduction of electrostatic charge → increased
glomerular permeability to serum albumin
Features
·
nephrotic syndrome
·
normotension - hypertension is rare
·
highly selective proteinuria
o only intermediate-sized proteins
such as albumin and transferrin leak through the glomerulus
·
renal biopsy
o normal glomeruli on light
microscopy
o electron microscopy shows fusion of
podocytes and effacement of foot processes
Management
·
majority of cases (80%) are steroid-responsive
·
cyclophosphamide is the next step for steroid-resistant cases
Prognosis is overall good, although
relapse is common. Roughly:
·
1/3 have just one episode
·
1/3 have infrequent relapses
·
1/3 have frequent relapses which stop before adulthood
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Renal transplant: HLA typing and graft failure
The human leucocyte antigen (HLA)
system is the name given to the major histocompatibility complex (MHC) in
humans. It is coded for on chromosome 6.
Some basic points on the HLA system
·
class 1 antigens include A, B and C. Class 2 antigens include
DP,DQ and DR
·
when HLA matching for a renal transplant the relative importance
of the HLA antigens are as follows DR > B > A
Graft survival
·
1 year = 90%, 10 years = 60% for cadaveric transplants
·
1 year = 95%, 10 years = 70% for living-donor transplants
Post-op problems
·
ATN of graft
·
vascular thrombosis
·
urine leakage
·
UTI
Hyperacute rejection (minutes to
hours)
·
due to pre-existing antibodies against ABO or HLA antigens
·
an example of a type II hypersensitivity reaction
·
leads to widespread thrombosis of graft vessels → ischaemia and
necrosis of the transplanted organ
·
no treatment is possible and the graft must be removed
Acute graft failure (< 6 months)
·
usually due to mismatched HLA. Cell-mediated (cytotoxic T cells)
·
other causes include cytomegalovirus infection
·
may be reversible with steroids and immunosuppressants
Causes of chronic graft failure
(> 6 months)
·
both antibody and cell mediated mechanisms cause fibrosis to the
transplanted kidney (chronic allograft nephropathy)
·
recurrence of original renal disease (MCGN > IgA > FSGS)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Acute interstitial nephritis
Acute interstitial nephritis
accounts for 25% of drug-induced acute kidney injury.
Causes
·
drugs: the most common cause, particularly antibiotics
o penicillin
o rifampicin
o NSAIDs
o allopurinol
o furosemide
·
systemic disease: SLE, sarcoidosis, and Sjögren's syndrome
·
infection: Hanta virus , staphylococci
Pathophysiology
·
histology: marked interstitial oedema and interstitial
infiltrate in the connective tissue between renal tubules
Features
·
fever, rash, arthralgia
·
eosinophilia
·
mild renal impairment
·
hypertension
Investigations
·
sterile pyuria
·
white cell casts
Tubulointerstitial nephritis with
uveitis
Tubulointerstitial nephritis with
uveitis (TINU) usually occurs in young females. Symptoms include fever,
weight loss and painful, red eyes. Urinalysis is positive for leukocytes and
protein.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Acute kidney injury: acute tubular necrosis vs. prerenal
uraemia
|
|
Pre-renal uraemia ('azotemia') |
Acute tubular necrosis |
|
Urine sodium |
< 20 mmol/L |
> 40 mmol/L |
|
Urine osmolality |
> 500 mOsm/kg |
< 350 mOsm/kg |
|
Fractional sodium excretion* |
< 1% |
> 1% |
|
Response to fluid challenge |
Good |
Poor |
|
Serum urea:creatinine ratio |
Raised |
Normal |
|
Fractional urea excretion** |
< 35% |
>35% |
|
Urine:plasma osmolality |
> 1.5 |
< 1.1 |
|
Urine:plasma urea |
> 10:1 |
< 8:1 |
|
Specific gravity |
> 1020 |
< 1010 |
|
Urine |
Normal/ 'bland' sediment |
Brown granular casts |
Prerenal uraemia - kidneys hold on
to sodium to preserve volume
*fractional sodium excretion =
(urine sodium/plasma sodium) / (urine creatinine/plasma creatinine) x 100
**fractional urea excretion =
(urine urea /blood urea ) / (urine creatinine/plasma creatinine) x 100
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
ADPKD: features
Features
·
hypertension
·
recurrent UTIs
·
abdominal pain
·
renal stones
·
haematuria
·
chronic kidney disease
Extra-renal manifestations
·
liver cysts (70% - the commonest extra-renal manifestation): may cause hepatomegaly
·
berry aneurysms (8%): rupture can cause subarachnoid haemorrhage
·
cardiovascular system: mitral valve prolapse, mitral/tricuspid incompetence,
aortic root dilation, aortic dissection
·
cysts in other organs: pancreas, spleen; very rarely: thyroid,
oesophagus, ovary
|
|
|
|
©
Image used on license from PathoPic |
|

Extensive cysts are seen in an enlarged kidney
|
|
|
|
©
Image used on license from Radiopaedia |
|

CT of the abdomen demonstrates both kidneys to be
markedly enlarged by innumerable cysts ranging in size from a few millimeters
to multiple centimeters with cysts also present in the liver
|
|
|
|
©
Image used on license from Radiopaedia |
|

CT showing multiple cysts of varying sizes in the liver,
and bilateral kidneys with little remaining normal renal parenchyma.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:25
Chronic kidney disease: mineral bone disease management
Pathophysiology
Basic problems in chronic kidney
disease (CKD):
·
1-alpha hydroxylation normally occurs in the kidneys → CKD leads
to low vitamin D
·
the kidneys normally excrete phosphate → CKD leads to high
phosphate
This, in turn, causes other
problems:
·
the high phosphate level 'drags'
calcium from the bones, resulting in osteomalacia
·
low calcium: due to lack of vitamin D, high phosphate
·
secondary hyperparathyroidism: due to low calcium, high
phosphate and low vitamin D
Management
The aim is to reduce phosphate and
parathyroid hormone levels.
Overview
·
reduced dietary intake of phosphate is the first-line management
·
phosphate binders
·
vitamin D: alfacalcidol, calcitriol
·
parathyroidectomy may be needed in some cases
Phosphate binders
·
aluminium-based binders are less commonly used now
·
calcium-based binders
o problems include hypercalcemia and vascular calcification
·
sevelamer
o a non-calcium based binder that is
now increasingly used
o binds to dietary phosphate and
prevents its absorption
o also appears to have other
beneficial effects including reducing uric acid levels and improving the lipid
profiles of patients with chronic kidney disease
|
|
|
|
©
Image used on license from Radiopaedia |
|

X-ray of a Brown tumour caused by secondary
hyperparathyroidism in a young female with chronic kidney disease
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Erythropoietin
Erythropoietin is a haematopoietic
growth factor that stimulates the production of erythrocytes. Erythropoietin is secreted by the
kidney in response to cellular hypoxia. The main uses of erythropoietin
are to treat the anaemia associated with chronic kidney disease and that
associated with cytotoxic therapy.
Side-effects of erythropoietin
·
accelerated hypertension potentially leading to encephalopathy
and seizures (blood pressure increases in 25% of patients)
·
bone aches
·
flu-like symptoms
·
skin rashes, urticaria
·
pure red cell aplasia* (due to antibodies against
erythropoietin)
·
raised PCV increases risk of thrombosis (e.g. Fistula)
·
iron deficiency 2nd to increased erythropoiesis
There are a number of reasons why
patients may fail to respond to erythropoietin therapy:
·
iron deficiency
·
inadequate dose
·
concurrent infection/inflammation
·
hyperparathyroid bone disease
·
aluminium toxicity
*the risk is greatly reduced with
darbepoetin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Acid - base disorders
Metabolic acidosis
Metabolic acidosis is commonly
classified according to the anion gap.
Normal anion gap ( =
hyperchloraemic metabolic acidosis)
·
gastrointestinal bicarbonate loss: diarrhoea,
ureterosigmoidostomy, fistula
·
renal tubular acidosis
·
drugs: e.g. acetazolamide
·
ammonium chloride injection
·
Addison's disease
Raised anion gap
·
lactate: shock, hypoxia
·
ketones: diabetic ketoacidosis, alcohol
·
urate: renal failure
·
acid poisoning: salicylates, methanol
Metabolic alkalosis
Metabolic alkalosis may be caused
by a loss of hydrogen ions or a gain of bicarbonate. It is due mainly to
problems of the kidney or gastrointestinal tract
Causes
·
vomiting / aspiration (e.g. peptic ulcer leading to pyloric
stenos, nasogastric suction)
·
diuretics
·
liquorice, carbenoxolone
·
hypokalaemia
·
primary hyperaldosteronism
·
Cushing's syndrome
·
Bartter's syndrome
·
congenital adrenal hyperplasia
Respiratory acidosis
Respiratory acidosis may be caused
by a number of conditions
·
COPD
·
decompensation in other respiratory conditions e.g.
life-threatening asthma / pulmonary oedema
·
sedative drugs: benzodiazepines, opiate overdose
Respiratory alkalosis
Common causes
·
anxiety leading to hyperventilation
·
pulmonary embolism
·
salicylate poisoning
·
CNS disorders: stroke, subarachnoid haemorrhage, encephalitis
·
altitude
·
pregnancy
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Acute vs. chronic renal failure
Best way to differentiate is renal
ultrasound - most patients with CRF have bilateral small kidneys
Exceptions
·
autosomal dominant polycystic kidney disease
·
diabetic nephropathy
·
amyloidosis
·
HIV-associated nephropathy
Other features suggesting CRF
rather than ARF
·
hypocalcaemia (due to lack of vitamin D)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Chronic kidney disease: proteinuria
Proteinuria is an important marker
of chronic kidney disease, especially for diabetic nephropathy. NICE recommend
using the albumin:creatinine ratio (ACR) in preference to the
protein:creatinine ratio (PCR) when identifying patients with proteinuria as it
has greater sensitivity. For quantification and monitoring of proteinuria, PCR
can be used as an alternative, although ACR is recommended in diabetics. Urine
reagent strips are not recommended unless they express the result as an ACR
Approximate equivalent values
|
ACR
(mg/mmol) |
PCR (mg/mmol) |
Urinary protein excretion (g/24 h) |
|
30 |
50 |
0.5 |
|
70 |
100 |
1 |
Collecting an ACR sample
·
by collecting a 'spot' sample it avoids the need to collect
urine over a 24 hour period in order to detect or quantify proteinuria
·
should be a first-pass morning urine specimen
·
if the initial ACR is between 3 mg/mmol and 70 mg/mmol, this
should be confirmed by a subsequent early morning sample. If the initial ACR is
70 mg/mmol or more, a repeat sample need not be tested.
Interpreting the ACR results
·
the NICE guidelines state 'regard a confirmed ACR of 3 mg/mmol or more as clinically important proteinuria'
NICE recommendations for referral
to a nephrologist:
·
a urinary albumin:creatinine ratio (ACR) of 70 mg/mmol or more, unless known to be caused by diabetes and already
appropriately treated
·
a urinary ACR of 30 mg/mmol or more, together with persistent
haematuria (two out of three dipstick tests show 1+ or more of blood) after
exclusion of a urinary tract infection
·
consider referral to a nephrologist for people with an ACR
between 3-29 mg/mmol who have persistent haematuria and other risk factors such
as a declining eGFR, or cardiovascular disease
Frequency of monitoring eGFR
(number of times per year by eGFR and ACR categories) for people with or at
risk of CKD
|
eGFR
categories (mL/min/1.73 m2) |
ACR categories (mg/mmol) |
|
|
|
|
A1 (< 3) Normal to mildly increased |
A2 (3-30) Moderately increased |
A3 (> 30) Severely increased |
|
G1 >=90 Normal and high |
=< 1 |
1 |
>= 1 |
|
G2 60-89 Mild reduction related to
normal range for a young adult |
=< 1 |
1 |
>= 1 |
|
G3a 45-59 Mild to moderate reduction |
1 |
1 |
2 |
|
G3b 30-44 Moderate to severe reduction |
=< 2 |
2 |
>= 2 |
|
G4 15-29 Severe reduction |
2 |
2 |
3 |
|
G5 <15 Kidney failure |
4 |
>=4 |
>=4 |
Management
·
ACE inhibitors (or angiotensin II receptor blockers) are key in
the management of proteinuria
o they should be used first-line in
patients with coexistent hypertension and CKD
o if the ACR > 70 mg/mmol they are
indicated regardless of the patient's blood pressure
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Membranous glomerulonephritis
Membranous glomerulonephritis is
the commonest type of glomerulonephritis in adults and is the third most common
cause of end-stage renal failure (ESRF). It usually presents with nephrotic
syndrome or proteinuria.
Renal biopsy demonstrates:
·
electron microscopy: the basement membrane is thickened with
subepithelial electron dense deposits. This creates a 'spike and dome'
appearance
Causes
·
idiopathic: due to anti-phospholipase A2
antibodies
·
infections: hepatitis B, malaria, syphilis
·
malignancy (in 5-20%): prostate, lung, lymphoma, leukaemia
·
drugs: gold, penicillamine, NSAIDs
·
autoimmune diseases: systemic lupus erythematosus (class V
disease), thyroiditis, rheumatoid
Management
·
all patients should receive an ACE inhibitor or an angiotensin
II receptor blocker (ARB):
o these have been shown to reduce
proteinuria and improve prognosis
·
immunosuppression
o as many patients spontaneously
improve only patient with severe or progressive disease require
immunosuppression
o corticosteroids alone have not been
shown to be effective. A combination of corticosteroid + another agent such as
cyclophosphamide is often used
·
consider anticoagulation for high-risk patients
Prognosis - rule of thirds
·
one-third: spontaneous remission
·
one-third: remain proteinuric
·
one-third: develop ESRF
Good prognostic features include
female sex, young age at presentation and asymptomatic proteinuria of a modest
degree at the time of presentation.
|
|
|
|
©
Image used on license from PathoPic |
|

Silver-stained section showing thickened basement
membrane, subepithelial spikes
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Nephrotic syndrome
Triad of:
·
1. Proteinuria (> 3g/24hr) causing
·
2. Hypoalbuminaemia (< 30g/L) and
·
3. Oedema
Loss of antithrombin-III, proteins
C and S and an associated rise in fibrinogen levels predispose to thrombosis. Loss of thyroxine-binding globulin lowers the total, but not free,
thyroxine levels.
|
|
|
|
|
|
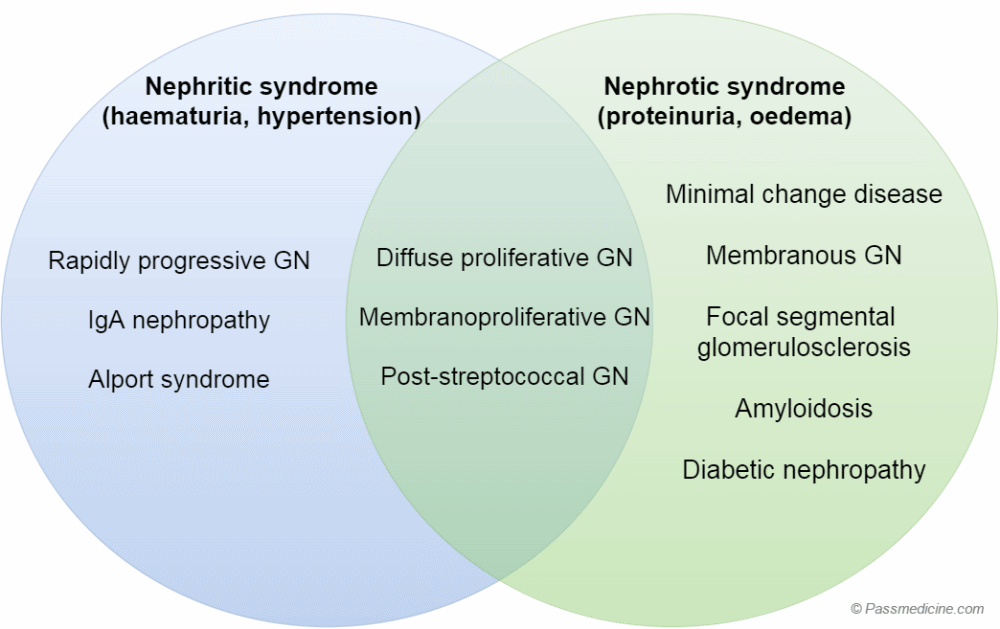
Diagram showing the glomerulonephritides and how they
typically present
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Peritoneal dialysis
Peritoneal dialysis (PD) is a form
of renal replacement therapy. It is sometimes used as a stop-gap to
haemodialysis or for younger patients who do not want to have to visit hospital
three times a week.
The majority of patients do
Continuous Ambulatory Peritoneal Dialysis (CAPD), which involves four 2-litre
exchanges/day.
Complications
·
peritonitis: coagulase-negative staphylococci
such as Staphylococcus epidermidis is the most common cause. Staphylococcus
aureus is another common cause
·
sclerosing peritonitis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Acute kidney injury: pathophysiology
Basic steps
·
Final pathway is tubular cell death.
·
renal medulla is a relatively hypoxic environment making it
susceptible to renal tubular hypoxia.
·
Renovascular autoregulation maintains renal blood flow across a
range of arterial pressures.
·
Estimates of GFR are the best indices of renal function. Useful
clinical estimates can be obtained by considering serum creatinine, age, race,
gender and body size. eGFR calculations such as the Cockcroft and Gault
equation are less reliable in populations with high GFRs.
·
Nephrotoxic stimuli such as aminoglycosides and radiological
contrast media induce apoptosis. Myoglobinuria and haemolysis result in
necrosis. Overlap exists and proinflammatory cytokines play and important role
in potentiating ongoing damage.
·
Post-operative renal failure is more likely to occur in patients
who are elderly, have peripheral vascular disease, high BMI, have COPD, receive
vasopressors, are on nephrotoxic medication or undergo emergency surgery.
·
Avoiding hypotension will reduce the risk of renal tubular
damage.
·
There is no evidence that administration of ACE inhibitors or
dopamine reduces the incidence of post-operative renal failure.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:26
Alport's syndrome
Alport's syndrome is usually
inherited in an X-linked
dominant pattern*. It is due to a defect in the gene which codes
for type IV collagen resulting in an abnormal glomerular-basement membrane (GBM). The
disease is more severe in males with females rarely developing renal failure.
A favourite question is an Alport's
patient with a failing renal
transplant. This may be caused by the presence of anti-GBM antibodies leading to a
Goodpasture's syndrome like picture.
Alport's syndrome usually presents
in childhood. The following features may be seen:
·
microscopic haematuria
·
progressive renal failure
·
bilateral sensorineural deafness
·
lenticonus: protrusion of the lens surface into the anterior
chamber
·
retinitis pigmentosa
·
renal biopsy: splitting of lamina densa seen on
electron microscopy
Diagnosis
·
molecular genetic testing
·
renal biopsy
o electron microscopy: characteristic finding is of the longitudinal splitting of the
lamina densa of the glomerular basement membrane, resulting in a 'basket-weave'
appearance
*in around 85% of cases - 10-15% of
cases are inherited in an autosomal recessive fashion with rare autosomal
dominant variants existing
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Anti-glomerular basement membrane (GBM) disease
(Goodpasture's syndrome)
Anti-glomerular basement membrane
(GBM) disease (previously known as Goodpasture's syndrome) is a rare type of
small-vessel vasculitis associated with both pulmonary haemorrhage and rapidly
progressive glomerulonephritis. It is caused by anti-glomerular basement
membrane (anti-GBM) antibodies against type IV collagen. Goodpasture's syndrome
is more common in men (sex ratio 2:1) and has a bimodal age distribution (peaks
in 20-30 and 60-70 age bracket). It is associated with HLA DR2.
Features
·
pulmonary haemorrhage
·
rapidly progressive glomerulonephritis
o this typically results in a rapid
onset acute kidney injury
o nephritis → proteinuria +
haematuria
Investigations
·
renal biopsy: linear IgG deposits along the basement membrane
·
raised transfer factor secondary to pulmonary haemorrhages
Management
·
plasma exchange (plasmapheresis)
·
steroids
·
cyclophosphamide
One of the main complications is
pulmonary haemorrhage. Factors which increase the likelihood of this include:
·
smoking
·
lower respiratory tract infection
·
pulmonary oedema
·
inhalation of hydrocarbons
·
young males
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Arteriovenous fistulas
Arteriovenous fistulas are direct
connections between arteries and veins. They may occur pathologically but are
generally formed surgically to allow access for haemodialysis.
They are now regarded as the preferred method of access for
haemodialysis due to the lower rates of
complications.
The time taken for an arteriovenous
fistula to develop is 6 to 8 weeks.
Potential complications include:
·
infection
·
thrombosis
o may be detected by the absence of a
bruit
·
stenosis
o may present with acute limb pain
·
steal syndrome
|
|
|
|
Image
sourced from Wikipedia |
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Chronic kidney disease: bone disease
Basic problems in chronic kidney
disease
·
low vitamin D (1-alpha hydroxylation normally occurs in the
kidneys)
·
high phosphate
·
low calcium: due to lack of vitamin D, high phosphate
·
secondary hyperparathyroidism: due to low calcium, high
phosphate and low vitamin D
Several clinical manifestations may
result:
Osteitis fibrosa cystica
·
aka hyperparathyroid bone disease
Adynamic
·
reduction in cellular activity (both osteoblasts and
osteoclasts) in bone
·
may be due to over treatment with vitamin D
Osteomalacia
·
due to low vitamin D
Osteosclerosis
Osteoporosis
|
|
|
|
©
Image used on license from Radiopaedia |
|
X-ray of a Brown tumour caused by secondary
hyperparathyroidism in a young female with chronic kidney disease
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Diabetic nephropathy: management
Screening
·
all patients should be screened annually using urinary albumin:creatinine ratio (ACR)
·
should be an early morning specimen
·
ACR > 2.5 = microalbuminuria
Management
·
dietary protein restriction
·
tight glycaemic control
·
BP control: aim for < 130/80 mmHg
·
benefits independent of blood pressure control have been
demonstrated for ACE inhibitors (ACE-i) and angiotensin II receptor blockers
(A2RB). Combinations of ACE-i and A2RB are not commonly used anymore following
the ON-TARGET trial which showed worse outcomes for patients on dual blockade
·
control dyslipidaemia e.g. Statins
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
IgA nephropathy
IgA nephropathy (also known as
Berger's disease) is the commonest cause of glomerulonephritis worldwide. It
classically presents as macroscopic
haematuria in young people following an upper respiratory tract infection.
Associated conditions
·
alcoholic cirrhosis
·
coeliac disease/dermatitis herpetiformis
·
Henoch-Schonlein purpura
Pathophysiology
·
thought to be caused by mesangial deposition of
IgA immune complexes
·
there is considerable pathological overlap with Henoch-Schonlein
purpura (HSP)
·
histology: mesangial hypercellularity,
positive immunofluorescence for IgA & C3
Presentations
·
young male, recurrent episodes of macroscopic haematuria
·
typically associated with a recent respiratory tract infection
·
nephrotic range proteinuria is rare
·
renal failure is unusual and seen in a minority of patients
Differentiating between IgA
nephropathy and post-streptococcal glomerulonephritis
·
post-streptococcal glomerulonephritis is associated with low
complement levels
·
main symptom in post-streptococcal glomerulonephritis is
proteinuria (although haematuria can occur)
·
there is typically an interval between URTI and the onset of
renal problems in post-streptococcal glomerulonephritis
|
|
|
|
|
|
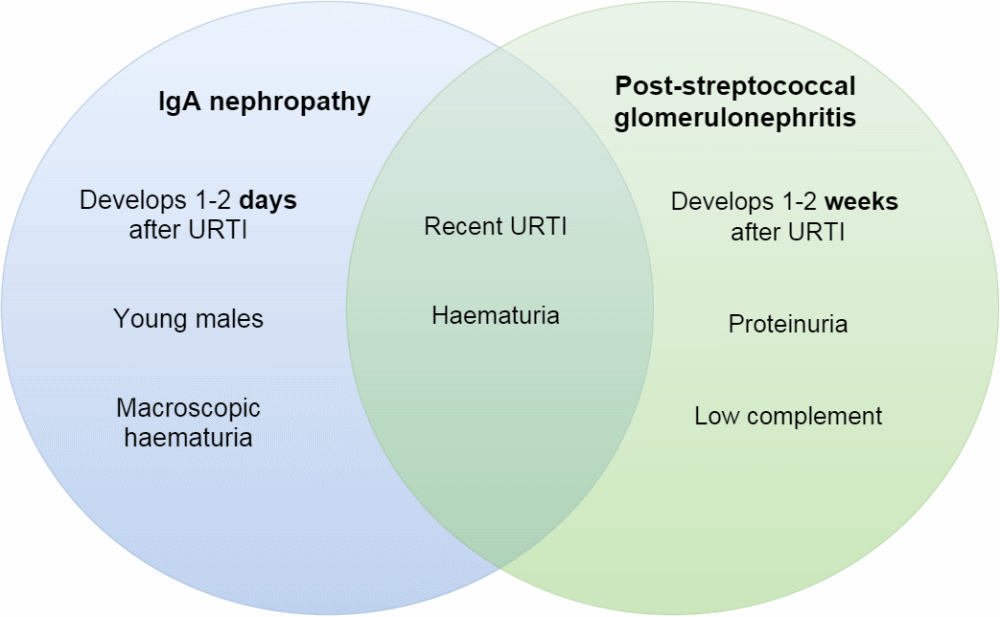
Management
·
steroids/immunosuppressants not be shown to be useful
Prognosis
·
25% of patients develop ESRF
·
markers of good prognosis: frank haematuria
·
markers of poor prognosis: male gender, proteinuria (especially
> 2 g/day), hypertension, smoking, hyperlipidaemia, ACE genotype DD
|
|
|
|
©
Image used on license from PathoPic |
|

Proliferation and hypercellularity of the mesangium is
seen in the glomerulus
|
|
|
|
©
Image used on license from PathoPic |
|

Immunostaining for IgA in a patient with HSP
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Nephrotic syndrome: complications
Complications
·
increased risk of thromboembolism related to
loss of antithrombin III and plasminogen in the urine
o deep vein thrombosis, pulmonary
embolism
o renal vein thrombosis, resulting in
a sudden deterioration in renal function
·
hyperlipidaemia
o increasing risk of acute coronary
syndrome, stroke etc
·
chronic kidney disease
·
increased risk of infection due to urinary immunoglobulin loss
·
hypocalcaemia (vitamin D and binding protein lost in urine)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Nephrotoxicity due to contrast media
Contrast media nephrotoxicity may be defined as a 25% increase in creatinine occurring within
3 days of the intravascular administration of contrast media.
Risk factors include
·
known renal impairment (especially diabetic nephropathy)
·
age > 70 years
·
dehydration
·
cardiac failure
·
the use of nephrotoxic drugs such as NSAIDs
Contrast-induced nephropathy occurs
2 -5 days after administration.
Prevention
·
the evidence base currently supports the use of intravenous 0.9% sodium chloride at a rate of 1 mL/kg/hour for 12
hours pre- and post- procedure. There is also evidence to support the use of
isotonic sodium bicarbonate
·
N-acetylcysteine has been given in the past but recent evidence
suggests it is not effective*
* Outcomes after Angiography with
Sodium Bicarbonate and Acetylcysteine. N Engl J Med. 2018;378(7):603
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Post-streptococcal glomerulonephritis
Post-streptococcal
glomerulonephritis typically occurs 7-14 days following a group A beta-haemolytic Streptococcus infection (usually Streptococcus pyogenes). It is caused by immune complex (IgG, IgM and C3)
deposition in the glomeruli. Young children are most commonly
affected.
Features
·
general
o headache
o malaise
·
visible haematuria
·
proteinuria
o this may result in oedema
·
hypertension
·
oliguria
·
bloods:
o low C3
o raised ASO titre
|
vi |
|
|
|
|
IgA nephropathy and post-streptococcal
glomerulonephritis are often confused as they both can cause renal disease
following an URTI
Renal biopsy features
·
post-streptococcal glomerulonephritis causes acute, diffuse
proliferative glomerulonephritis
·
endothelial proliferation with neutrophils
·
electron microscopy: subepithelial 'humps'
caused by lumpy immune complex deposits
·
immunofluorescence: granular or 'starry sky'
appearance
Carries a good prognosis



From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:27
Renal replacement therapy
Chronic kidney disease (CKD) is a
relatively common condition, affecting 1 in 8 people in the UK. Around 10% of
those with CKD will go on to develop renal failure, which is defined as a
glomerular filtration rate of less than 15ml/min. For patients with renal failure,
the management options are renal replacement therapy (RRT), to take over the
physiology of the kidneys, or conservative management, which will be
palliative.
There are several types of renal
replacement therapy available to patients:
·
haemodialysis
·
peritoneal dialysis
·
renal transplant
The decision about which RRT option
to pick should be made jointly by the patient and their healthcare team, taking
into account the following:
·
predicted quality of life
·
predicted life expectancy
·
patient preference
·
co-existing medical conditions
Haemodialysis is the most
common form of renal replacement therapy. This involves regular filtration of
the blood through a dialysis machine in hospital. Most patients need dialysis 3
times per week, with each session lasting 3-5 hours. At least 8 weeks before
the commencement of treatment, the patient must undergo surgery to create an
arteriovenous fistula, which provides the site for haemodialysis. Most commonly
this is created in the lower arm. Some patients may be trained to perform home
haemodialysis so that they do not have to regularly attend hospital.
Peritoneal dialysis is another
form of renal replacement therapy where the filtration occurs within the
patient's abdomen. Dialysis solution is injected into the abdominal cavity
through a permanent catheter. The high dextrose concentration of the solution
draws waste products from the blood into the abdominal cavity across the
peritoneum. After several hours of dwell time, the dialysis solution is then
drained, removing the waste products from the body, and exchanged for new dialysis solution. There are two types of peritoneal
dialysis:
·
Continuous ambulatory peritoneal dialysis (CAPD) - as described
above, with each exchange lasting 30-40 minutes and each dwell time lasting 4-8 hours. The patient may go about their normal
activities with the dialysis solution inside their abdomen
·
Automated peritoneal dialysis (APD) - a dialysis machine fills
and drains the abdomen while the patient is sleeping, performing 3-5 exchanges over 8-10 hours each night
Renal transplantation involves the
receipt of a kidney from either a live or deceased donor. The average wait for
a kidney in the UK is 3 years, though patients may also receive kidneys donated
by cross-matched friends or family. The donor kidney is transplanted into the
groin, with the renal vessels connected to the external iliac vessels. The
failing kidneys are not removed. Following transplantation, the patient must
take life-long immunosuppressants to prevent rejection of the new kidney. The
average lifespan of a donor kidney is 10-12 years from deceased donors and
12-15 years from living donors.
Complications of renal replacement
therapy
|
Haemodialysis |
Peritoneal dialysis |
Renal transplantation |
|
Site infection |
Peritonitis |
DVT / PE |
|
Endocarditis |
Sclerosing peritonitis |
Opportunistic infection |
|
Stenosis at site |
Catheter infection |
Malignancies (particularly lymphoma and
skin cancer) |
|
Hypotension |
Catheter blockage |
Bone marrow suppression |
|
Cardiac arrhythmia |
Constipation |
Recurrence of original disease |
|
Air embolus |
Fluid retention |
Urinary tract obstruction |
|
Anaphylactic reaction to sterilising
agents |
Hyperglycaemia |
Cardiovascular disease |
|
Disequilibration syndrome |
Hernias |
Graft rejection |
|
|
Back pain |
|
|
|
Malnutrition |
|
The average life expectancy of a
patient with renal failure that does not receive renal replacement therapy is 6
months. The symptoms of renal failure that is not being adequately managed with
RRT are:
·
breathlessness
·
fatigue
·
insomnia
·
pruritus
·
poor appetite
·
swelling
·
weakness
·
weight gain/loss
·
abdominal cramps
·
nausea
·
muscle cramps
·
headaches
·
cognitive impairment
·
anxiety
·
depression
·
sexual dysfunction
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Renal transplant: immunosuppression
Example regime
·
initial: ciclosporin/tacrolimus with a monoclonal antibody
·
maintenance: ciclosporin/tacrolimus with MMF or sirolimus
·
add steroids if more than one steroid responsive acute rejection
episode
Ciclosporin
·
inhibits calcineurin, a phosphotase involved in T cell
activation
Tacrolimus
·
lower incidence of acute rejection compared to ciclosporin
·
also less hypertension and hyperlipidaemia
·
however, high incidence of impaired glucose tolerance and
diabetes
Mycophenolate mofetil (MMF)
·
blocks purine synthesis by inhibition of IMPDH
·
therefore inhibits proliferation of B and T cells
·
side-effects: GI and marrow suppression
Sirolimus (rapamycin)
·
blocks T cell proliferation by blocking the IL-2 receptor
·
can cause hyperlipidaemia
Monoclonal antibodies
·
selective inhibitors of IL-2 receptor
·
daclizumab
·
basilximab
Monitoring
Patients on long-term
immunosuppression for organ transplantation require regular monitoring for
complications such as:
Cardiovascular disease - tacrolimus
and ciclosporin can cause hypertension and hyperglycaemia. Tacrolimus can also
cause hyperlipidaemia. Patients must be monitored for accelerated
cardiovascular disease.
Renal failure - due to nephrotoxic
effects of tacrolimus and ciclosporin/graft rejection/recurrence of original
disease in transplanted kidney
Malignancy - patients should be
educated about minimising sun exposure to reduce the risk of squamous cell
carcinomas and basal cell carcinomas
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Spironolactone
Spironolactone is an aldosterone antagonist which acts in the cortical collecting duct.
Indications
·
ascites: patients with cirrhosis develop a secondary
hyperaldosteronism. Relatively large doses such as 100 or 200mg are often used
·
hypertension: used in some patients as a NICE 'step 4' treatment
·
heart failure (see RALES study below)
·
nephrotic syndrome
·
Conn's syndrome
Adverse effects
·
hyperkalaemia
·
gynaecomastia: less common with eplerenone
RALES
·
NYHA III + IV, patients already taking ACE inhibitor
·
low dose spironolactone reduces all cause mortality
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Urine
Hyaline casts
·
consist of Tamm-Horsfall protein (secreted by distal convoluted
tubule)
·
seen in normal urine, after exercise, during fever or with loop diuretics
Acute tubular necrosis
·
brown granular casts in urine
Prerenal uraemia
·
'bland' urinary sediment
Red cell casts
·
nephritic syndrome
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Acute kidney injury: NICE guidelines
This guideline tells what increases
the risk of AKI:
·
1. Emergency surgery, ie, risk of sepsis or hypovolaemia
·
2. Intraperitoneal surgery
·
3. CKD, ie if eGFR < 60
·
4. Diabetes
·
5. Heart failure
·
6. Age >65 years
·
7. Liver disease
·
8. Use of nephrotoxic drugs
It also defines the criteria for
diagnosing AKI
·
1. Rise in creatinine of 26 micromol/L or more in 48 hours OR
·
2. >= 50% rise in creatinine over 7 days OR
·
3. Fall in urine output to less than 0.5ml/kg/hour for more than
6 hours in adults (8 hours in children) OR
·
4. >= 25% fall in eGFR in children / young adults in 7 days.
Refer to a nephrologist if any of
the following apply:
·
1. Renal tranplant
·
2. ITU patient with unknown cause of AKI
·
3. Vasculitis/ glomerulonephritis/ tubulointerstitial nephritis/
myeloma
·
4. AKI with no known cause
·
5. Inadequate response to treatment
·
6. Complications of AKI
·
7. Stage 3 AKI (see guideline for details)
·
8. CKD stage 4 or 5
·
9. Qualify for renal replacement hyperkalaemia / metabolic
acidosis/ complications of uraemia/ fluid overload (pulmonary oedema)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Chronic kidney disease: hypertension
The majority of patients with
chronic kidney disease (CKD) will require more than two drugs to treat
hypertension. ACE inhibitors are first line and are particularly helpful in
proteinuric renal disease (e.g. diabetic nephropathy). As these drugs tend to
reduce filtration pressure a small fall in glomerular filtration pressure (GFR)
and rise in creatinine can be expected. NICE suggest that a decrease in eGFR of
up to 25% or a rise in creatinine of up to 30% is acceptable, although any rise
should prompt careful monitoring and exclusion of other causes (e.g. NSAIDs). A
rise greater than this may indicate underlying renovascular disease.
Furosemide is useful as a
anti-hypertensive in patients with CKD, particularly when the GFR falls to
below 45 ml/min*. It has the added benefit of lowering serum potassium. High
doses are usually required. If the patient becomes at risk of dehydration (e.g.
Gastroenteritis) then consideration should be given to temporarily stopping the
drug
*the NKF K/DOQI guidelines suggest
a lower cut-off of less than 30 ml/min
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Fibromuscular dysplasia
Renal artery stenosis secondary to
atherosclerosis accounts for around 90% of renal vascular disease, with
fibromuscular dysplasia being the most common cause of the remaining 10%.
Epidemiology
·
90% of patients are female
Features
·
hypertension
·
chronic kidney disease or more acute renal failure e.g. secondary to ACE-inhibitor initiation
·
'flash' pulmonary oedema
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Fluid compartment physiology
Body fluid compartments comprise
intracellular and extracellular compartments. The latter includes interstitial
fluid, plasma and transcellular fluid.
Typical figures are based on the 70
Kg male.
Body fluid volumes
|
Compartment |
Volume in litres |
Percentage of total volume |
|
Intracellular |
28 L |
60-65% |
|
Extracellular |
14 L |
35-40% |
|
Plasma |
3 L |
5% |
|
Interstitial |
10 L |
24% |
|
Transcellular |
1 L |
3% |
Figures are approximate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Focal segmental glomerulosclerosis
Focal segmental glomerulosclerosis
(FSGS) is a cause of nephrotic syndrome and chronic kidney disease. It
generally presents in young adults.
Causes
·
idiopathic
·
secondary to other renal pathology e.g. IgA nephropathy, reflux
nephropathy
·
HIV
·
heroin
·
Alport's syndrome
·
sickle-cell
Focal segmental glomerulosclerosis
is noted for having a high recurrence rate in renal transplants.
Investigations
·
renal biopsy
o focal and segmental sclerosis and
hyalinosis on light microscopy
o effacement of foot processes on
electron microscopy
Management
·
steroids +/- immunosuppressants
Prognosis
·
untreated FSGS has a < 10% chance of spontaneous remission
|
|
|
|
©
Image used on license from PathoPic |
|

Sclerosis of the glomerulus is seen next to Bowman's
capsule
|
|
|
|
©
Image used on license from PathoPic |
|

Sclerosis is seen in the perihilar region of the
glomerulus
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Hypokalaemia: features
Features
·
muscle weakness, hypotonia
·
hypokalaemia predisposes patients to digoxin toxicity - care
should be taken if patients are also on diuretics
ECG features
·
U waves
·
small or absent T waves
·
prolonged PR interval
·
ST depression
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Polyuria
A recent review in the BMJ
categorised the causes of polyuria by how common they were. This does not of
course tally with how common they are in exams!
Common (>1 in 10)
·
diuretics, caffeine & alcohol
·
diabetes mellitus
·
lithium
·
heart failure
Infrequent (1 in 100)
·
hypercalcaemia
·
hyperthyroidism
Rare (1 in 1000)
·
chronic renal failure
·
primary polydipsia
·
hypokalaemia
Very rare (<1 in 10 000)
·
diabetes insipidus
Jakes A, Bhandari S. Investigating
polyuria. BMJ 2013;347:f6772.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Reflux nephropathy
Overview
·
term used to chronic pyelonephritis secondary to vesico-uretic
reflux
·
commonest cause of chronic pyelonephritis
·
scarring usually occurs in first 5 years
·
strong genetic disposition
·
renal scar may produce increased quantities of renin causing
hypertension
Diagnosis
·
micturating cystography
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:28
Renal artery stenosis (secondary to atherosclerosis)
Renal artery stenosis secondary to
atherosclerosis accounts for around 90% of renal vascular disease, with
fibromuscular dysplasia being the most common cause of the remaining 10%.
Features
·
hypertension
·
chronic kidney disease
·
'flash pulmonary oedema'
From <https://www.passmedicine.com/review/textbook.php?s=#>
Primary and secondary
aldosteronism can be differentiated by looking at the renin levels. If renin is
high then a secondary cause is more likely, i.e renal artery stenosis.
Renal
artery stenosis - the patient has a high renin level and therefore a secondary
aldosteronism is more likely. The reduced perfusion results in decreased
stimulation of the baroreceptors (or stretch receptors) in the wall of the
afferent arteriole. The renin–angiotensin–aldosterone system is activated and
with the increased aldosterone the potassium may be low, and the sodium high.
From <https://www.passmedicine.com/question/questions.php?q=0>
24 December 2020
14:28
Sterile pyuria
Causes
·
partially treated UTI
·
urethritis e.g. Chlamydia
·
renal tuberculosis
·
renal stones
·
appendicitis
·
bladder/renal cell cancer
·
adult polycystic kidney disease
·
analgesic nephropathy
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:29
Systemic lupus erythematosus: renal complications
Lupus nephritis is a severe
manifestation of systemic lupus erythematosus (SLE) that can result in
end-stage renal disease. SLE patients should be monitored by performing
urinalysis at regular check-up appointments to rule out proteinuria.
WHO classification
·
class I: normal kidney
·
class II: mesangial glomerulonephritis
·
class III: focal (and segmental) proliferative
glomerulonephritis
·
class IV: diffuse proliferative glomerulonephritis
·
class V: diffuse membranous glomerulonephritis
·
class VI: sclerosing glomerulonephritis
Class IV (diffuse proliferative
glomerulonephritis) is the most common and severe form. Renal biopsy
characteristically shows the following findings:
·
glomeruli shows endothelial and mesangial proliferation,
'wire-loop' appearance
·
if severe, the capillary wall may be thickened secondary to
immune complex deposition
·
electron microscopy shows subendothelial immune complex deposits
·
granular appearance on immunofluorescence
|
|
|
|
©
Image used on license from PathoPic |
|

Diffuse proliferative SLE. Proliferation of endothelial
and mesangial cells. The thickening of the capillary wall results in a
'wire-loop' appearance. Some crescents are present.
Management
·
treat hypertension
·
corticosteroids if clinical evidence of disease
·
immunosuppressants e.g. azathioprine/cyclophosphamide
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
17:16
Acute kidney injury: a very basic introduction
Acute kidney injury (AKI),
previously termed acute renal failure, describes a reduction in renal function
following an insult to the kidneys. In years gone by the kidneys were very much
a neglected organ in acute medicine - the recognition of decreasing renal
function was often slow and action limited. Around 15% of patients admitted to
hospital develop AKI.
Whilst most patients with AKI
recover their renal function there are many patients who will have long term
impaired kidney function due to AKI. As well as long-term morbidity, AKI may
also result in acute complications including death. Whilst exact figures are
difficult to calculate NICE estimate that inpatient mortality of AKI in the UK
might typically be 25-30% or more.
Pre-renal:
·
Caused by inadequate
renal perfusion e.g. dehydration, haemorrhage, heart failure, sepsis
·
Kidneys act to
concentrate urine and retain sodium - urine osmolality high, urine sodium low
Renal:
·
Most common = acute
tubular necrosis
·
Damage to tubular
cells due to prolonged ischaemia or toxins
·
Kidneys can no longer
concentrate urine or retain sodium - urine osmolality low, urine sodium high
·
Rarer causes = acute
glomerulonephritis, acute interstitial nephritis
Post-renal:
·
Obstruction of urinary
tract
·
Usually identified
with hydronephrosis on renal ultrasound
|
|
|
|
©
Image used on license from PathoPic |
|

Specimen from a patient who had an acute kidney injury.
Note the marked pallor of the cortex in certain areas, contrasting to the
darker areas of surviving medullary tissue.
What causes AKI?
Causes of AKI are traditionally
divided into prerenal, intrinsic and postrenal causes
Prerenal
Think of what causes big problems
in other major organs. In the heart, a lack of blood flow (ischaemia) to the
myocardium causes a myocardial infarction. In a similar fashion, 85% of strokes
are caused by ischaemia to the brain. The same goes for the kidneys. One of the
major causes of AKI is ischaemia, or lack of blood flowing to the kidneys.
Examples
·
hypovolaemia secondary to diarrhoea/vomiting
·
renal artery stenosis
Intrinsic
The second group of causes relate
to intrinsic damage to the glomeruli, renal tubules or interstitium of the
kidneys themselves. This may be due to toxins (drugs, contrast etc) or
immune-mediated glomuleronephritis.
Examples
·
glomerulonephritis
·
acute tubular necrosis (ATN)
·
acute interstitial nephritis (AIN), respectively
·
rhabdomyolysis
·
tumour lysis syndrome
Postrenal
The third group relates to problems
after the kidneys. This is where there is an obstruction to the urine coming
from the kidneys resulting in things 'backing-up' and affecting the normal
renal function. An example could be a unilateral ureteric stone or bilateral
hydroneprosis secondary to acute urinary retention caused by benign prostatic
hyperplasia.
Examples
·
kidney stone in ureter or bladder
·
benign prostatic hyperplasia
·
external compression of the ureter
|
|
|
|
©
Image used on license from PathoPic |
|

This patient had an invasive papillary tumour of the
distal left ureter, indicated by the arrow. This resulted in the ureter
becoming blocked, resulting in a left hydroureter and hydronephrosis. Note the
thinning of the renal cortex of the left kidney compared to the right.
Who is at an increased risk of AKI?
One of the keys to reducing the
incidence of AKI is identifying patient who are at increased risk. NICE support
this approach and have published guidelines suggesting which patients are at
greater risk.
Risk factors for AKI include:
·
chronic kidney disease
·
other organ failure/chronic disease e.g. heart failure, liver
disease, diabetes mellitus
·
history of acute kidney injury
·
use of drugs with nephrotoxic potential (e.g. NSAIDs, aminoglycosides, ACE
inhibitors, angiotensin II receptor antagonists [ARBs] and diuretics) within the past week
·
use of iodinated contrast agents within the past week
·
age 65 years or over
oliguria (urine output less than
0.5 ml/kg/hour)
·
neurological or cognitive impairment or disability, which may
mean limited access to fluids because of reliance on a carer
Preventing AKI
By identifying patients at
increased risk of AKI (see above) it may be possible to take steps to reduce
the risk. For example, patients who are at risk of AKI and who are undergoing
an investigation requiring contrast are usually given IV fluids to reduce the
risk. Certain drugs such as ACE inhibitors and ARBs may also be temporarily
stopped.
What happens when kidneys stop
working?
It's best to work backwards and
think about what kidneys actually do. The kidneys are primarily responsible for
fluid balance and maintaining homeostasis. Therefore two of the key ways AKI
may be detected are:
·
a reduced urine output. This is termed oliguria and is defined
as a urine output of less than 0.5
ml/kg/hour
·
fluid overload
·
a rise in molecules that the kidney normal excretes/maintains a
careful balance of. Examples include potassium, urea and creatinine
Symptoms and signs
Many patients with early AKI may
experience no symptoms. However, as renal failure progresses the following may
be seen:
·
reduced urine output
·
pulmonary and peripheral oedema
·
arrhythmias (secondary to changes in potassium and acid-base
balance)
·
features of uraemia (for example, pericarditis or
encephalopathy)
Detection
One of the most common blood tests
performed on the wards is 'urea and electrolytes' or 'U&Es'. This returns a
number of markers, including
·
sodium
·
potassium
·
urea
·
creatinine
NICE recommend that we can use a
variety of different criteria to make an official diagnosis of AKI. They state:
Detect acute kidney injury, in line with the (p)RIFLE,
AKIN or KDIGO definitions, by using any of the following criteria:
·
a rise in serum creatinine of 26 micromol/litre or greater
within 48 hours
·
a 50% or greater rise in serum creatinine known or presumed to
have occurred within the past 7 days
·
a fall in urine output to less
than 0.5 ml/kg/hour for more than 6 hours in adults and more than
Urinalysis
·
all patients with suspected AKI should have urinalysis
Imaging
·
if patients have no identifiable cause for the deterioration or
are at risk of urinary tract obstruction they should have a renal ultrasound within 24 hours of assessment.
Management
The management of AKI is largely
supportive. This means patients require careful fluid balance to ensure that
the kidneys are properly perfused but not excessively to avoid fluid overload.
It is also important to review
a patient's medication list to see what treatments may either
be exacerbating their renal dysfunction or may be dangerous as a consequence of
renal dysfunction. The table below gives some examples of common drugs:
|
Usually
safe to continue in AKI |
Should be stopped in AKI as may worsen
renal function |
May have to be stopped in AKI as
increased risk of toxicity (but doesn't usually worsen AKI itself) |
|
• Paracetamol • Warfarin • Statins • Aspirin (at a
cardioprotective dose of 75mg od) • Clopidogrel • Beta-blockers |
• NSAIDs (except if aspirin at cardiac dose e.g. 75mg od) • Aminoglycosides • ACE inhibitors • Angiotensin II
receptor antagonists • Diuretics |
• Metformin • Lithium • Digoxin |
Treatments which are not recommend include the routine use of loop diuretics (to artificially boost
urine output) and low-dose dopamine (in an attempt to increase renal
perfusion). There is however a role for loop diuretics in patients who
experience significant fluid overload.
Hyperkalaemia also needs prompt
treatment to avoid arrhythmias which may potentially be life-threatening. The
table below categorises the different treatments for hyperkalaemia:
|
Stabilisation
of the cardiac membrane |
• Short-term shift in potassium from
extracellular to intracellular fluid compartment |
• Removal of potassium from the body |
|
• Intravenous calcium
gluconate |
• Combined
insulin/dextrose infusion • Nebulised salbutamol |
• Calcium resonium
(orally or enema) • Loop diuretics • Dialysis |
Specialist input from a
nephrologist is required for cases where the cause is not known or where the
AKI is severe.
All patients with suspected AKI
secondary to urinary obstruction require prompt review by a urologist.
Renal replacement therapy (e.g.
haemodialysis) is used when a patient is not responding to medical treatment of
complications, for example hyperkalaemia, pulmonary oedema, acidosis or uraemia.
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:51
Metabolic acidosis
Metabolic acidosis is commonly
classified according to the anion gap. This can be calculated by: (Na+ + K+) - (Cl- + HCO-3). If a
question supplies the chloride level then this is often a clue that the anion
gap should be calculated. The normal range = 10-18 mmol/L
Normal anion gap ( =
hyperchloraemic metabolic acidosis)
·
gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula
·
renal tubular acidosis
·
drugs: e.g. acetazolamide
·
ammonium chloride injection
·
Addison's disease
Raised anion gap
·
lactate: shock, sepsis, hypoxia
·
ketones: diabetic ketoacidosis, alcohol
·
urate: renal failure
·
acid poisoning: salicylates, methanol
Metabolic acidosis secondary to
high lactate levels may be subdivided into two types:
·
lactic acidosis type A: sepsis, shock, hypoxia, burns
·
lactic acidosis type B: metformin
From <https://www.passmedicine.com/review/textbook.php?s=#>
Tuesday, 22 December 2020
18:25
Chronic kidney disease: anaemia
Patients with chronic kidney
disease (CKD) may develop anaemia due to a variety of factors, the most
significant of which is reduced erythropoietin levels. This is usually a
normochromic normocytic anaemia and becomes apparent when the GFR is less than
35 ml/min (other causes of anaemia should be considered if the GFR is > 60
ml/min). Anaemia in CKD predisposes to the development of left ventricular
hypertrophy - associated with a three fold increase in mortality in renal
patients
Causes of anaemia in renal failure
·
reduced erythropoietin levels - the most significant factor
·
reduced erythropoiesis due to toxic effects of uraemia on bone
marrow
·
reduced absorption of iron
·
anorexia/nausea due to uraemia
·
reduced red cell survival (especially in haemodialysis)
·
blood loss due to capillary fragility and poor platelet function
·
stress ulceration leading to chronic blood loss
Management
·
the 2011 NICE guidelines suggest a target haemoglobin of 10
- 12 g/dl
·
determination and optimisation of iron
status should be carried out prior to the administration of
erythropoiesis-stimulating agents (ESA). Many patients, especially those on
haemodialysis, will require IV iron
·
ESAs such as erythropoietin and darbepoetin should be used in
those 'who are likely to benefit in terms of quality of life and physical
function'
21 December 2020
21:51
Rhabdomyolysis
Rhabdomyolysis will typically
feature in the exam as a patient who has had a fall or prolonged epileptic
seizure and is found to have an acute kidney injury on admission.
Features
·
acute kidney injury with disproportionately raised creatinine
·
elevated creatine kinase (CK)
·
myoglobinuria
·
hypocalcaemia (myoglobin binds calcium)
·
elevated phosphate (released from myocytes)
·
hyperkalaemia (may develop before renal failure)
·
metabolic acidosis
Causes
·
seizure
·
collapse/coma (e.g. elderly patients collapses at home, found 8
hours later)
·
ecstasy
·
crush injury
·
McArdle's syndrome
·
drugs: statins (especially if co-prescribed with clarithromycin)
Management
·
IV fluids to maintain good urine output
·
urinary alkalinization is sometimes used
From <https://www.passmedicine.com/review/textbook.php?s=#>
Tuesday, 22 December 2020
18:20
Chronic kidney disease: eGFR and classification
Serum creatinine may not provide an
accurate estimate of renal function due to differences in muscle. For this
reason, formulas were developed to help estimate the glomerular filtration rate
(estimated GFR or eGFR). The most commonly used formula is the Modification of
Diet in Renal Disease (MDRD) equation, which uses the following variables:
·
serum creatinine
·
age
·
gender
·
ethnicity
Factors which may affect the result
·
pregnancy
·
muscle mass (e.g. amputees, body-builders)
·
eating red meat 12 hours prior to the sample being taken
CKD may be classified according to
GFR:
|
CKD
stage |
GFR range |
|
1 |
Greater than 90 ml/min, with some sign
of kidney damage on other tests (if all the kidney tests* are normal, there
is no CKD) |
|
2 |
60-90 ml/min with some sign of kidney
damage (if kidney tests* are normal, there is no CKD) |
|
3a |
45-59 ml/min, a moderate reduction in
kidney function |
|
3b |
30-44 ml/min, a moderate reduction in
kidney function |
|
4 |
15-29 ml/min, a severe reduction in
kidney function |
|
5 |
Less than 15 ml/min, established kidney
failure - dialysis or a kidney transplant may be needed |
*i.e. normal U&Es and no
proteinuria
eGFR
variables - CAGE - Creatinine, Age, Gender, Ethnicity
A
|
Albuminuria categories in CKD |
|
|
|
Category |
ACR (mg/g) |
Terms |
|
A1 |
<30 or <3 mg/mmol |
Normal to mildly increased |
|
A2 |
30-300 or 3-29 mg/mmol |
Moderately increased* |
|
A3 |
>300 >30mg mmol |
Severely increased** |
|
Abbreviations: ACR, albumin-to-creatinine ratio; CKD, chronic
kidney disease. *Relative to young adult level. **Including nephrotic syndrome (albumin excretion ACR >2220
mg/g) |
|
|
**Collectively referred to as “CGA
Staging”
From <https://www.kidney.org/professionals/explore-your-knowledge/how-to-classify-ckd>

21 December 2020
21:50
Henoch-Schonlein purpura
Henoch-Schonlein purpura (HSP) is
an IgA mediated small vessel
vasculitis. There is a degree of overlap with IgA nephropathy (Berger's disease). HSP is usually seen in children following an
infection.
Features
·
palpable purpuric rash (with localized oedema) over
buttocks and extensor surfaces of arms and legs
·
abdominal pain
·
polyarthritis
·
features of IgA nephropathy may occur e.g. haematuria, renal
failure
|
|
|
©
Image used on license from DermNet NZ |

Treatment
·
analgesia for arthralgia
·
treatment of nephropathy is generally supportive. There is
inconsistent evidence for the use of steroids and immunosuppressants
Prognosis
·
usually excellent, HSP is a self-limiting condition, especially
in children without renal involvement
·
around 1/3rd of patients have a relapse
|
|
|
©
Image used on license from DermNet NZ |

|
|
|
©
Image used on license from DermNet NZ |

From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
23:00
Anion gap
The anion gap is calculated by:
(sodium + potassium) - (bicarbonate
+ chloride)
A normal anion gap is 8-14 mmol/L
It is useful to consider in
patients with a metabolic acidosis:
Causes of a normal anion gap or
hyperchloraemic metabolic acidosis
·
gastrointestinal bicarbonate loss: diarrhoea, ureterosigmoidostomy, fistula
·
renal tubular acidosis
·
drugs: e.g. acetazolamide
·
ammonium chloride injection
·
Addison's disease
Causes of a raised anion gap
metabolic acidosis
·
lactate: shock, hypoxia
·
ketones: diabetic ketoacidosis, alcohol
·
urate: renal failure
·
acid poisoning: salicylates, methanol
·
5-oxoproline: chronic paracetamol use
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
20:18
ADPKD
Autosomal dominant polycystic
kidney disease (ADPKD) is the most common inherited cause of kidney disease,
affecting 1 in 1,000 Caucasians. Two disease loci have been identified, PKD1
and PKD2, which code for polycystin-1 and polycystin-2 respectively
|
ADPKD
type 1 |
ADPKD type 2 |
|
85% of cases |
15% of cases |
|
Chromosome 16 |
Chromosome 4 |
|
Presents with renal failure earlier |
|
The screening investigation for
relatives is abdominal ultrasound:
Ultrasound diagnostic criteria (in
patients with positive family history)
·
two cysts, unilateral or bilateral, if aged < 30 years
·
two cysts in both kidneys if aged 30-59 years
·
four cysts in both kidneys if aged > 60 years
Management
For select patients, tolvaptan (vasopressin
receptor 2 antagonist) may be an option. NICE
recommended it as an option for treating ADPKD in adults to slow the progression
of cyst development and renal insufficiency only if:
·
they have chronic kidney disease stage 2 or 3 at the start of
treatment
·
there is evidence of rapidly progressing disease and
·
the company provides it with the discount agreed in the patient
access scheme.
|
|
|
|
©
Image used on license from PathoPic |
|
Extensive cysts are seen in an enlarged kidney
From <https://www.passmedicine.com/question/questions.php?q=0#>
21 December 2020
23:10
Amyloidosis
Overview
·
amyloidosis is a term which describes the extracellular
deposition of an insoluble fibrillar protein termed amyloid
·
amyloid is derived from many different precursor proteins
·
in addition to the fibrillar component, amyloid also contains a
non-fibrillary protein called amyloid-P component, derived from the acute phase
protein serum amyloid P
·
other non-fibrillary components include apolipoprotein E and
heparan sulphate proteoglycans
·
the accumulation of amyloid fibrils leads to tissue/organ
dysfunction
Classification
·
systemic or localized
·
further characterised by precursor protein (e.g. AL in myeloma -
A for Amyloid, L for immunoglobulin Light chain fragments)
Diagnosis
·
Congo red staining: apple-green birefringence
·
serum amyloid precursor (SAP) scan
·
biopsy of rectal tissue



From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
18:10
Chronic kidney disease: causes
Common causes of chronic kidney
disease
·
diabetic nephropathy
·
chronic glomerulonephritis
·
chronic pyelonephritis
·
hypertension
·
adult polycystic kidney disease
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:35
Rapidly progressive
glomerulonephritis
Rapidly progressive
glomerulonephritis is a term used to describe a rapid loss of renal function
associated with the formation of epithelial crescents in the majority of
glomeruli.
Causes
·
Goodpasture's syndrome
·
Wegener's granulomatosis (c ANCA)
·
others: SLE, microscopic polyarteritis
Features
·
nephritic syndrome: haematuria with red cell casts, proteinuria,
hypertension, oliguria
·
features specific to underlying cause (e.g. haemoptysis with
Goodpasture's, vasculitic rash or sinusitis with Wegener's)
|
|
|
|
©
Image used on license from PathoPic |
|

Glomeruli are full of crescents.
|
|
|
|
©
Image used on license from PathoPic |
|

Another image showing the glomeruli full of crescents
cANCA
- c = Crescenteric glomerulonephritis!
From <https://www.passmedicine.com/question/questions.php?q=0>
Next question
Save my notes
Search
Go
Google
search on "Rapidly progressive glomerulonephritis"
Media
|
|
|
|
|
|
|
Osmosis
- YouTube |
50 |

From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:50
Fluid therapy
The prescription of intravenous
fluids is one of the most common tasks that junior doctors need to do.
In the 2013 guidelines NICE
recommend the following requirements for maintenance fluids:
·
25-30 ml/kg/day of water and
·
approximately 1 mmol/kg/day of potassium, sodium and chloride and
·
approximately 50-100 g/day of glucose to limit starvation ketosis
So, for a 80kg patient, for a 24
hour period, this would translate to:
·
2 litres of water
·
80mmol potassium
For the first 24 hours NICE
recommend the following::
When prescribing for routine maintenance alone, consider
using 25-30 ml/kg/day sodium chloride 0.18% in 4% glucose with 27 mmol/l
potassium on day 1 (there are other regimens to achieve this).
The amount of fluid patients
require obviously varies according to their recent and past medical history.
For example a patient who is post-op and is having significant losses from
drains will require more fluid whereas a patient with heart failure should be
given less fluid to avoid precipitating pulmonary oedema.
The table below shows the
electrolyte concentrations (in millimoles/litre) of plasma and the most
commonly used fluids:
|
|
Na+ |
Cl- |
K+ |
HCO3- |
Glucose |
|
Plasma |
135-145 |
98-105 |
3.5-5 |
22-28 |
- |
|
0.9% saline |
154 |
154 |
- |
- |
- |
|
5% glucose |
- |
- |
- |
- |
50g |
|
0.18% saline with 4% glucose |
30 |
30 |
- |
- |
40g |
|
Hartmann's solution |
131 |
111 |
5 |
29 |
- |
Specific points
0.9% saline
·
if large volumes are used there is an increased risk of
hyperchloraemic metabolic acidosis
Hartmann's
·
contains potassium and therefore should not be used in patients
with hyperkalaemia
From <https://www.passmedicine.com/review/textbook.php?s=#>
Wednesday, 23 December 2020
01:01
Haematuria
The management of patients with
haematuria is often difficult due to the absence of widely followed guidelines.
It is sometimes unclear whether patients are best managed in primary care, by
urologists or by nephrologists.
The terminology surrounding
haematuria is changing. Microscopic or dipstick positive haematuria is
increasingly termed non-visible haematuria whilst macroscopic haematuria is
termed visible haematuria. Non-visible haematuria is found in around 2.5% of
the population.
Causes of transient or spurious
non-visible haematuria
·
urinary tract infection
·
menstruation
·
vigorous exercise (this normally settles after around 3 days)
·
sexual intercourse
Causes of persistent non-visible
haematuria
·
cancer (bladder, renal, prostate)
·
stones
·
benign prostatic hyperplasia
·
prostatitis
·
urethritis e.g. Chlamydia
·
renal causes: IgA nephropathy, thin basement membrane disease
Spurious causes - red/orange urine,
where blood is not present on dipstick
·
foods: beetroot, rhubarb
·
drugs: rifampicin, doxorubicin
Management
Current evidence does not support
screening for haematuria. The incidence of non-visible haematuria is similar in
patients taking aspirin/warfarin to the general population hence these patients
should also be investigated.
Testing
·
urine dipstick is the test of choice for detecting haematuria
·
persistent non-visible haematuria is often defined as blood
being present in 2 out of 3 samples tested 2-3 weeks apart
·
renal function, albumin:creatinine (ACR) or protein:creatinine
ratio (PCR) and blood pressure should also be checked
·
urine microscopy may be used but time to analysis significantly
affects the number of red blood cells detected
NICE urgent cancer referral
guidelines were updated in 2015.
Urgent referral (i.e. within 2
weeks)
Aged >= 45 years AND:
·
unexplained visible haematuria without urinary tract infection,
or
·
visible haematuria that persists or recurs after successful
treatment of urinary tract infection
Aged >= 60 years AND have
unexplained nonvisible haematuria and either dysuria or a raised white cell
count on a blood test
Non-urgent referral
Aged 60 >= 60 years with
recurrent or persistent unexplained urinary tract infection
Since the investigation (or not) of
non-visible haematuria is such as a common dilemma a number of guidelines have
been published. They generally agree with NICE guidance, of note:
·
patients under the age of 40 years with normal renal function,
no proteinuria and who are normotensive do not need to be referred and may be
managed in primary care
22 December 2020
19:48
Hypokalaemia: features
Features
·
muscle weakness, hypotonia
·
hypokalaemia predisposes patients to digoxin toxicity - care
should be taken if patients are also on diuretics
ECG features
·
U waves
·
small or absent T waves
·
prolonged PR interval
·
ST depression
From <https://www.passmedicine.com/question/questions.php?q=0#>
This
gentleman has severe hypokalaemia, defined as a serum potassium < 2.5mmol/l.
Mild to moderate hypokalaemia can be asymptomatic but the more severe the
electrolyte derangement the more likely that symptoms will develop. Symptoms
include weakness, leg cramps, palpitations secondary to cardiac arrhythmias and
ascending paralysis.
Causes
can be secondary to:
1.) Increased potassium loss:
·
Drugs: thiazides, loop diuretics, laxatives,
glucocorticoids, antibiotics
·
GI losses: diarrhoea, vomiting, ileostomy
·
Renal causes: dialysis
·
Endocrine disorders: hyperaldosteronism,
Cushing's syndrome
2.) Trans-cellular shift
·
Insulin/glucose therapy
·
Salbutamol
·
Theophylline
·
Metabolic alkalosis
3.) Decreased potassium intake
4.) Magnesium depletion (associated with increased potassium
loss)
ECG changes seen in hypokalaemia include:
·
U waves
·
T wave flattening
·
ST segment changes
Treatment
of hypokalaemia depends on severity. Any causative agents should be removed.
Gradual replacement of potassium via the oral route is preferred if possible.
Mild
to moderate hypokalaemia 2.5 - 3.4 mmol/l can be treated with oral potassium
provided the patient is not symptomatic and there are no ECG changes.
Severe
hypokalaemia (<2.5mmol/l) or symptomatic hypokalaemia should be managed with
IV replacement. The patient should be managed in an area where cardiac
monitoring can take place. If there are no contraindications to fluid therapy
(e.g. volume overload, heart failure) potassium should be diluted to low
concentrations as higher concentrations can be phlebitic. The infusion rate
should not exceed 20mmol/hr. In this case, 3 bags of 0.9% Saline with 40mmol
KCL is the correct answer.
From <https://www.passmedicine.com/question/questions.php?q=0#>
Intrinsic AKI differences
01 January 2021
16:24
Membranous glomerulonephritis
histology:
basement membrane thickening on
light microscopy
subepithelial spikes on sliver
stain
positive immunohistochemistry for
PLA2
classically causes nephrotic
syndrome (protein +hypoalbuminaemia)
Membranous glomerulonephritis
also causes a hypercoagulable state,
Minimal
change disease would typically affect children, who would be normotensive, with
no haematuria and no findings on light microscopy.
Goodpasture's
disease would cause nephritic syndrome (never nephrotic), lung symptoms and
more systemic upset. It also would not cause these histology findings.
Focal
segmental glomerulosclerosis would cause similar symptoms, urine dip and blood
test findings to membranous glomeulonephritis but would not cause these
histology findings.
IgA
nephropathy is the commonest cause of glomerulonephritis in adults worldwide,
particularly affecting young males. It can cause nephrotic or nephritic
syndrome or isolated haematuria. It would not cause these histology findings.
From <https://www.passmedicine.com/question/questions.php?q=0>
nephrotic syndrome and nephritic
syndrome are on a continuous spectrum
Causes of bladder outlet
obstruction
04 January 2021
22:11
potential
causes of bladder outlet obstruction:
·
Genitalia: Meatal
stenosis, phimosis, paraphimosis, atrophic vaginitis
·
Urethra: Stones,
strictures, diverticulum, posterior urethral valves, carcinoma, surgery
·
Prostate: Benign
prostatic hyperplasia, calculi, abscess, prostate carcinoma
·
Gynaecologic:
Prolapse, cystocele, pregnancy, ovarian mass, uterine tumour, cervical tumour
·
Bladder: Calculi,
blood clot, tumour, bladder neck dysfunction
·
Bowel: Faecal
impaction
·
Neurogenic: Multiple
sclerosis, diabetes, spinal cord trauma, Parkinson disease, cerebrovascular
accident
From <https://mle.ncl.ac.uk/cases/page/17216/>
Pulmonary renal syndrome
04 January 2021
22:21
Pulmonary-renal syndrome is almost always a
manifestation of an underlying autoimmune disorder.
Goodpasture
syndrome is the prototype cause, but
PRS can also be caused by SLE, granulomatosis with polyangiitis, microscopic polyangiitis, and, less commonly, by other vasculitides, connective
tissue disorders, and drug-induced vasculitides.
From <https://mle.ncl.ac.uk/cases/page/16998/>
Pulmonary-renal syndrome (PRS) is
diffuse alveolar haemorrhage plus glomerulonephritis, often occurring
simultaneously. Cause is almost always an autoimmune disorder. Diagnosis is by
serologic tests and sometimes lung and renal biopsy. Treatment typically
includes immunosuppression with corticosteroids and cytotoxic drugs.
Pulmonary-renal syndrome (PRS) is
not a specific entity but is a syndrome that suggests a differential diagnosis
and a specific sequence of testing.
Systemic Symptoms: night sweats,
abdominal pain, bloody diarrhoea
Signs of Sepsis: Fever,
lymphadenopathy
Signs of Autoimmune Conditions:
Joint pains, myalgia, rash, sicca, epistaxis, deafness, ulcers
Other Significant PMH: DVT/ PE
thrombotic disorders, SLE, Autoimmune conditions

There are many potential reasons
for coughing up blood. Causes for haemoptysis include:
Bronchitis (acute or chronic),
the most common cause of coughing up blood. Haemoptysis due to bronchitis is
rarely life-threatening.
Bronchiectasis
Lung cancer or non-malignant lung
tumours
Use of anticoagulation
Pneumonia
Pulmonary embolism
Congestive heart failure,
especially due to mitral stenosis
Tuberculosis
Inflammatory or autoimmune
conditions (lupus, Granulomatosis with polyangiitis (GPA previously called
Wegener’s), Microscopic polyangiitis (MPA), or Eosinophilic granulomatosis with
polyangiitis (EGPA, previously called Churg-Strauss) and many others)
Pulmonary arteriovenous
malformations (AVMs)
Crack cocaine
Trauma, such as a gunshot wound
or motor vehicle accident
Dialysis indications
04 January 2021
22:58
AKI and
dialysis indications (AEIOU)
Acidosis
·
intractable metabolic
acidosis
·
Bic 14, PH <7.2
Electrolytes
·
severe persistent
hyperkalemia
·
>6 – esp if anuric
Intoxication
·
methanol, ethylene
glycol, lithium, aspirin
Overload :hypervolemia
·
Diuretics not
effective
·
Pulmonary oedema
Uraemia
·
uremic pericarditis
·
encephalopathy
From <https://mle.ncl.ac.uk/cases/page/17236/>
Lifestyle and health
23 December 2020
13:02
Health is a state of complete
physical, mental and social well-being and not merely the absence of disease or
infirmity. WHO and Health
What is classed as life style
Diet
Physical activity
Smoking
Alcohol
Non communicable diseases
modified by life style modification
Obesity
Type 2 Diabetes
Lipid Disorders
Atherosclerotic cardiovascular
diseases
Hypertension
Cancer
Best portions
·
33% Starchy carbohydrates Bulk of meals
·
33% Fruit & Vegetables 5+ a Day
·
15% Milk & Dairy 3 portions daily
·
12% Meat, Fish, Eggs, Beans Oily fish once a week
·
<8% High fat/sugary foods Avoid saturated fats
Exercise
Frequency: 3-5 days per week
Aerobic exercise: a minimum if 3
days a week are necessary to reach most exercise goals and minimize health
benefits
Strength training: a minimum of 2
days per week
Flexibility training: a minimum
of 3-5 days per week
Duration
Aerobic: 20-60 minutes of
continuous aerobic activity
Strength: 1-3 sets of 8-12
repetitions
Stretching: Stretch all muscle
groups and hold positions for 10-30 seconds
Benefits of exercise
Associated with lower all-cause
mortality rates
Increases life span
Prevention of cardiovascular disease, cancer (colon,
breast), type 2 diabetes, hypertension, obesity
Mitigates negative effects of
aging
Reduces dementia risk
Enhances executive function and
attention, processing speed, memory
Decreases symptoms of depression,
anxiety
Improves psychological well-being
Promotes brain cell growth
Alcohol
To keep health risks from alcohol
to a low level it is safest not to drink more than 14 units a week on
a regular basis
If you regularly drink as much as
14 units per week, it's best to spread your drinking evenly over three
or more days. If you have one or two heavy drinking episodes a week, you
increase your risk of long term illness and injury
Non-communicable diseases
(NCD)
23 December 2020
13:26
Non-communicable diseases (NCDs)
are also known as chronic diseases
Tend to be of long duration
Are mainly a result of lifestyle
behaviour habits
May also be caused by
non-modifiable risk factors such individual characteristics (age, sex, and
genetic factors)



NCD kill 41 million people
annually – that’s 71% of all global deaths
Each year, 15 million people die
prematurely from a NCD between the ages of 30 and 69 years
85% of these
"premature" deaths occur in low- and middle-income countries
In England, over 15 million
people live with NCDs
NCDs account for approximately
70% of the NHS annual budget
50% of all GP appointments
64% of outpatient appointments
70% of all inpatient bed days
Disproportionately affect people
in deprived areas more
Why increasing life expectancy
Vaccinations and antimicrobials
medication are now widespread
– reduced burden from infectious
(communicable) diseases
Living standards have improved
and lifestyles have changed dramatically
Economic prosperity &
globalisation
Urbanisation
Sedentary lifestyles

Dementia and mental illness may
be classified as NCDs.
Often patients have two or more chronic
diseases.
Cardiovascular
disease
These account for most NCD deaths
worldwide – killing 18 million people annually
In the UK, coronary heart disease
and stroke are the biggest causes of disability and death
Men are at greater risk than
women
Smoking, hypertension, harmful
alcohol consumption, physical inactivity, obesity and diet can all cause CVDs.
Cancers
Cancers are the second biggest
causes of morbidity and death and cause 9 million deaths annually worldwide
In the UK, 300,000 people are
diagnosed with cancer with 130,000 deaths
There are more than 200 types of
cancers: lung, colorectal and breast cancer are the top 3 causes of premature
morbidity
Cancer incidence increases with
age
Greatly affected by individual
lifestyle behaviours
Tobacco smoking alone is
estimated to cause more than a 25% of
all deaths from cancer
Note: although the number of
cancer survivors is rising, survivors often have worse overall health than the
rest of the population
Chronic respiratory
diseases
COPD causes 3.9 million deaths
annually
Around 835,000 people in the UK
have been diagnosed with COPD
additional 2 million people living
with the disease who have not been diagnosed.
Causes many years of disability
before death
Smoking is the most important
risk factor. Air pollution can also be a contributory cause
Public health smoking campaigns
have achieved success and smoking rates are decreasing in the UK. However,
there is a higher prevalence of smoking in more deprived areas.
Diabetes
Diabetes is a major
non-communicable disease causing 1.6 million deaths annually
Around 3 million people in the UK
have diabetes. This figure is expected to rise to 4 million people by 2025.
Diabetes has micro - and macro-
vascular complications resulting in poor quality of life and premature
mortality.
Almost 90% of new and existing
cases of diabetes are type 2.
Type 2 diabetes has a strong
association with obesity and diet
Changing lifestyle behaviours by
tackling obesity and hyperlipidaemia can have a major impact on the burden on
the disease
Preventing and managing NCDS

How do we reduce risk
factors on an individual level?
Monitoring blood pressure in the
community
Checking lipid profiles for at
risk patients - offering statins
Offering weight reduction
services for overweight and obese individuals
Referring smokers to smoking
cessation services
Encouraging an overall healthy
and active lifestyle

Epidemiology of Obesity
23 December 2020
13:34
|
|
|||
|
|
Since the 1970s, obesity has nearly tripled
worldwide The WHO estimated that by 2016 more than 1.9 billion
adults worldwide were overweight That’s 39% of the world population. Of those, 650 million were obese That’s 13% of the world population.
Adult obesity Obesity is no longer just a high-income country
problem. It is on the rise in low- and middle-income
countries, especially in urban settings. Worldwide, obesity is more prevalence that
underweight in every region except in parts of sub-Saharan Africa and Asia. UK: 66% of
population are either overweight or obese 1 in every 4 adults are obese The prevalence of obesity is similar among genders 67% of men and 60% of women Scotland has the highest proportion of obesity
(27.7%)
Prevalence of obesity if higher in the most deprived
areas than the least deprived areas. WHO estimated that by 2019: 38 million children under the age of 5 were
overweight or obese Over 340 million children and adolescents aged 5-19
were overweight or obese The prevalence of overweight and obesity among
children and adolescents has risen from 4% in 1975 to over 18% in 2016. This rise has been similar among both boys and girls UK: ·
For
children aged 4 & 5 years – 13% are overweight and 9% are obese ·
For
children aged 10 & 11 year olds – 14% are overweight while 20% are obese ·
Younger
generations are becoming obese earlier and staying obese into adulthood ·
Children
living in deprived areas are more likely to be obese Obesity and Social Deprivation The Marmot review was published on
February 2010 and looked at health inequalities in England Addressed the social determinants of
health, the conditions in which people are born, live, work and age and which
can lead to health inequalities. The review highlighted that there is a
strong relationship between obesity and health inequalities Obesity is attributed to the increased consumption
of ready meals and high calorie drinks.
These foods have higher levels of saturated fats, sugar, and salt, and
lower levels of micronutrients. Ready meals are: Often cheap Readily available at all times of the day More than 27% of adults and 20% of children eat food
from fast food outlets at least once a week.
On average, there are more fast food chains in
deprived areas than in more affluent areas. Public Health England estimated that there were
over 50,000 fast food takeaway, delivery services and fish and chip shops in
England. Those
in deprived areas are: More likely to eat healthy foods Become obese from a younger age Develop non-communicable diseases early
on NCDs further reduce their quality of
life And increases deprivation Projection trends suggest that by 2050,
half of the entire adult population worldwide will be obese. Obesity causes more than 30,000 deaths each year. Over 11, 000 hospital admissions It also reduces life expectancy by up to 8 years
(especially in severely obese individuals) Individuals with obesity are: ·
2.5
times more likely to develop high blood pressure ·
3
times more likely to develop colon cancer ·
5
times more likely to develop type 2 diabetes During the COVID-19 pandemic, evidence
suggests that obese or overweight patients who developed the illness had
poorer outcomes.
The NHS projects that the annual cost to the NHS
will to reach £9.7 billion and the cost to the wider economy will reach £49.9
billion by 2050 Obesity is preventable: …so chronic conditions that are caused by obesity
are also preventable. If we stop the obesity trend and reverse it
then we can Improve our patients’ quality of life Prevent unnecessary death Ultimately help our healthcare system |
||
|
|
|
||
|
|







Obesity Classification,
investigations and management
23 December 2020
13:40
Definition:
·
Abnormal or excessive
fat accumulation that presents a risk to health
·
Body Mass Index:
Commonly used
·
Waist circumference in
BMI <35
Obesity
classification- NICE

Ethnicity-
South Asian- 23 BMI obesity
Primary
cause- lifestyle
Secondary
cause:
Endocrine-
Cushing’s syndrome
Hypothyroid
Pseudohypoparathyroid
Hypothalamic disorders
Genetic-
Prader Willi
Laurence Moon
Bardet Biedel
Cohen’s
Alstrom’s
Medications-
Steroids
Tricyclic antidepressants
Phenothiazines
Sodium valproate
Sulphonyl ureas, Insulin
Psychiatric-
Eating disorders: Bulimia nervosa
Conditions associated with Obesity-
Osteoarthritis
Hypertension
Type 2 Diabetes
Obstructive sleep apnoea
Reflux Oesophagitis
Depression / Mental health problems
Asthma
Heart failure


Assessment:
BMI: Not enough
EOSS
4M


Medical management:
Life style modification
Behavioural modification
Psychology support- Motivational consultation
Dietician support
Specialised weight management service
Assessment, investigations, Treatment of co-morbidities
NHS 4 tier weight management:

Obesity – A Public Health
Perspective
23 December 2020
13:48
Overweight and obesity are
defined as excessive fat accumulation that pose a risk to health.
The body mass index (BMI) is a
crude population measure of obesity
BMI is calculated as a person’s
weight (in kilograms) divided by the square of his or her height (in metres).

7 Key cause-

–
to put it simply …
Obesity
and overweight are fundamentally a result of an energy imbalance between the
number of calories consumed and calories expended
While
there is an element of individual choice in food consumption, we must remember
that we live in an obesogenic world.
7 main causes of
obesity -
Increased consumption
of energy-dense foods
Food is often processed and high
in saturated fat and sugars
Ready meals are convenient and
readily available
Fast-food chains are widespread
with late opening hours
Marketing campaigns play a major
influential role
Increased food
production for commercial profit
Food producers are pressured to
turn a profit for stakeholders and make processed food in large volumes
This processed food is often sold
affordably to encourage consumption
An increase in
physical inactivity and sedentary lifestyle.
Changing work patterns (sitting
at desks rather than manual labour)
Technology advances including
changes to transportation ( more people are using cars, buses or trains rather than walking, biking etc…)
Poor physical
activity environment
There is reduced availability of
safe green spaces for outdoor activity, especially in urban settings.
Individual biological
physiology
Genes can impact how fat is
metabolised as well as individual perception of fullness
Individual psychology
Stress and low self-esteem can
impede a person’s ability to consciously control his or her food intake
Food can also be used as a
psychological reward
Social psychology
Collective societal beliefs about
food and body shape can play a role in determining how much people eat
These beliefs vary around the
world
Obesity and
overweight are major risk factors for non-communicable diseases including:
Cardiovascular diseases
Diabetes mellitus
Hypertension
Stroke
Musculoskeletal disorders
(especially osteoarthritis)
Cancers (including endometrial,
breast, ovarian, prostate, liver, gallbladder, kidney, and colon)
Dyslipidaemia
The risk of developing a
non-communicable disease increases as a person’s BMI increases.
Poor mental health
Poor quality sleep (sleep apnoea)
Increased stigmatization and
discrimination


What is Public Health England doing about obesity?
The Eatwell Guide shows how much of what we eat overall should come from each food group
to achieve a healthy, balanced diet.
Better Health Campaign
Launched on the 27th of July 2020
by Public Health England.
Response to national interest in
obesity during the COVID pandemic
It is an opportunity for a
“national reset moment”.
Gives individuals access to a
range of mobile apps and online tools to help them stay in shape and make
healthier food choices
It will also support people to
live healthier lives in general with smoking cessation and mental health
advise.
Reversing the obesity trend will
improve quality of life and reduce morbidity and mortality from NCDs
Dietetic Management of
Obesity
23 December 2020
14:17
Healthy eating will vary
according to a person’s health and lifestyle.
In general, healthy eating will
involve a variety of all food groups in proportions that are relevant to your
patient.
The food groups are:
Vegetables & fruit
Starchy carbohydrates
Protein foods
Dairy foods & alternatives
Fats & oils.
Calories (kcal)
Calories or kilocalories (kcal)
are a measurement of the amount of energy in our food and drinks.
The energy balance equation
states that if we take in more energy than we use, we will store this energy in
our body tissues, and gain weight.
Therefore, kcals and kcal
reduction have become a useful tools in weight management.
There are many different equations
that can be used to estimate someone’s energy expenditure.
In practice, I have not found
these easy to use.
A patient’s weight, and the trend
of their weight is a good indicator of their kcal requirements.
Practical kcal
Reduction
Kcal counting apps (accurate portions are key)
Looking at the kcal content of
foods such as on food labelling
Meal replacement products
Portion control
Plate models.
Partial Meal
Replacement Diets:
Uses meal replacement products to
replace 1-2 meals per day to create a calorie deficit.
Meal replacement products:
shakes, bar, soups and smoothies.
Each meal replacement typically
contains between 200-230 kcal/serving, 15g protein and vitamins and minerals.
These can be used safely outside
of Specialist Weight Management Services.
Meal Replacement
Products
I.e. slimfast
Very Low Calorie
Diets (VLCDs)
VLCDs are:
Any diet providing 800 kcal/day
or less.
Can be liquid diets (total meal
replacements) or fixed meal plans.
NICE advise that these should not
be used for longer than 12 weeks.
These should not be used in Tier
1 & 2 except under guidance from a GP or Consultant Physician.
VLCDs have been shown in some
cases to put type 2 diabetes into remission, up to 10 years after diagnosis.
Where remission is not achieved,
often an improvement in HbA1c is achieved. Also reduction in medication.
VLCDs are very restrictive and
can be difficult.
A specific VLCD plan should be
followed.
The Problem with kcal
& Low Fat
Research shows that most people
who go on a kcal controlled diet, lose weight over a 3-6 month period. Weight
loss then plateaus, and often weight is regained.
Low fat dietary advice has been
around for approximately 50 years. Low fat diets usually have a high proportion
of kcal from carbohydrate.
Poor outcomes in the general
population.
Lower Carbohydrate
Diets
These involve the reduction in
the consumption of starchy carbohydrates and sugars.
Can be successful in weight loss
and improving HbA1c.
Often higher in protein &
sometimes fat.
Often more satiating than other
dietary interventions.
Success may be due to the need
for the body to produce less insulin.
There is a spectrum of low
carbohydrate diets
Diabetes UK plan
100g or less per day of carbohydrate
Ketogenic or “keto” diets (20g or less).
Some practical difficulties in
achieving a lower carbohydrate long-term.
Other Interventions
Intermittent fasting
Time restricted eating
Lower glycaemic index (GI) diets
Weight loss/diabetes medications:
·
Orlistat
·
GLP-1 analogues
·
Saxenda (liraglutide)
·
SGLT2 inhibitors.

Meal replacement products
Either as an ad-hoc tool, or as
part of a partial meal replacement diet.
Investigate new dietary
interventions and fads when patients mention them.
Some may be useful, some may be
unhealthy.
Meet the patient where they
are.in terms of their weight loss
Be flexible, there are many ways
to lose weight in a healthy way
Be non-judgemental to encourage
patients to talk about their weight issues
Gently but firmly correct any
misunderstandings a patient may have.
Lifestyle Preparation For
Bariatric Surgery
23 December 2020
16:01
Prerequisites for Bariatric Surgery
Engage well with a Tier 3 Specialist Weight Management Service for 12
months.
Lose 10% of excess body weight during this time.
Must be a non-smoker. Some nicotine replacement therapies will also need
to have ceased prior to surgery.
Must be assessed for Obstructive Sleep Apnoea and, if diagnosed, be
compliant with the appropriate treatment.
Checklist:
I eat 3 regular meals (breakfast, lunch and evening meal).
I eat my regular meals at about the same time every day.
My portion sizes have decreased.
I eat 5 portions of fruit and vegetables a day.
I have reduced the amount of fat in my diet by limiting/avoiding fried
foods, choosing reduced or low fat options and now only eating lean cuts of
meat.
I have 3 portions of dairy foods or fortified alternatives in my diet
every day and choose reduced fat versions.
One portion can be:
200 ml semi-skimmed/skimmed milk
125-150g yoghurt (lower calorie)
30g reduced fat hard cheese
60g reduced fat soft cheese
100g low fat cottage cheese.
I no longer have fizzy drinks.
I aim to drink 2 litres of low calorie fluid per day (water, no added
sugar drinks e.g. tea, coffee, squash, flavoured water).
I avoid drinking 30 minutes before, after and during eating and I am now
sipping drinks throughout the day.
I do not drink alcohol Or I drink alcohol in moderation and do not
exceed the recommendation of 14 units per week over 3 or more days.
I rarely eat sugary foods and can now limit myself to 1 biscuit or 2
squares of chocolate.
I no longer eat takeaways.
I take at least 20 minutes to eat a meal.
I chew each mouthful of food 20 times before swallowing and I wait 20
seconds between each mouthful.
I do not binge eat.
I do not graze on foods.
I do not comfort eat.
Dumping Syndrome
·
This is an unpleasant
collection of symptoms that can occur post-bariatric surgery.
·
These symptoms can
include: sweating, faintness, palpitations, diarrhoea, nausea (feeling sickly)
and a bloated stomach.
·
Avoiding sugary and
fatty foods and drinks.
·
Avoiding drinking 30
mins, before and after and during eating.
·
Eating slowly and
chewing food well.
Bariatric Surgery /
Metabolic Surgery
23 December 2020
16:09
NHS Tier 4 weight management

Types:
Restrictive
·
Laparoscopic adjustable gastric band
o
*Restrictive procedure
*Inflatable band *Can be adjusted
via a reservoir under the skin
·
Vertical sleeve gastrectomy
o
*Restrictive Procedure
*Part of stomach is removed *Rest
of the stomach left as a sleeve
Malabsorptive
·
Roux-Y-Gastric Bypass (RYGB)
*Mal-absorptive procedure: *A small pouch is made in the stomach
*A loop of the bowel is anastomosed
into small bowel
·
Single anastomosis Mini bypass
·
Biliary Pancreatic Diversion-Duodenal Switch (BPD-DS)
Who is considered for bariatric
surgery:
People with BMI Of >40 without
co-morbidities
People with BMI of >35 with
co-morbidities
Before:
Work with a structured weight
management program for 6 months to 1 year
Make sustainable life style
changes
Confirm no major mental health
problems
Stop smoking
Co-morbidities optimised
Patient keen and motivated
Prepared for a long term life
style change
Bariatric surgery achieves
remission of type 2 Diabetes:
Studies have shown bariatric
surgery results in remission of Type 2 Diabetes-Defined as HbA1c <48 without
medications for more than a year
Benefits:
Improved mobility
Hypertension improved
Sleep apnoea resolved
Quality of life improved
Mental health benefits
Improved financial and social
health
Complications:
Peri-operative
complications
Infection, Bleeding, anaesthetic
complications
Long term
Nutritional deficiencies
Loose skin
Dumping syndrome
Summary:
Indications for bariatric surgery
Life style change is vital
Careful assessment of patients to
assess suitability for bariatric surgery
Benefits include significant
weight loss and improved co-morbidities
Helps to achieve remission of
Type 2 Diabetes
Plays a major role in treating
people with morbid obesity
Weight loss after:



Impaired Glucose Tolerance
23 December 2020
16:20
Diagnostic Criteria
(from IDF Atlas 9th edn 2019)

Bimodal distributions- DIabetes



Impaired Glucose
Tolerance
Global prevalence 2019 (age
adjusted) in 20-79 yr old adults 8.6%
Projected to rise in 2045 to
9.5%
Prevalence nationally in UK in
2011 10.7 %
Prevalence in Malaysia in 2019
15.5 %
25 – 75 % of people with IGT will
go on to develop Type 2 diabetes
Incidence of around 5 % per annum
Linked to increased
cardiovascular risk (RR 1.2 for IGT & IFG)

Evidence that intervention can
prevent development of T2DM
Diet and exercise
with modest weight loss ± Metformin was effective in the Diabetes Prevention
Programme in the USA
NICE PH 38 Prevention of Type 2
Diabetes www.nice.org.uk/guidance/ph38/chapter/Glossary
NHS England has a National
Diabetes Prevention Programme – recruited
> 380,000 by March 2019
At least 13 sessions over 9
months with health care professionals
If Lifestyle changes alone
ineffective then trial of metformin or acarbose
Address all other CV Disease risk
factors
·
Blood pressure
·
Plasma cholesterol
·
Smoking
·
Alcohol
Types of Diabetes
23 December 2020
16:39
Definition:
A net deficiency of insulin leading to imbalance in
glucose production and utilization
·
·
·
Fasting plasma glucose
≥7.0 mmol/L and 2h plasma glucose ≥11.1 mmol/L
Or
·
HbA1c >48
mmol/mol
Or
·
Random plasma glucose
≥ 11.1 mmol/L PLUS symptoms (thirst, polyuria,weight loss)
From <https://mle.ncl.ac.uk/cases/page/16226/>
Best non pharmacological treatment
Weight loss, DASH (Dietary Approaches to Stop Hypertension) diet,
Increase potassium intake, Decrease sodium intake, Decrease alcohol
consumption, Regular exercise, Increase dietary fibre.
In 2013, over 3.2
million adults were diagnosed with diabetes, with prevalence rates of 6% and
6.7% in England and Wales respectively. It is estimated that about 90% of
adults currently diagnosed with diabetes have type 2 diabetes. Type 2 diabetes
is more common in people of African, African‑Caribbean and South
Asian family origin. It can occur in all age groups and is increasingly being
diagnosed in children and adolescents almost always in association with obesity


·
Global prevalence 2019 (age adjusted) in 20-79 yr old
adults 8.3%
·
Projected to rise in 2045 to 9.6%
·
Prevalence on Teesside around 7.0 %
·
Prevalence nationally UK around 6.5 %
·
Prevalence in 65-99 year olds around 20.1 %
·
Prevalence in Malaysia in 20 – 79 year olds > 16.0
%

·
Acute complications - metabolic comas
o
DKA accounts for > 50% deaths in people
with diabetes in the USA aged < 24yrs
o
DKA listed as main cause of death in 25%
of those aged < 50 yrs in Scotland
·
Chronic complications - microvascular and
macrovascular
o
Diabetes commonest cause of end stage
renal disease globally
o
Incidence rates in Malaysia amongst
highest in world
o
Over 20% of UK dialysis population have
diabetes
o
Diabetes commonest cause of visual loss
globally
o
Diabetes commonest cause of non traumatic
amputation
o
Diabetes doubles cardiovascular disease
risk
o
Diabetes causes major pregnancy
complications
Diabetes Mellitus – Type 1
·
Type 1 diabetes rare in Malaysia
·
UK incidence ~ 10 - 20 / 100,000 children
·
Usually occurs < 40 years of age
·
Peak incidence adolescence but getting
younger
·
Strong genetic and auto immune basis
·
Always requires
·
Autoantibodies :
o
Glutamic acid decarboxylase (GAD 65)
o
Islet cells (not specific or sensitive)
o
Insulin
o
Tyrosine phosphatases (IA2 & IA2b)
o
Zinc transporter (ZnT8)
o
> 80% positive for GAD, IA2 or ZnT8 or
all three
·
Genetics – HLA :
o
>90% have DR4, DQB*0302 and/or DR3,
DQB*0201
o
Over 20 other genes identified with small
effects
·
insulin therapy
Latent Autoimmune Diabetes in Adults -
LADA
·
Up to 10% adults in Scandinavia have autoantibodies to
b cell antigens
·
Share genetic features with Type 1 (HLA) and Type 2
(TCF7L2)
·
Variable phenotype
·
Many develop insulin dependence
Diabetes Mellitus – Type 2
·
Type 2 diabetes represent at least 95% of
all cases
·
Incidence difficult to estimate
·
Prevalence varies with age, weight and
race
·
Usually occurs > 40 yrs of age;
becoming more common in young
·
Polygenic up to 50 genes with small
effects (TCF7L2 most powerful)
·
Usually not insulin dependent but often
becomes insulin requiring
Diabetes Mellitus – Other Types
Secondary –
due to pancreatic disease e.g. pancreatitis (acute, chronic and
calcific)
Cystic fibrosis - now more common with increased survival
Haemachromatosis due to iron deposition
Drug induced e.g. chronic steroid use, calcineurin inhibitors, statins,
major anti-psychotic agents, HAART
Monogenic – Maturity Onset Diabetes of the Young (MODY) (1-4% young adults with diabetes in UK). 37% glucokinase mutations; 63%
transcription factors
Early onset non-insulin dependent diabetes before the age 25 yrs
Monogenic: autosomal dominance
rare (1-3% of Type 2 diabetes)
Different genes, including HNFA1 and GCK
Congenital & neonatal
Syndromic e.g. lipodystrophies, Prader-Willi syndrome, myotonic
dystrophy, Wolfram (DIDMOAD)
Chromosomal e.g. Down and Turner syndrome increased Type 1 diabetes
Mitochondrial – maternal inheritance with deafness and cardio-neural
problems ( around 1% of those with Type 2 diabetes in Japan)
Associated Endocrinopathies
·
Excess hormones associated with diabetes
o
Cushing’s including iatrogenic -
Glucocorticoids
o Acromegaly – Growth Hormone
o Phaeochromocytoma – Catecholamines
o
Glucagonomas
o
Somatostatinomas
o
Hyperthyroidism (NB autoimmune link with
Type 1)
·
Summary:
·
Diabetes is common and getting commoner
·
Diabetes is associated with significant
morbidity and mortality
·
Not all diabetes is type 1 or type 2 -
Consider rare but treatable causes
·
MODY is an important diagnosis (in UK)
·
it can alter treatment & prognosis
·
Understanding unusual causes of DM helps :
·
understand pancreatic beta cell function
·
understand pathophysiology of all types of
DM
Personalised Medicine
23 December 2020
17:16
WHO Classification of Diabetes
(2019)
Type 1
Insulin-dependent
Autoimmune destruction of
B-cells
Characterised by ketones and weight loss
Type 2
Non-insulin dependent
Both decreased insulin secretion and insulin resistance
Hybrid forms
Slowly evolving immune mediated (LADA)
Maturity Onset
Diabetes of the Young: MODY
Early onset non-insulin dependent
diabetes before the age 25 yrs
Monogenic: autosomal dominance
rare (1-3% of Type 2 diabetes)
Different genes, including HNFA1
and GCK

Personalised Medicine:
“ An approach for disease
treatment and prevention that takes into account individual variability in
environment, lifestyle and genes for each person”




Remission of Type 2
Diabetes
23 December 2020
17:57


As duration goes up its harder to
put T2DM into remission

Diet for weight loss:
Simple
Practical
Spouse/partner on board
Duration limited and planned- 8
weeks max 12 weeks
No additional exercise during
this time
Compensatory eating renders
exercise counterproductive during weight loss
Protein mainly- satiety


Lipid and Health
23 December 2020
18:17
Why should we know
about lipids?
Abnormal lipid values are highly
prevalent
Well documented relationship
between total and LDL-C levels and vascular events like coronary artery
disease, cerebrovascular disease and peripheral vascular disease
Treatment decreases the risk
of events
Early knowledge of a lipid
disorder creates the best opportunity for early intervention
Prevalence:
About 50% of adults have an
elevated total cholesterol level
Majority of patients with
atherosclerosis have some form of dyslipidemia
70-80% of individuals with
dyslipidemia do not meet LDL cholesterol targets despite lipid therapy
Symptoms:
High cholesterol does not cause
any symptoms
Too much cholesterol may lead to
a build up of plaque inside the arteries causing atherosclerosis


Measure:
Total Cholesterol (Desirable
<5 mmol / l)
Low density Lipoproteins (LDL)
(Desirable <2.5 mmol / l)
High Density lipoproteins (HDL)
(Desirable > 1.2 in women and > 1 in men)
Triglycerides (Desirable < 2.5
mmol / l)
Total cholesterol/ HDL Ratio
(Desirable < 4 )
Others: Very low density
lipoproteins (VLDL), Lipoprotein A, Apolipoproteins
Total Cholesterol:
Total cholesterol measures the
combination of LDL, HDL, and VLDL (very low density lipoprotein) in your
bloodstream. VLDL is a precursor of LDL, the bad cholesterol.
A total cholesterol of under 5 is considered
healthy in most cases.
LDL:
Most of the cholesterol in the
blood is carried by proteins called low density lipoproteins or LDL or the bad cholesterol
LDL combines with other
substances to clog the arteries.
A diet high in saturated fats and
trans fats tends to raise the level of LDL cholesterol.
For most people, an LDL score
below 2.5 is healthy, but people with heart disease may need to aim even lower
HDL:
Up to a third of blood
cholesterol is carried by high-density lipoproteins or HDL or the good
cholesterol
HDL helps remove bad cholesterol,
preventing it from building up inside the arteries.
The higher the level of HDL
cholesterol, the better. People with too little are more likely to develop
heart disease.
Triglyceride:
The body converts excess
calories, sugar, and alcohol into triglycerides, a type of fat that is carried
in the blood and stored in fat cells throughout the body.
People who are overweight,
inactive, smokers, or heavy drinkers and those who eat a very high carbohydrate
diet tend to have high triglycerides
High triglycerides puts people at risk for
metabolic syndrome, which is linked to heart disease and diabetes.
Causes:
Primary Dyslipidaemia
·
Genetic dyslipidaemia
·
Familial Hypercholsterolaemia
Secondary
·
Type 2 Diabetes
·
Nephrotic syndrome
·
Hypothyroidism
·
Obesity, smoking, life style
What increases risk:
A diet high in saturated fats and
cholesterol
A family history of high
cholesterol
Being overweight or obese
Getting older
Secondary causes like Diabetes
Physical inactivity, smoking,
alcohol will increase triglyceride level
Ways to lower:
Many National and International
guidelines are in place
European Society of cardiology
guidelines
NICE UK guidelines
Dietary
Modifications:
Saturated fats - from animal
products and tropical oils -- raise LDL cholesterol
Trans fats increase bad
cholesterol and lowers the good cholesterol
These two bad fats are found in
many baked goods, fried foods (doughnuts, french fries, chips), stick
margarine, and cookies
Unsaturated fats may lower LDL
when combined with other healthy diet changes. They're found in avocados, olive
oil, and peanut oil.
Moderate alcohol intake
Lifestyle
Modifications:
Lose weight
Stop smoking
Increase physical activity
Medications/Drugs:
Statins
Fibrates, Ezetimibe, Omega 3
fatty acids
Bile acid sequestrants
PCSK 9 inhibitors, Inclisiron
Statins:
Lipid soluble
Atorvastatin
Simvastatin
Water soluble
Rosuvastatin
Pravastatin
Decrease LDL by 18 – 55 %
Increase HDL by 5 – 15 %
Decrease TG by 7 – 30 %

Genetic dyslipideamia
23 December 2020
18:32
Familial hypercholesterolaemia


Familial Hypercholesterolemia:
Prevalence estimayed : 1 in 200
to 1 in 250 people
Most common inherited condition
Autosomal Dominant inheritance

When to suspect:
High LDL > 5 mmol/l
Early Cardio vascular event
Strong family history
Stigmata
Tendon xanthoma
Arcus Lipidalis
Dutch lipid scoring system:

Confirmatory test:
Gene sequencing
Once confirmed-Family members are
screened- family cascading
Simon Broom Criteria:

Management:
Life style modification
Family cascading
Statins
Ezetimibe
PCSK-9 inhibitors
·
Alirocumab
·
Evolucumab
Inclisiron
Essential Hypertension
23 December 2020
18:48
Normal Blood Pressure:
Blood pressure not normally distributed in population
Marked variation by age- higher the higher, higher distribution in
elderly
Long tail of values to the right, especially in elderly
Abnormal defined largely by response to blood pressure lowering
Essential Hypertension:
Defined as ‘hypertension with no known cause’
Accounts for > 95% of cases (secondary causes separate resource)
Divided into stages
Stage 1 BP 140-159/90-99 mmHg clinic (135-149/85-94 mmHg average
ABPM/HBPM)
Stage 2 BP 160-179/100-119 mmHg (≥ 150/95 ≤180/120 mmHg average
ABPM/HBPM)
Stage 3 (severe) BP ≥ 180/120 mmHg
66% of patients with hypertension have a comorbidity

Recommended practice for measuring blood pressure adapted from
International Society of Hypertension
Use a calibrated and validated instrument
Quiet room
No smoking, exercise or caffeine for 30 mins
Measure after 5 minutes in a seated position, feet on floor
Arm should be free of tight clothing and at heart level
Cuff bladder should cover >80% of arm circumference
Take 3 measurements, 1 min apart and average last 2
Check both arms (always use the arm with higher reading)
Check standing blood pressure to detect drug-induced postural
hypotension


Age Related Prevalence of Hypertension in England in 2014




WHO Priority Actions:
Public Health Initiatives e.g. alcohol and weight reduction; dietary
salt
Integrated Programmes to treat hypertension and other NCDs (diabetes,
atherosclerotic cardiovascular disease)
Education & Encouragement of populations to get tested and treated
(In UK 35% identified and treated to target; 65% in Canada)
Promote Workplace Wellness Programmes e.g. smoking restriction, healthy
food options
Assessment and investigation of the patient with hypertension :
(from NICE NG136 Hypertension in adults:diagnosis and management)
·
Measurement of height
and weight (for BMI) or waist circumference
·
Examination of the:
·
heart for evidence of
left ventricular hypertrophy
·
lungs for heart failure
·
abdomen for pulsatile
masses, renal enlargement or bruits
·
fundi for signs of
retinopathy
·
Auscultation for carotid
and femoral arterial bruits
·
Examination of
peripheral pulses (to exclude coarctation or peripheral vascular disease)
·
Investigations to
include ECG, urinalysis (including for microalbuminuria), serum electrolytes,
urea and creatinine (and calculation of eGFR), HbA1c, fasting blood
lipid profile, chest X-ray or echocardiogram to confirm left ventricular
hypertrophy if suspected from ECG
·
Consider referral for
specialist opinion in those with signs or symptoms of possible secondary causes
of hypertension.


Secondary Hypertension
23 December 2020
18:53




Life style and Cancer
23 December 2020
18:59
What is classed as life style
Diet
Physical activity
Smoking
Alcohol
Poor diet and reduced physical
activity causes obesity
Obesity is associated with Cancer
Type of Cancer and risk of death
in Obesity-Men

Type of Cancer and risk of death
in Obesity- Women


Smoking : Carcinogens to Humans
Group 1 : Definite
·
Tobacco Smoking
·
Tobacco Products, Smokeless
·
4-Aminobiphenyl (4-ABP)
·
Benzene
·
Carmium
·
Chromium
·
2-Naphthylamine (2-NA)
·
Nickel
·
Polonium-210 (Radon)
·
Vinyl Chloride
Group 2: Probable
·
Acrylonitrile
·
Benzo[a]pyrene
·
Benzo[a]anthracene
·
1,3-Butadiene
·
Dibenz(a,h)anthracene
·
Formaldehyde
·
N-Nitrosodiethylamine
·
N-Nitrosodimethylamine
Overall, 86% of cases in men and
49% in women are due to smoking.
Stop smoking apps:
Kwit
QuitNow! Quit smoking
Quit Vaping
SmokeFree
Unsmok'd
|
Type of beverage |
ABV (w/w in %) |
|
beer, cider, and Perry |
4-6 |
|
wine |
9-13 |
|
spirits (e.g. brandy, gin, rum, vodka,
whisky) made by distilling fermented liquor |
38-45 |
|
liqueurs made from distilled spirits,
sweetened and flavored |
20-40 |
|
fortified wines (aperitif wines,
Madeira, port, sherry) made by adding spirit to wine |
18-25 |

Alcohol cancers: 7
Oral and pharyngeal cancer
Esophageal cancer
Stomach cancer
Liver cancer
Colorectal cancer
Lung cancer
Breast cancer


BMI
04 January 2021
21:23


24 December 2020
14:11
Wilson's disease
Wilson's disease is an autosomal recessive disorder characterised by excessive copper deposition in the
tissues. Metabolic abnormalities include increased copper absorption from the
small intestine and decreased hepatic copper excretion. Wilson's disease is
caused by a defect in the ATP7B gene located on chromosome
13.
The onset of symptoms is usually
between 10 - 25 years. Children usually present with liver disease whereas the
first sign of disease in young adults is often neurological disease
Features result from
excessive copper deposition in the tissues, especially the brain, liver and
cornea:
·
liver: hepatitis, cirrhosis
·
neurological:
o basal ganglia degeneration: in the
brain, most copper is deposited in the basal ganglia, particularly in the
putamen and globus pallidus
o speech, behavioural and psychiatric problems are often the first manifestations
o also: asterixis, chorea, dementia, parkinsonism
·
Kayser-Fleischer rings
o green-brown rings in the periphery
of the iris
o due to copper accumulation in
Descemet membrane
o present in around 50% of patients
with isolated hepatic Wilson's disease and 90% who have neurological
involvement
·
renal tubular acidosis (esp. Fanconi syndrome)
·
haemolysis
·
blue nails
Diagnosis
·
slit lamp examination for Kayser-Fleischer rings
·
reduced serum caeruloplasmin
·
reduced total serum copper (counter-intuitive, but 95% of
plasma copper is carried by ceruloplasmin)
o free (non-ceruloplasmin-bound)
serum copper is increased
·
increased 24hr urinary copper excretion
Management
·
penicillamine (chelates copper) has been the
traditional first-line treatment
·
trientine hydrochloride is an alternative chelating agent which
may become first-line treatment in the future
·
tetrathiomolybdate is a newer agent that is currently under
investigation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Primary sclerosing cholangitis
Primary sclerosing cholangitis is a
biliary disease of unknown aetiology characterised by inflammation and fibrosis
of intra and extra-hepatic bile ducts.
Associations
·
ulcerative colitis: 4% of patients with UC have PSC, 80% of patients with PSC have UC
·
Crohn's (much less common association than UC)
·
HIV
Features
·
cholestasis
o jaundice, pruritus
o raised bilirubin + ALP
·
right upper quadrant pain
·
fatigue
Investigation
·
endoscopic retrograde
cholangiopancreatography (ERCP) or magnetic resonance cholangiopancreatography
(MRCP) are the standard diagnostic investigations, showing multiple biliary strictures giving a 'beaded' appearance
·
p-ANCA
may be positive
·
there
is a limited role for liver biopsy, which may show fibrous, obliterative
cholangitis often described as 'onion skin'
Complications
·
cholangiocarcinoma (in
10%)
·
increased
risk of colorectal cancer
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Variceal haemorrhage
Acute treatment of variceal
haemorrhage
·
ABC: patients should ideally be resuscitated prior to endoscopy
·
correct clotting: FFP, vitamin K
·
vasoactive agents:
o terlipressin is currently the
only licensed vasoactive agent and is supported by NICE guidelines. It has been
shown to be of benefit in initial haemostasis and preventing rebleeding
o octreotide may also be used
although there is some evidence that terlipressin has a greater effect on
reducing mortality
·
prophylactic antibiotics have been shown to reduce mortality
in patients with liver cirrhosis. Quinolones are typically used. NICE support
this in their 2016 guidelines: 'Offer prophylactic intravenous
antibiotics for people with cirrhosis who have upper gastrointestinal bleeding.'
·
endoscopy: endoscopic variceal band ligation is superior to
endoscopic sclerotherapy. NICE recommend band ligation
·
Sengstaken-Blakemore tube if uncontrolled haemorrhage
·
Transjugular Intrahepatic Portosystemic Shunt (TIPSS) if above
measures fail
o connects the hepatic vein to the
portal vein
o exacerbation of hepatic
encephalopathy is a common complication
Prophylaxis of variceal haemorrhage
·
propranolol: reduced rebleeding and mortality compared to placebo
·
endoscopic variceal band ligation (EVL) is superior to
endoscopic sclerotherapy. It should be performed at two-weekly intervals until
all varices have been eradicated. Proton pump inhibitor cover is given to
prevent EVL-induced ulceration. This is supported by NICE who recommend: 'Offer endoscopic variceal band ligation for the primary prevention of
bleeding for people with cirrhosis who have medium to large oesophageal
varices.'
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Ischaemia to the lower gastrointestinal tract
Ischaemia to the lower
gastrointestinal tract can result in a variety of clinical conditions. Whilst
there is no standard classification it can be useful to separate cases into 3
main conditions
·
acute mesenteric ischaemia
·
chronic mesenteric ischaemia
·
ischaemic colitis
|
|
|
|
|
|

Venn diagram showing types of bowel ischaemia
Common features in bowel ischaemia
Common predisposing factors
·
increasing age
·
atrial fibrillation - particularly for mesenteric ischaemia
·
other causes of emboli: endocarditis, malignancy
·
cardiovascular disease risk factors: smoking, hypertension,
diabetes
·
cocaine: ischaemic colitis is sometimes seen in young patients
following cocaine use
Common features
·
abdominal pain - in acute mesenteric ischaemia this is often of
sudden onset, severe and out-of-keeping with physical exam findings
·
rectal bleeding
·
diarrhoea
·
fever
·
bloods typically show an elevated white blood cell count
associated with a lactic acidosis
Diagnosis
·
CT is the investigation of choice
Acute mesenteric ischaemia
Acute mesenteric ischaemia is
typically caused by an embolism resulting in occlusion of an artery which
supplies the small bowel, for example the superior mesenteric artery.
Classically patients have a history of atrial fibrillation.
The abdominal pain is typically
severe, of sudden onset and out-of-keeping with physical exam findings.
Management
·
urgent surgery is usually required
·
poor prognosis, especially if surgery delayed
Chronic
mesenteric ischaemia
Chronic mesenteric ischaemia is a
relatively rare clinical diagnosis due to it's non-specific features and may be
thought of as 'intestinal angina'. Colickly, intermittent abdominal pain
occurs.
Ischaemiac colitis
Ischaemic colitis describes an
acute but transient compromise in the blood flow to the large bowel. This may
lead to inflammation, ulceration and haemorrhage. It is more likely to occur in
'watershed' areas such as the splenic flexure that are
located at the borders of the territory supplied by the superior and inferior
mesenteric arteries.
Investigations
·
'thumbprinting' may be seen on abdominal x-ray due to mucosal
oedema/haemorrhage
Management
- usually supportive
- surgery may be required in a
minority of cases if conservative measures fail. Indications would include
generalised peritonitis, perforation or ongoing haemorrhage
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Alcoholic liver disease
Alcoholic liver disease covers a
spectrum of conditions:
·
alcoholic fatty liver disease
·
alcoholic hepatitis
·
cirrhosis
Selected investigation findings:
·
gamma-GT is characteristically elevated
·
the ratio of AST:ALT is normally > 2, a ratio of > 3 is strongly
suggestive of acute alcoholic hepatitis
Selected management notes for
alcoholic hepatitis:
·
glucocorticoids (e.g. prednisolone) are often used
during acute episodes of alcoholic hepatitis
o Maddrey's discriminant function
(DF) is often used during acute episodes to determine who
would benefit from glucocorticoid therapy
o it is calculated by a formula using prothrombin time and bilirubin concentration
·
pentoxyphylline is also sometimes used
o the STOPAH study (see reference)
compared the two common treatments for alcoholic hepatitis, pentoxyphylline and
prednisolone. It showed that prednisolone improved survival at 28 days and that
pentoxyphylline did not improve outcomes
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Dysphagia
The table below gives
characteristic exam question features for conditions causing dysphagia.
Remember that new-onset dysphagia is a red flag symptom that requires urgent
endoscopy, regardless of age or other symptoms.
|
Causes |
Notes |
|
Oesophageal cancer |
Dysphagia may be associated with weight
loss, anorexia or vomiting during eating Past history may include Barrett's
oesophagus, GORD, excessive smoking or alcohol use |
|
Oesophagitis |
There may be a history of heartburn Odynophagia but no weight loss and
systemically well |
|
Oesophageal candidiasis |
There may be a history of HIV or other
risk factors such as steroid inhaler use |
|
Achalasia |
Dysphagia of both liquids and
solids from the start Heartburn Regurgitation of food - may lead to
cough, aspiration pneumonia etc |
|
Pharyngeal pouch |
More common in older men Represents a posteromedial herniation
between thyropharyngeus and cricopharyngeus muscles Usually not seen but if large then a
midline lump in the neck that gurgles on palpation Typical symptoms are dysphagia,
regurgitation, aspiration and chronic cough. Halitosis may occasionally be
seen |
|
Systemic sclerosis |
Other features of CREST syndrome may be
present, namely Calcinosis, Raynaud's phenomenon, oEsophageal dysmotility,
Sclerodactyly, Telangiectasia As well as oesophageal dysmotility the
lower oesophageal sphincter (LES) pressure is decreased. This contrasts to
achalasia where the LES pressure is increased |
|
Myasthenia gravis |
Other symptoms may include extraocular
muscle weakness or ptosis Dysphagia with liquids as well as
solids |
|
Globus hystericus |
There may be a history of anxiety Symptoms are often intermittent and
relieved by swallowing Usually painless - the presence of pain
should warrant further investigation for organic causes |
Causes of dysphagia - by
classification
As with many conditions, it's often
useful to think about causes of a symptom in a structured way:
|
Classification |
Examples |
|
Extrinsic |
·
Mediastinal masses ·
Cervical spondylosis |
|
Oesophageal wall |
·
Achalasia ·
Diffuse oesophageal spasm ·
Hypertensive lower oesophageal sphincter |
|
Intrinsic |
·
Tumours ·
Strictures ·
Oesophageal web ·
Schatzki rings |
|
Neurological |
·
CVA ·
Parkinson's disease ·
Multiple Sclerosis ·
Brainstem pathology ·
Myasthenia Gravis |
Investigation
All patients require an upper GI
endoscopy unless there are compelling reasons for this not to be performed.
Motility disorders may be best appreciated by undertaking fluoroscopic
swallowing studies.
A full blood count should be
performed.
Ambulatory oesophageal pH and
manometry studies will be required to evaluate conditions such as achalasia and
patients with GORD being considered for fundoplication surgery.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Clostridium difficile
Clostridium difficile is a Gram positive rod often encountered in hospital practice. It produces an exotoxin
which causes intestinal damage leading to a syndrome called pseudomembranous
colitis. Clostridium
difficile develops when the normal gut flora
are suppressed by broad-spectrum antibiotics. Clindamycin is historically associated with causing Clostridium difficile but the aetiology has evolved significantly over the past 10
years. Second and third generation cephalosporins are now the leading cause of Clostridium difficile.
Other than antibiotics, risk
factors include:
·
proton pump inhibitors
Features
·
diarrhoea
·
abdominal pain
·
a raised white blood cell count
(WCC) is characteristic
·
if severe toxic megacolon may develop
The Public Health England severity
scale is often used as this may determine treatment:
|
Mild |
Moderate |
Severe |
life-threatening |
|
Normal WCC |
↑ WCC ( < 15 x 109/L) Typically 3-5 loose stools per day |
↑ WCC ( > 15 x 109/L) or an acutely ↑ creatinine (> 50%
above baseline) or a temperature > 38.5°C or evidence of severe colitis(abdominal
or radiological signs) |
Hypotension Partial or complete ileus Toxic megacolon, or CT evidence of
severe disease |
Diagnosis
·
is made by detecting Clostridium difficile toxin (CDT) in the stool
·
Clostridium difficile antigen positivity
only shows exposure to the bacteria, rather than current infection
Management
·
first-line therapy is oral
metronidazole for 10-14 days
·
if severe or not responding to metronidazole
then oral vancomycin may be used
o recurrent infection occurs in
around 20% of patients, increasing to 50% after their second episode
·
fidaxomicin may also be used for patients who are not responding ,
particularly those with multiple co-morbidities
·
for life-threatening infections a combination of oral vancomycin and intravenous metronidazole should be used
Other therapies
·
bezlotoxumab is a monoclonal antibody which targets Clostridium
difficile toxin B - it is not in widespread use

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:12
Ulcerative colitis: management
Treatment can be divided into
inducing and maintaining remission. NICE updated their guidelines on the
management of ulcerative colitis in 2019.
The severity of UC is usually
classified as being mild, moderate or severe:
·
mild: < 4 stools/day, only a small amount of blood
·
moderate: 4-6 stools/day, varying amounts of blood, no systemic
upset
·
severe: >6 bloody stools per day + features of systemic upset
(pyrexia, tachycardia, anaemia, raised inflammatory markers)
Inducing remission
Treating mild-to-moderate
ulcerative colitis
·
proctitis
o topical (rectal) aminosalicylate:
for distal colitis rectal mesalazine has been shown to be superior to rectal
steroids and oral aminosalicylates
o if remission is not achieved within 4 weeks, add an oral aminosalicylate
o if remission still not achieved add
topical or oral corticosteroid
·
proctosigmoiditis and left-sided ulcerative colitis
o topical (rectal) aminosalicylate
o if remission is not achieved within
4 weeks, add a high-dose oral
aminosalicylate OR switch to a high-dose oral aminosalicylate and a topical
corticosteroid
o if remission still not achieved
stop topical treatments and offer an oral aminosalicylate and an oral corticosteroid
·
extensive disease
o topical (rectal)
aminosalicylate and a high-dose oral aminosalicylate:
o if remission is not achieved within
4 weeks, stop topical treatments and offer a high-dose oral aminosalicylate and
an oral corticosteroid
Severe colitis
·
should be treated in hospital
·
intravenous steroids are usually given first-line
o intravenous ciclosporin may be used
if steroid are contraindicated
·
if after 72 hours there has been no improvement, consider adding
intravenous ciclosporin to intravenous corticosteroids or consider surgery
Maintaining remission
Following a mild-to-moderate
ulcerative colitis flare
·
proctitis and proctosigmoiditis
o topical (rectal) aminosalicylate
alone (daily or intermittent) or
o an oral aminosalicylate plus a
topical (rectal) aminosalicylate (daily or intermittent) or
o an oral aminosalicylate by itself:
this may not be effective as the other two options
·
left-sided and extensive ulcerative colitis
o low maintenance dose of an oral
aminosalicylate
Following a severe relapse or
>=2 exacerbations in the past year
·
oral azathioprine or oral mercaptopurine
Other points
·
methotrexate is not recommended for the management of UC (in
contrast to Crohn's disease)
·
there is some evidence that probiotics may prevent relapse in
patients with mild to moderate disease
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Haemochromatosis: investigation and management
Haemochromatosis is an autosomal
recessive disorder of iron absorption and metabolism resulting in iron
accumulation. It is caused by inheritance of mutations in the HFE gene on both
copies of chromosome 6*.
There is continued debate about the
best investigation to screen for haemochromatosis.
·
general population: transferrin
saturation is considered the most useful marker. Ferritin should also be
measured but is not usually abnormal in the early stages of iron accumulation
·
testing family members: genetic testing for HFE
mutation
These guidelines may change as HFE
gene analysis become less expensive
Diagnostic tests
·
molecular genetic testing for the C282Y and H63D mutations
·
liver biopsy: Perl's stain
Typical iron study profile in patient with haemochromatosis
·
transferrin saturation > 55% in men or > 50% in women
·
raised ferritin (e.g. > 500 ug/l) and iron
·
low TIBC
Management
·
Venesection is the first-line treatment
o monitoring adequacy of venesection: transferrin saturation should be kept below 50% and the serum
ferritin concentration below 50 ug/l
·
desferrioxamine may be used second-line
Joint x-rays characteristically
show chondrocalcinosis
*there are rare cases of families
with classic features of genetic haemochromatosis but no mutation in the HFE
gene
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Oesophageal cancer
Until recent times oesophageal
cancer was most commonly due to a squamous cell carcinoma but the incidence of
adenocarcinoma is rising rapidly. Adenocarcinoma is now the most common type of
oesophageal cancer and is more likely to develop in patients with a history of gastro-oesophageal
reflux disease (GORD) or Barrett's.
The majority of adenocarcinomas are
located near the gastroesophageal junction whereas squamous cell tumours are
most commonly found in the upper two-thirds of the oesophagus.
|
|
Adenocarcinoma |
Squamous cell cancer |
|
Epidemiology |
Most common type in the UK/US |
Most common type in the developing
world |
|
Location |
Lower third - near the gastroesophageal
junction |
Upper two-thirds of the oesophagus |
|
Risk factors |
·
GORD ·
Barrett's oesophagus ·
smoking ·
achalasia ·
obesity |
·
smoking ·
alcohol ·
achalasia ·
Plummer-Vinson syndrome ·
diets rich in nitrosamines |
Features
·
dysphagia: the most common presenting symptom
·
anorexia and weight loss
·
vomiting
·
other possible features include: odynophagia, hoarseness, melaena, cough
Diagnosis
·
Upper GI endoscopy is the first line test
·
Contrast swallow may be of benefit in classifying benign
motility disorders but has no place in the assessment of tumours
·
Staging is initially undertaken with CT scanning of the chest,
abdomen and pelvis. If overt metastatic disease is identified using this
modality then further complex imaging is unnecessary
·
If CT does not show metastatic disease, then local stage may be
more accurately assessed by use of endoscopic ultrasound
·
Staging laparoscopy is performed to detect occult peritoneal
disease. PET CT is performed in those with negative laparoscopy. Thoracoscopy
is not routinely performed.
Treatment
·
Operable disease is best managed by surgical resection.
·
The most standard procedure is an Ivor- Lewis type
oesophagectomy. This procedure involves the mobilisation of the stomach and
division of the oesophageal hiatus. The abdomen is closed and a right-sided
thoracotomy performed. The stomach is brought into the chest and the oesophagus
mobilised further. An intrathoracic oesophagogastric anastomosis is
constructed. Alternative surgical strategies include a transhiatal resection
(for distal lesions), a left thoracoabdominal resection (difficult access due
to thoracic aorta) and a total oesophagectomy (McKeown) with a cervical
oesophagogastric anastomosis.
·
The biggest surgical challenge is that of anastomotic leak, with
an intrathoracic anastomosis this will result in mediastinitis. With high
mortality. The McKeown technique has an intrinsically lower systemic insult in
the event of anastomotic leakage.
·
In addition to surgical resection many patients will be treated
with adjuvant chemotherapy.


From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Pancreatic cancer
Pancreatic cancer is often
diagnosed late as it tends to present in a non-specific way. Over 80% of
pancreatic tumours are adenocarcinomas
which typically occur at the head of the pancreas.
Associations
·
increasing age
·
smoking
·
diabetes
·
chronic pancreatitis (alcohol does not appear an independent
risk factor though)
·
hereditary non-polyposis colorectal carcinoma
·
multiple endocrine neoplasia
·
BRCA2 gene
·
KRAS gene mutation
Features
·
classically painless jaundice
o pale stools, dark urine, and
pruritus
o cholestatic liver function tests
·
Courvoisier's law states that in the presence of
painless obstructive jaundice, a palpable gallbladder is unlikely to be due to
gallstones
·
however, patients typically present in a non-specific way with
anorexia, weight loss, epigastric pain
·
loss of exocrine function (e.g. steatorrhoea)
·
loss of endocrine function (e.g. diabetes
mellitus)
·
atypical back pain is often seen
·
migratory thrombophlebitis (Trousseau sign) is more common than
with other cancers
Investigation
·
ultrasound has a sensitivity of around 60-90%
·
high-resolution CT scanning is the investigation of choice if the diagnosis
is suspected
·
imaging may demonstrate the 'double
duct' sign - the presence of simultaneous dilatation of the common bile and
pancreatic ducts
Management
·
less than 20% are suitable for surgery at diagnosis
·
a Whipple's resection (pancreaticoduodenectomy) is performed for
resectable lesions in the head of pancreas. Side-effects of a Whipple's include
dumping syndrome and peptic ulcer disease
·
adjuvant chemotherapy is usually given following surgery
·
ERCP with stenting is often used for palliation
|
|
|
|
©
Image used on license from Radiopaedia |
|

ERCP showing invasive ductal adenocarcinoma. Note the
dilation of the common bile duct due to the pancreatic lesion
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Acute upper gastrointestinal bleeding
NICE published guidelines in 2012
on the management of acute upper gastrointestinal bleeding which is most
commonly due to either peptic ulcer disease or oesophageal varices. Some of the
key points are detailed below.
Risk assessment
·
use the Blatchford score at first assessment, and
·
the full Rockall score after endoscopy
Blatchford score
|
Admission
risk marker |
Score |
|
Urea (mmol/l) |
6·5 - 8 = 2 8 - 10 = 3 10 - 25 = 4 > 25 = 6 |
|
Haemoglobin (g/l) |
Men ·
12 - 13 = 1 ·
10 - 12 = 3 ·
< 10 = 6 Women ·
10 - 12 = 1 ·
< 10 = 6 |
|
Systolic blood pressure (mmHg) |
100 - 109 = 1 90 - 99 = 2 < 90 = 3 |
|
Other markers |
Pulse >=100/min = 1 Presentation with melaena = 1 Presentation with syncope = 2 Hepatic disease = 2 Cardiac failure = 2 |
Patients with a Blatchford score of
0 may be considered for early discharge.
Resuscitation
·
ABC, wide-bore intravenous access * 2
·
platelet transfusion if actively bleeding platelet count of less
than 50 x 10*9/litre
·
fresh frozen plasma to patients who have either a fibrinogen
level of less than 1 g/litre, or a prothrombin time (international normalised
ratio) or activated partial thromboplastin time greater than 1.5 times normal
·
prothrombin complex concentrate to patients who are taking
warfarin and actively bleeding
Endoscopy
·
should be offered immediately after resuscitation in patients
with a severe bleed
·
all patients should have endoscopy within 24 hours
Management of non-variceal bleeding
·
NICE do not recommend the use of proton pump inhibitors (PPIs)
before endoscopy to patients with suspected non-variceal upper
gastrointestinal bleeding although PPIs should be given to patients with
non-variceal upper gastrointestinal bleeding and stigmata of recent haemorrhage
shown at endoscopy
·
if further bleeding then options include repeat endoscopy,
interventional radiology and surgery
Management of variceal bleeding
·
terlipressin and prophylactic antibiotics should be given to
patients at presentation (i.e. before endoscopy)
·
band ligation should be used for oesophageal varices and
injections of N-butyl-2-cyanoacrylate for patients with gastric varices
·
transjugular intrahepatic portosystemic shunts (TIPS) should be
offered if bleeding from varices is not controlled with the above measures
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Carcinoid tumours
Carcinoid syndrome
·
usually occurs when metastases are present in the liver and
release serotonin into the systemic circulation
·
may also occur with lung carcinoid as mediators are not
'cleared' by the liver
Features
·
flushing (often earliest symptom)
·
diarrhoea
·
bronchospasm
·
hypotension
·
right heart valvular stenosis (left heart can be affected in
bronchial carcinoid)
·
other molecules such as ACTH and GHRH may also be secreted
resulting in, for example, Cushing's syndrome
·
pellagra can rarely develop as dietary tryptophan is diverted to
serotonin by the tumour
Investigation
·
urinary 5-HIAA
·
plasma chromogranin A y
Management
·
somatostatin analogues e.g. octreotide
·
diarrhoea: cyproheptadine may help
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Hepatitis B serology
Interpreting hepatitis B serology
is a dying art form which still occurs at regular intervals in medical exams.
It is important to remember a few key facts:
·
surface antigen (HBsAg) is the first marker to appear and causes
the production of anti-HBs
·
HBsAg normally implies acute disease (present for 1-6 months)
·
if HBsAg is present for > 6 months then this implies chronic disease (i.e. Infective)
·
Anti-HBs implies immunity (either exposure or immunisation). It
is negative in chronic disease
·
Anti-HBc implies previous (or current) infection. IgM anti-HBc
appears during acute or recent hepatitis B infection and is present for about 6
months. IgG anti-HBc persists
·
HbeAg results from breakdown of core antigen from infected liver
cells as is, therefore, a marker of infectivity
Example results
·
previous immunisation: anti-HBs positive, all others negative
·
previous hepatitis B (> 6 months ago), not a carrier:
anti-HBc positive, HBsAg negative
·
previous hepatitis B, now a carrier: anti-HBc positive, HBsAg
positive
HBsAg = ongoing infection, either acute or chronic if present > 6 months
anti-HBc = caught, i.e. negative if immunized
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Primary biliary cholangitis
Primary biliary cholangitis
(previously referred to as primary biliary cirrhosis) is a chronic liver
disorder typically seen in middle-aged
females (female:male ratio of 9:1). The aetiology is not fully
understood although it is thought to be an autoimmune condition. Interlobular
bile ducts become damaged by a chronic inflammatory process causing progressive
cholestasis which may eventually progress to cirrhosis. The classic
presentation is itching in a middle-aged woman
Associations
·
Sjogren's syndrome (seen in up to 80% of patients)
·
rheumatoid arthritis
·
systemic sclerosis
·
thyroid disease
Clinical features
·
early: may be asymptomatic (e.g. raised ALP on routine LFTs) or
fatigue, pruritus
·
cholestatic jaundice
·
hyperpigmentation, especially over pressure points
·
around 10% of patients have right upper quadrant pain
·
xanthelasmas, xanthomata
·
also: clubbing, hepatosplenomegaly
·
late: may progress to liver failure
Diagnosis
·
anti-mitochondrial antibodies (AMA) M2 subtype are present in
98% of patients and are highly specific
·
smooth muscle antibodies in 30% of patients
·
raised serum IgM
Management
·
first-line: ursodeoxycholic acid
o slows disease progression and
improves symptoms
·
pruritus: cholestyramine
·
fat-soluble vitamin supplementation
·
liver transplantation
o e.g. if bilirubin > 100 (PBC is
a major indication)
o recurrence in graft can occur but
is not usually a problem
Complications
·
cirrhosis → portal hypertension → ascites, variceal haemorrhage
·
osteomalacia and osteoporosis
·
significantly increased risk of hepatocellular carcinoma
(20-fold increased risk)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Autoimmune hepatitis
Autoimmune hepatitis is condition
of unknown aetiology which is most commonly seen in young females. Recognised
associations include other autoimmune disorders, hypergammaglobulinaemia and
HLA B8, DR3. Three types of autoimmune hepatitis have been characterised
according to the types of circulating antibodies present
|
Type
I |
Type II |
Type III |
|
Anti-nuclear antibodies (ANA) and/or
anti-smooth muscle antibodies (SMA) Affects both adults and children |
Anti-liver/kidney microsomal type 1
antibodies (LKM1) Affects children only |
Soluble liver-kidney antigen Affects adults in middle-age |
Features
·
may present with signs of chronic liver disease
·
acute hepatitis: fever, jaundice etc (only 25% present in this
way)
·
amenorrhoea (common)
·
ANA/SMA/LKM1 antibodies, raised IgG levels
·
liver biopsy: inflammation extending beyond limiting plate
'piecemeal necrosis', bridging necrosis
Management
·
steroids, other immunosuppressants e.g. azathioprine
·
liver transplantation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Coeliac disease: investigation
Coeliac disease is caused by
sensitivity to the protein gluten. Repeated exposure leads to villous atrophy
which in turn causes malabsorption. Conditions associated with coeliac disease
include dermatitis herpetiformis (a vesicular, pruritic skin eruption) and
autoimmune disorders (type 1 diabetes mellitus and autoimmune hepatitis).
Diagnosis is made by a combination
of immunology and jejunal biopsy. Villous atrophy and immunology normally
reverses on a gluten-free diet.
NICE issued guidelines on the
investigation of coeliac disease in 2009. If patients are already taking a
gluten-free diet they should be asked, if possible, to reintroduce gluten for
at least 6 weeks prior to
testing.
Immunology
·
tissue transglutaminase (TTG) antibodies (IgA) are first-choice according to NICE
·
endomyseal antibody (IgA)
o needed to look for selective IgA
deficiency, which would give a false negative coeliac result
·
anti-gliadin antibody (IgA or IgG) tests are not recommended by
NICE
·
anti-casein antibodies are also found in some patients
Duodenal biopsy*
·
villous atrophy
·
crypt hyperplasia
·
increase in intraepithelial lymphocytes
·
lamina propria infiltration with lymphocytes
Rectal gluten challenge has been
described but is not widely used
|
|
|
|
©
Image used on license from PathoPic |
|

Duodenal biopsy from a patient with coeliac disease.
Complete atrophy of the villi with flat mucosa and marked crypt hyperplasia.
Intraepithelial lymphocytosis. Dense mixed inflammatory infiltrate in the
lamina propria.
|
|
|
|
©
Image used on license from PathoPic |
|

Duodenal biopsy from a patient with coeliac disease.
Flat mucosa with hyperplastic crypts and dense cellular infiltrate in the
lamina propria. Increased number of intraepithelial lymphocytes and vacuolated
superficial epithelial cell vacuolated superficial epithelial cells. Higher
magnification image on the right.
*these are also occasionally
performed from the jejunum
From <https://www.passmedicine.com/review/textbook.php?s=#>
Target
cells and Howell-Jolly bodies may be seen in coeliac disease → hyposplenism
From <https://www.passmedicine.com/question/questions.php?q=0>
24 December 2020
14:13
Non-alcoholic fatty liver disease
Non-alcoholic fatty liver disease
(NAFLD) is now the most common cause of liver disease in the developed world.
It is largely caused by obesity and describes a spectrum of disease ranging
from:
·
steatosis - fat in the liver
·
steatohepatitis - fat with inflammation, non-alcoholic
steatohepatitis (NASH), see below
·
progressive disease may cause fibrosis and liver cirrhosis
NAFLD is thought to represent the
hepatic manifestation of the metabolic syndrome and hence insulin resistance is thought to be the key mechanism leading to steatosis.
Non-alcoholic steatohepatitis
(NASH) is a term used to describe liver changes similar to those seen in
alcoholic hepatitis in the absence of a history of alcohol abuse. It is
relatively common and thought to affect around 3-4% of the general population.
The progression of disease in patients with NASH may be responsible for a
proportion of patients previously labelled as cryptogenic cirrhosis.
Associated factors
·
obesity
·
type 2 diabetes mellitus
·
hyperlipidaemia
·
jejunoileal bypass
·
sudden weight loss/starvation
Features
·
usually asymptomatic
·
hepatomegaly
·
ALT is typically greater than AST
·
increased echogenicity on ultrasound
NICE produced guidelines on the
investigation and management of NAFLD in 2016. Key points:
·
there is no evidence to support screening for NAFLD in adults,
even in at risk groups (e.g. type 2 diabetes)
·
the guidelines are therefore based on the management of the incidental finding of NAFLD - typically asymptomatic fatty changes on liver
ultrasound
·
in these patients, NICE recommends the use of the enhanced liver
fibrosis (ELF) blood test to check for advanced fibrosis
·
the ELF blood test is a combination of hyaluronic acid +
procollagen III + tissue inhibitor of metalloproteinase 1. An algorithm based
on these values results in an ELF blood test score, similar to triple testing
for Down's syndrome
An excellent review by Byrne et Al1 in 2018
reviewed the diagnosis and monitoring of NAFLD. It made the following
suggestions if the ELF blood test was not available:
·
non-invasive tests may be used to assess the severity of
fibrosis
·
these include the FIB4 score or NALFD fibrosis score
·
these scores may be used in combination with a FibroScan (liver
stiffness measurement assessed with transient elastography)
·
this combination has been shown to have excellent accuracy in
predicting fibrosis
Patients who are likely to have
advanced fibrosis should be referred to a liver specialist. They will then
likely have a liver biopsy to stage the disease more accurately.
Management
·
the mainstay of treatment is lifestyle changes (particularly weight loss) and monitoring
·
there is ongoing research into the role of gastric banding and
insulin-sensitising drugs (e.g. metformin, pioglitazone)
References
1. BMJ 2018;362:k2734
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Achalasia
Failure of oesophageal peristalsis
and of relaxation of the lower oesophageal sphincter (LOS) due to degenerative
loss of ganglia from Auerbach's plexus i.e. LOS contracted, oesophagus above
dilated. Achalasia typically presents in middle-age and is equally common in
men and women.
Clinical features
·
dysphagia of BOTH liquids and solids
·
typically variation in severity of symptoms
·
heartburn
·
regurgitation of food
o may lead to cough, aspiration
pneumonia etc
·
malignant change in small number of patients
Investigations
·
oesophageal manometry
o excessive LOS tone which doesn't
relax on swallowing
o considered the most important
diagnostic test
·
barium swallow
o shows grossly expanded oesophagus,
fluid level
o 'bird's beak' appearance
·
chest x-ray
o wide mediastinum
o fluid level
Treatment
·
pneumatic (balloon) dilation is increasingly the preferred
first-line option
o less invasive and quicker recovery
time than surgery
o patients should be a low surgical
risk as surgery may be required if complications occur
·
surgical intervention with a Heller
cardiomyotomy should be considered if recurrent or
persistent symptoms
·
intra-sphincteric injection of botulinum toxin is sometimes used
in patients who are a high surgical risk
·
drug therapy (e.g. nitrates, calcium channel blockers) has a
role but is limited by side-effects
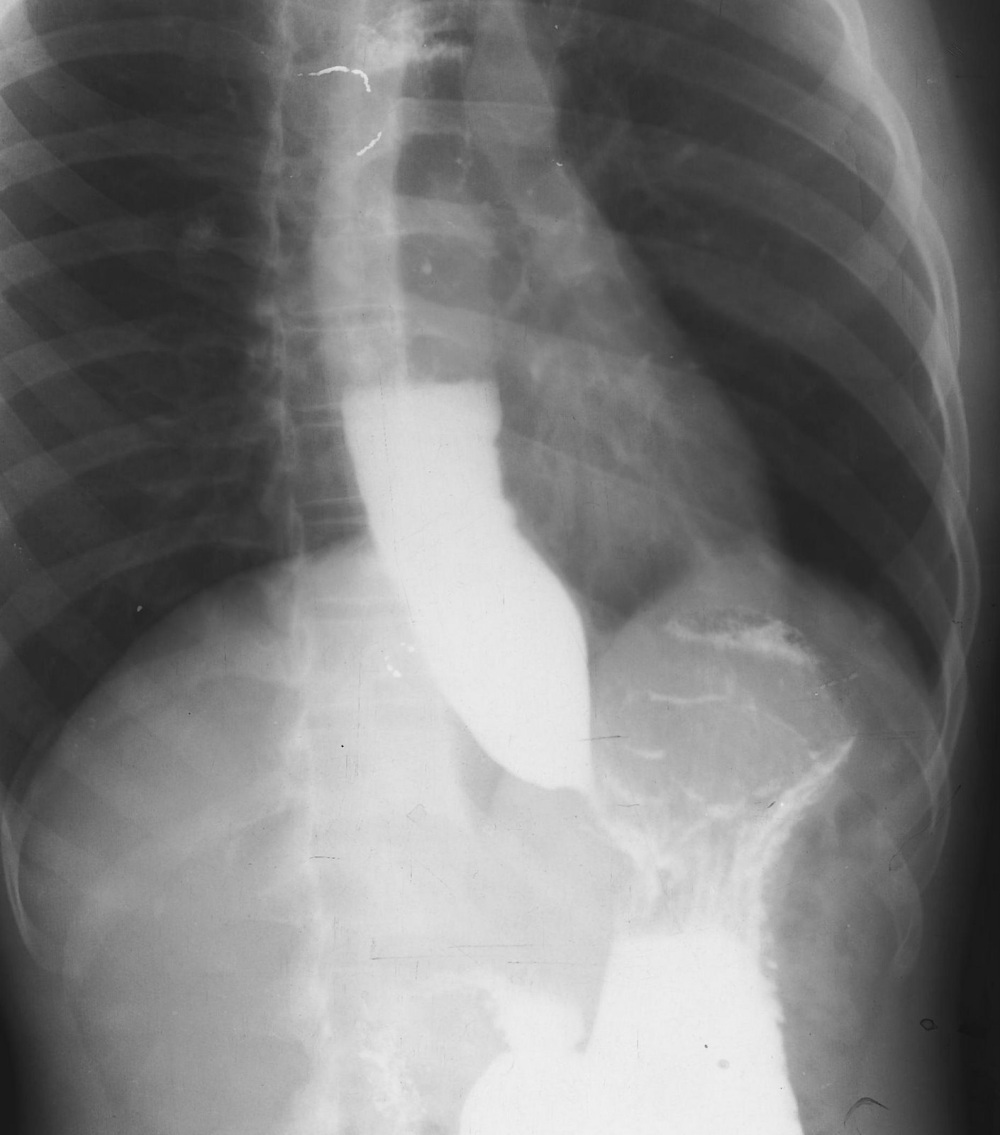

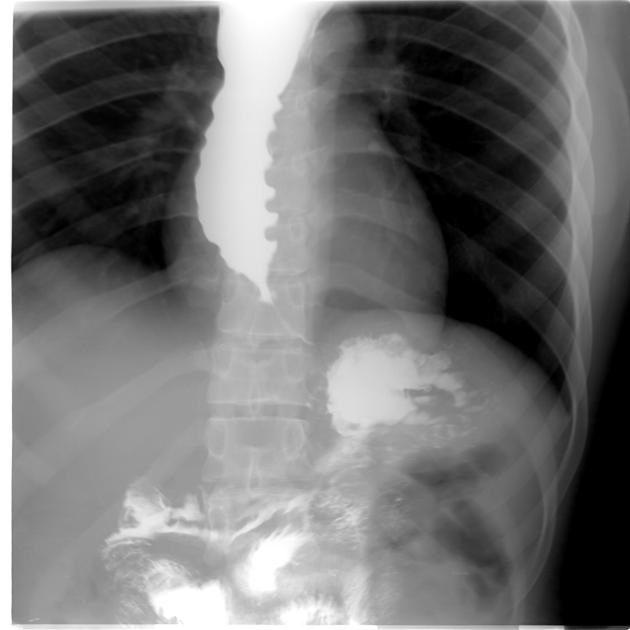
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Alcohol: units
In 2016 the Chief Medical Officer
proposed new guidelines in relation to the safe consumption of alcohol
following an expert group report. The most significant change has been a
reduction in the number of units it is recommending men do not exceed from 21
to 14, in line with the recommendations for women.
The government now recommend the
following:
·
men and women should drink no more than 14
units of alcohol per week
·
they advise 'if you do drink as much as 14
units per week, it is best to spread this evenly over 3 days or more'
·
pregnant women should not drink. The wording of the official
advice is 'If you are pregnant or planning a
pregnancy, the safest approach is not to drink alcohol at all, to keep risks to
your baby to a minimum. Drinking in pregnancy can lead to long-term harm to the
baby, with the more you drink the greater the risk.'
One unit of alcohol is equal to 10
mL of pure ethanol. The 'strength' of an alcoholic drink is determined by the
'alcohol by volume' (ABV).
Examples of one unit of alcohol:
·
25ml single measure of spirits (ABV 40%)
·
a third of a pint of beer (ABV 5 to 6%)
·
half a 175ml 'standard' glass of red wine (ABV 12%)
To calculate the number of units in
a drink multiply the number of millilitres by the ABV and divide by 1,000. For
example:
·
half a 175ml 'standard' glass of red wine = 87.5 * 12 / 1000 =
1.05 units
·
one bottle of wine = 750 * 12 / 1000 = 9 units
·
one pint of 5% beer or lager = 568 * 5 / 1000 = 2.8 units
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Ascites
The causes of ascites can be
grouped into those with a serum-ascites albumin gradient (SAAG) <11 g/L or a
gradient >11g/L as per the table below:
|
SAAG
> 11g/L |
SAAG <11g/L |
|
Indicates portal hypertension Cirrhosis Alcoholic hepatitis Cardiac ascites Mixed ascites Massive liver metastases Fulminant hepatic failure Budd-Chiari syndrome Portal vein thrombosis Veno-occlusive disease Myxoedema Fatty liver of pregnancy |
Peritoneal carcinomatosis Tuberculous peritonitis Pancreatic ascites Bowel obstruction Biliary ascites Postoperative lymphatic leak Serositis in connective tissue diseases |
Management
·
reducing dietary sodium
·
fluid restriction is sometimes recommended if the sodium is <
125 mmol/L
·
aldosterone antagonists: e.g. spironolactone
o loop diuretics are often added.
Some authorities only add loop diuretics in patients who don't respond to
aldosterone agonists whereas other authorities suggest starting both types of
diuretic on the first presentation of ascites
·
drainage if tense ascites (therapeutic abdominal paracentesis)
o large-volume
paracentesis for the treatment of ascites requires albumin 'cover'. Evidence
suggests this reduces paracentesis-induced circulatory dysfunction and
mortality
o paracentesis induced circulatory
dysfunction can occur due to large volume paracentesis (> 5 litres). It is
associated with a high rate of ascites recurrence, development of hepatorenal
syndrome, dilutional hyponatraemia, and high mortality rate
·
prophylactic antibiotics to reduce the risk of spontaneous
bacterial peritonitis. NICE recommend: 'Offer
prophylactic oral ciprofloxacin or norfloxacin for people with cirrhosis and
ascites with an ascitic protein of 15 g/litre or less, until the ascites has
resolved'
·
a transjugular intrahepatic portosystemic shunt (TIPS) may be
considered in some patients
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Diarrhoea
The table below gives
characteristic features for conditions causing diarrhoea:
World Health Organisation
definitions
·
Diarrhoea: > 3 loose or watery stool per day
·
Acute diarrhoea < 14 days
·
Chronic diarrhoea > 14 days
Usually acute
|
Condition |
Notes |
|
Gastroenteritis |
May be accompanied by abdominal pain or
nausea/vomiting |
|
Diverticulitis |
Classically causes left lower quadrant
pain, diarrhoea and fever |
|
Antibiotic therapy |
More common with broad spectrum
antibiotics Clostridium difficile is also seen with antibiotic use |
|
Constipation causing overflow |
A history of alternating diarrhoea and
constipation may be given May lead to faecal incontinence in the
elderly |
Usually chronic
|
Condition |
Notes |
|
Irritable bowel syndrome |
Extremely common. The most consistent
features are abdominal pain, bloating and change in bowel habit. Patients may
be divided into those with diarrhoea predominant IBS and those with
constipation-predominant IBS. Features such as lethargy, nausea,
backache and bladder symptoms may also be present |
|
Ulcerative colitis |
Bloody diarrhoea may be seen. Crampy abdominal pain and weight loss
are also common. Faecal urgency and tenesmus may
be seen |
|
Crohn's disease |
Crampy abdominal pains and diarrhoea.
Bloody diarrhoea less common than in ulcerative colitis. Other features
include malabsorption, mouth ulcers, perianal
disease and intestinal
obstruction |
|
Colorectal cancer |
Symptoms depend on the site of the
lesion but include diarrhoea, rectal bleeding, anaemia and constitutional
symptoms e.g. Weight loss and anorexia |
|
Coeliac disease |
In children may present with failure to
thrive, diarrhoea and abdominal distension In adults lethargy, anaemia, diarrhoea
and weight loss are seen. Other autoimmune conditions may coexist |
Other conditions associated with
diarrhoea include:
·
thyrotoxicosis
·
laxative abuse
·
appendicitis
·
radiation enteritis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Dyspepsia
The 2015 NICE guidelines 'Suspected
cancer: recognition and referral' further updated the advice on who needs
urgent referral for an endoscopy (i.e. within 2 weeks). The list below combines
the advice for oesophageal and stomach cancer, with the bold added by the
author, not NICE.
Urgent
All patients who've got dysphagia
All patients who've got an upper abdominal mass consistent with stomach cancer
Patients aged >= 55 years who've
got weight loss, AND any of the following:
·
upper abdominal pain
·
reflux
·
dyspepsia
Non-urgent
Patients with haematemesis
Patients aged >= 55 years who've
got:
·
treatment-resistant dyspepsia or
·
upper abdominal pain with low haemoglobin levels or
·
raised platelet count with any of the following: nausea,
vomiting, weight loss, reflux, dyspepsia, upper abdominal pain
·
nausea or vomiting with any of the following: weight loss,
reflux, dyspepsia, upper abdominal pain
Managing patients who do not meet
referral criteria ('undiagnosed dyspepsia')
This can be summarised at a
step-wise approach
·
1. Review medications for possible causes of dyspepsia
·
2. Lifestyle advice
·
3. Trial of full-dose proton pump inhibitor for one month OR a
'test and treat' approach for H. pylori
o if symptoms persist after either of
the above approaches then the alternative approach should be tried
Testing for H. pylori infection
·
initial diagnosis: NICE recommend using a carbon-13 urea breath
test or a stool antigen test, or laboratory-based serology 'where its
performance has been locally validated'
·
test of cure:
o there is no
need to check for H. pylori eradication if symptoms have
resolved following test
and treat
o however, if repeat testing is
required then a carbon-13 urea breath test should be used
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Gallstones
Up to 24% of women and 12% of men
may have gallstones. Of these up to 30% may develop local infection and
cholecystitis. In patients subjected to surgery, 12% will have stones contained
within the common bile duct. The majority of gallstones are of a mixed
composition (50%) with pure cholesterol stones accounting for 20% of cases.
The aetiology of CBD stones differs
in the world, in the West most CBD stones are the result of migration. In the
East, a far higher proportion arise in the CBD de novo.
The classical symptoms are of
colicky right upper quadrant pain that occurs postprandially. The symptoms are
usually worst following a fatty meal when cholecystokinin levels are highest
and gallbladder contraction is maximal.
Investigation
In almost all suspected cases the
standard diagnostic workup consists of abdominal ultrasound and liver function
tests. Of patients who have stones within the bile duct, 60% will have at least
one abnormal result on LFT's. Ultrasound is an important test, but is operator
dependent and therefore may occasionally need to be repeated if a negative
result is at odds with the clinical picture. Where stones are suspected in the
bile duct the options lie between magnetic resonance cholangiography and
intraoperative imaging. The choice between these two options is determined by
the skills and experience of the surgeon. The advantages of intraoperative
imaging are less useful in making therapeutic decisions if the operator is
unhappy about proceeding the bile duct exploration, and in such circumstances,
preoperative MRCP is probably a better option.
Specific gallstone and gallbladder
related disease
|
Disease |
Features |
Management |
|
Biliary colic |
Colicky abdominal pain, worse
postprandially, worse after fatty foods |
If imaging shows gallstones and history
compatible then laparoscopic cholecystectomy |
|
Acute cholecystitis |
Right upper quadrant pain Fever Murphys sign on examination Occasionally mildly deranged LFT's (especially
if Mirizzi syndrome) |
Imaging (USS) and cholecystectomy
(ideally within 48 hours of presentation) (2) |
|
Gallbladder abscess |
Usually prodromal illness and right
upper quadrant pain Swinging pyrexia Patient may be systemically unwell Generalised peritonism not present |
Imaging with USS +/- CT Scanning Ideally, surgery although subtotal
cholecystectomy may be needed if Calot's triangle is hostile In unfit patients, percutaneous
drainage may be considered |
|
Cholangitis |
Patient severely septic and unwell Jaundice Right upper quadrant pain |
Fluid resuscitation Broad-spectrum intravenous antibiotics Correct any coagulopathy Early ERCP |
|
Gallstone ileus |
Patients may have a history of previous
cholecystitis and known gallstones Small bowel obstruction (may be
intermittent) |
Laparotomy and removal of the gallstone
from small bowel, the enterotomy must be made proximal to the site of
obstruction and not at the site of obstruction. The fistula between the
gallbladder and duodenum should not be interfered with. |
|
Acalculous cholecystitis |
Patients with intercurrent illness
(e.g. diabetes, organ failure) Patient of systemically unwell Gallbladder inflammation in absence of
stones High fever |
If patient fit then cholecystectomy, if
unfit then percutaneous cholecystostomy |
Treatment
Asymptomatic gallstones which are
located in the gallbladder are common and do not require treatment. However, if
stones are present in the common bile duct there is an increased risk of
complications such as cholangitis or pancreatitis and surgical management
should be considered.
Patients with asymptomatic
gallstones rarely develop symptoms related to them (less than 2% per year) and
may, therefore, be managed expectantly. In almost all cases of symptomatic
gallstones the treatment of choice is cholecystectomy performed via the
laparoscopic route. In the very frail patient, there is sometimes a role for
the selective use of ultrasound guided cholecystostomy.
During the course of the procedure,
some surgeons will routinely perform either intraoperative cholangiography to
either confirm anatomy or to exclude CBD stones. The latter may be more easily
achieved by use of laparoscopic ultrasound. If stones are found then the
options lie between early ERCP in the day or so following surgery or immediate
surgical exploration of the bile duct. When performed via the trans cystic
route this adds little in the way of morbidity and certainly results in faster
recovery. Where transcystic exploration fails the alternative strategy is that
of formal choledochotomy. The exploration of a small duct is challenging and
ducts of less than 8mm should not be explored. Small stones that measure less
than 5mm may be safely left and most will pass spontaneously.
Risks of ERCP(1)
·
Bleeding 0.9% (rises to 1.5% if sphincterotomy performed)
·
Duodenal perforation 0.4%
·
Cholangitis 1.1%
·
Pancreatitis 1.5%
References
1. Williams E et al. Guidelines on the management of common bile duct stones (CBDS)Gut 2008;57:10041021
2. Gurusamy KS, Samraj K. Early
versus delayed laparoscopic cholecystectomy for acute cholecystitis. Cochrane
Database Syst Rev. 2006 Oct 18;(4):CD005440.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Hepatobiliary disease and related disorders
The table below gives
characteristic exam question features for conditions causing hepatobiliary
disease and related disorders:
|
Condition |
Features |
|
Viral hepatitis |
Common symptoms include: ·
nausea and vomiting, anorexia ·
myalgia ·
lethargy ·
right upper quadrant (RUQ) pain Questions may point to risk factors
such as foreign travel or intravenous drug use. |
|
Congestive hepatomegaly |
The liver only usually causes pain if
stretched. One common way this can occur is as a consequence of congestive heart
failure. In severe cases cirrhosis may occur. |
|
Biliary colic |
RUQ pain, intermittent, usually begins
abruptly and subsides gradually. Attacks often occur after eating. Nausea is
common. It is sometimes taught that patients
are female, forties, fat and fair although this is obviously a
generalisation. |
|
Acute cholecystitis |
Pain similar to biliary colic but more
severe and persistent. The pain may radiate to the back or right shoulder. The patient may be pyrexial and
Murphy's sign positive (arrest of inspiration on palpation of the RUQ) |
|
Ascending cholangitis |
An infection of the bile ducts commonly
secondary to gallstones. Classically presents with a triad of: ·
fever (rigors are common) ·
RUQ pain ·
jaundice |
|
Gallstone ileus |
This describes small bowel obstruction
secondary to an impacted gallstone. It may develop if a fistula forms between
a gangrenous gallbladder and the duodenum. Abdominal pain, distension and vomiting
are seen. |
|
Cholangiocarcinoma |
Persistent biliary colic symptoms,
associated with anorexia, jaundice and weight loss. A palpable mass in the
right upper quadrant (Courvoisier sign), periumbilical lymphadenopathy
(Sister Mary Joseph nodes) and left supraclavicular adenopathy (Virchow node)
may be seen |
|
Acute pancreatitis |
Usually due to alcohol or gallstones Severe epigastric pain Vomiting is common Examination may reveal tenderness,
ileus and low-grade fever Periumbilical discolouration (Cullen's
sign) and flank discolouration (Grey-Turner's sign) is described but rare |
|
Pancreatic cancer |
Painless jaundice is the classical
presentation of pancreatic cancer. However pain is actually a relatively
common presenting symptom of pancreatic cancer. Anorexia and weight loss are
common |
|
Amoebic liver abscess |
Typical symptoms are malaise, anorexia
and weight loss. The associated RUQ pain tends to be mild and jaundice is
uncommon. |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Spontaneous bacterial peritonitis
Spontaneous bacterial peritonitis
(SBP) is a form of peritonitis usually seen in patients with ascites secondary
to liver cirrhosis.
Features
·
ascites
·
abdominal pain
·
fever
Diagnosis
·
paracentesis: neutrophil count > 250 cells/ul
·
the most common organism found on ascitic fluid culture is E. coli
Management
·
intravenous cefotaxime is usually given
Antibiotic prophylaxis should be
given to patients with ascites if:
·
patients who have had an episode of SBP
·
patients with fluid protein <15 g/l and either Child-Pugh
score of at least 9 or hepatorenal syndrome
·
NICE recommend: 'Offer prophylactic oral ciprofloxacin or norfloxacin for people with cirrhosis and ascites with an ascitic protein of
15 g/litre or less until the ascites has resolved'
Alcoholic liver disease is a marker
of poor prognosis in SBP.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Ulcerative colitis
Ulcerative colitis (UC) is a form
of inflammatory bowel disease. Inflammation always starts at rectum (hence it
is the most
common site for UC), never spreads beyond ileocaecal
valve and is continuous. The peak incidence of ulcerative colitis is in people aged
15-25 years and in those aged 55-65 years.
The initial presentation is usually
following insidious and intermittent symptoms. Features include:
·
bloody diarrhoea
·
urgency
·
tenesmus
·
abdominal pain, particularly in the left lower quadrant
·
extra-intestinal features (see below)
Questions regarding the
'extra-intestinal' features of inflammatory bowel disease are common:
|
|
Common to both Crohn's disease (CD) and
Ulcerative colitis (UC) |
Notes |
|
Related to disease activity |
Arthritis: pauciarticular, asymmetric Erythema nodosum Episcleritis Osteoporosis |
Arthritis is the most common
extra-intestinal feature in both CD and UC Episcleritis is more common in CD |
|
Unrelated to disease activity |
Arthritis: polyarticular, symmetric Uveitis Pyoderma gangrenosum Clubbing Primary sclerosing cholangitis |
Primary sclerosing cholangitis is much
more common in UC Uveitis is more common in UC |
|
|
|
|
|
|
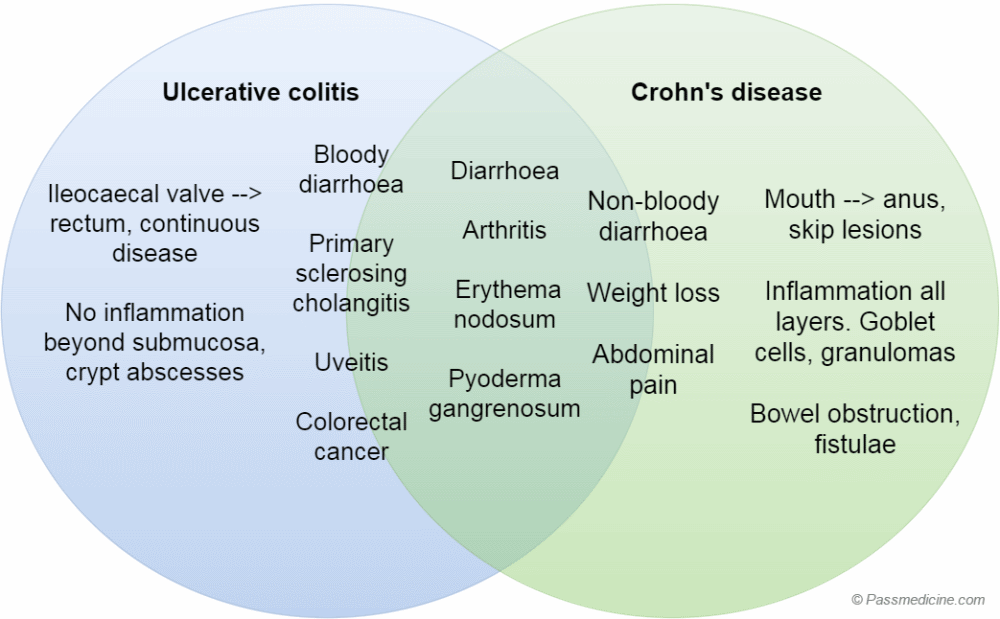
Venn diagram showing shared features and differences
between ulcerative colitis and Crohn's disease. Note that whilst some features
are present in both, some are much more common in one of the conditions, for
example colorectal cancer in ulcerative colitis
Pathology
·
red, raw mucosa, bleeds easily
·
no inflammation beyond submucosa (unless fulminant disease)
·
widespread ulceration with preservation of adjacent mucosa which
has the appearance of polyps ('pseudopolyps')
·
inflammatory cell infiltrate in lamina propria
·
neutrophils migrate through the walls of glands to form crypt abscesses
·
depletion of goblet cells and mucin from gland epithelium
·
granulomas are infrequent
Barium enema
·
loss of haustrations
·
superficial ulceration, 'pseudopolyps'
·
long standing disease: colon is narrow and short
-'drainpipe colon'
|
|
|
|
©
Image used on license from Radiopaedia |
|
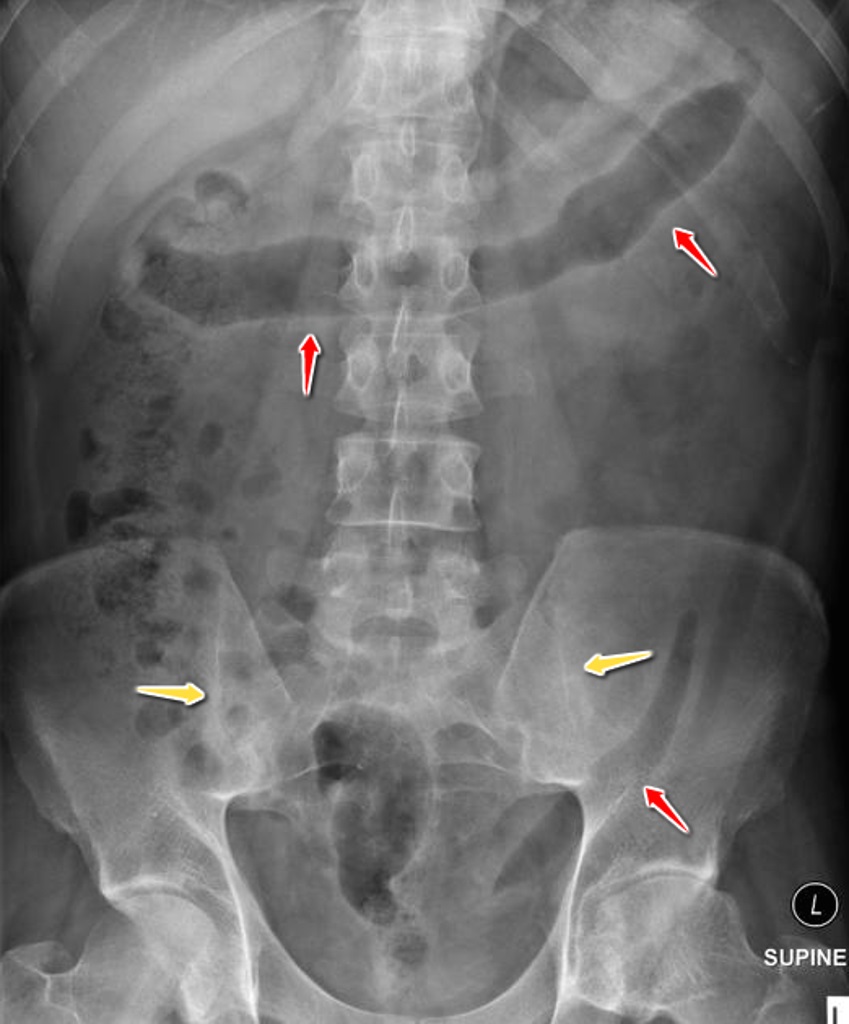
Abdominal x-ray from a patient with ulcerative colitis
showing lead pipe appearance of the colon (red arrows). Ankylosis of the left
sacroiliac joint and partial ankylosis on the right (yellow arrow), reinforcing
the link with sacroilitis.
|
|
|
|
©
Image used on license from Radiopaedia |
|

Barium enema from a patient with ulcerative colitis. The
whole colon, without skips is affected by an irregular mucosa with loss of
normal haustral markings.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Helicobacter pylori: tests
Urea breath test
·
patients consume a drink containing carbon isotope 13 (13C)
enriched urea
·
urea is broken down by H. pylori urease
·
after 30 mins patient exhale into a glass tube
·
mass spectrometry analysis calculates the amount of 13C CO2
·
should not be performed within 4
weeks of treatment with an antibacterial or within 2 weeks of an antisecretory
drug (e.g. a proton pump inhibitor)
·
sensitivity 95-98%, specificity 97-98%
·
may be used to check for H.
pylori eradication
Rapid urease test (e.g. CLO test)
·
biopsy sample is mixed with urea and pH indicator
·
colour change if H pylori urease activity
·
sensitivity 90-95%, specificity 95-98%
Serum antibody
·
remains positive after eradication
·
sensitivity 85%, specificity 80%
Culture of gastric biopsy
·
provide information on antibiotic sensitivity
·
sensitivity 70%, specificity 100%
Gastric biopsy
·
histological evaluation alone, no culture
·
sensitivity 95-99%, specificity 95-99%
Stool antigen test
·
sensitivity 90%, specificity 95%
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Acute liver failure
Acute liver failure describes the
rapid onset of hepatocellular dysfunction leading to a variety of systemic
complications.
Causes
·
paracetamol overdose
·
alcohol
·
viral hepatitis (usually A or B)
·
acute fatty liver of pregnancy
Features*
·
jaundice
·
coagulopathy: raised prothrombin time
·
hypoalbuminaemia
·
hepatic encephalopathy
·
renal failure is common ('hepatorenal syndrome')
*remember that 'liver function
tests' do not always accurately reflect the synthetic function of the liver.
This is best assessed by looking at the prothrombin time and albumin level.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Budd-Chiari syndrome
Budd-Chiari syndrome, or hepatic
vein thrombosis, is usually seen in the context of underlying haematological
disease or another procoagulant condition.
Causes
·
polycythaemia rubra vera
·
thrombophilia: activated protein C resistance, antithrombin III
deficiency, protein C & S deficiencies
·
pregnancy
·
combined oral contraceptive pill: accounts for around 20% of
cases
The features are
classically a triad of:
·
abdominal pain: sudden onset, severe
·
ascites → abdominal distension
·
tender hepatomegaly
Investigations
·
ultrasound with Doppler flow studies is very sensitive and should be the
initial radiological investigation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Coeliac disease
Coeliac disease is an autoimmune
condition caused by sensitivity
to the protein gluten. It is thought to affect around 1%
of the UK population. Repeated exposure leads to villous atrophy which in turn
causes malabsorption. Conditions associated with
coeliac disease include dermatitis herpetiformis (a vesicular, pruritic skin
eruption) and autoimmune disorders (type 1 diabetes mellitus and autoimmune
hepatitis). It is strongly associated with HLA-DQ2 (95% of patients) and HLA-DQ8 (80%).
In 2009 NICE issued guidelines on
the investigation of coeliac disease. They suggest that the following patients
should be screened for coeliac disease:
|
Signs
and symptoms |
Conditions |
|
·
Chronic or intermittent diarrhoea ·
Failure to thrive or faltering growth (in children) ·
Persistent or unexplained gastrointestinal symptoms
including nausea and vomiting ·
Prolonged fatigue ('tired all the time') ·
Recurrent abdominal pain, cramping or distension ·
Sudden or unexpected weight loss ·
Unexplained iron-deficiency anaemia, or other
unspecified anaemia |
·
Autoimmune thyroid disease ·
Dermatitis herpetiformis ·
Irritable bowel syndrome ·
Type 1 diabetes ·
First-degree relatives (parents, siblings or
children) with coeliac disease |
Complications
·
anaemia: iron, folate and vitamin B12 deficiency (folate deficiency is more common
than vitamin B12 deficiency in coeliac disease)
·
hyposplenism
·
osteoporosis, osteomalacia
·
lactose intolerance
·
enteropathy-associated T-cell lymphoma of small intestine
·
subfertility, unfavourable pregnancy outcomes
·
rare: oesophageal cancer, other malignancies
|
|
|
|
©
Image used on license from PathoPic |
|
Duodenal biopsy from a patient with coeliac disease.
Complete atrophy of the villi with flat mucosa and marked crypt hyperplasia.
Intraepithelial lymphocytosis. Dense mixed inflammatory infiltrate in the
lamina propria.
|
|
|
|
©
Image used on license from PathoPic |
|
Duodenal biopsy from a patient with coeliac disease.
Flat mucosa with hyperplastic crypts and dense cellular infiltrate in the
lamina propria. Increased number of intraepithelial lymphocytes and vacuolated
superficial epithelial cell vacuolated superficial epithelial cells. Higher magnification
image on the right.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:13
Coeliac disease: management
The management of coeliac disease
involves a gluten-free
diet. Gluten-containing cereals include:
·
wheat: bread, pasta, pastry
·
barley: beer
o whisky is made using malted barley.
Proteins such as gluten are however removed during the distillation process
making it safe to drink for patients with coeliac disease
·
rye
·
oats
o some patients with coeliac disease
appear able to tolerate oats
Some notable foods which are
gluten-free include:
·
rice
·
potatoes
·
corn (maize)
Tissue transglutaminase antibodies
may be checked to check compliance with a gluten-free diet.
Immunisation
·
Patients with coeliac disease often have a degree of functional hyposplenism
·
For this reason, all patients with coeliac disease are offered the pneumococcal vaccine
o Coeliac UK
recommends that everyone with coeliac disease is vaccinated against
pneumococcal infection and has a booster every 5 years
·
Currrent guidelines suggest giving the influenza vaccine on an
individual basis.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Colorectal cancer: genetics
It is currently thought there are
three types of colon cancer:
·
sporadic (95%)
·
hereditary non-polyposis colorectal carcinoma (HNPCC, 5%)
·
familial adenomatous polyposis (FAP, <1%)
Studies have shown that sporadic
colon cancer may be due to a series of genetic mutations. For example, more
than half of colon cancers show allelic loss of the APC gene. It is believed a
further series of gene abnormalities e.g. activation of the K-ras oncogene,
deletion of p53 and DCC tumour suppressor genes lead to invasive carcinoma
HNPCC, an autosomal dominant
condition, is the most
common form of inherited colon cancer. Around 90% of patients develop
cancers, often of the proximal colon, which are usually poorly
differentiated and highly aggressive. Currently seven mutations have been
identified, which affect genes involved in DNA mismatch repair leading to
microsatellite instability. The most common genes involved are:
·
MSH2 (60% of cases)
·
MLH1 (30%)
Patients with HNPCC are also at a
higher risk of other cancers, with endometrial cancer being the next most common association, after colon cancer.
The Amsterdam criteria are
sometimes used to aid diagnosis:
·
at least 3 family members with colon cancer
·
the cases span at least two generations
·
at least one case diagnosed before the age of 50 years
FAP is a rare autosomal dominant condition which leads to the formation of hundreds of polyps by the age of 30-40 years. Patients inevitably develop
carcinoma. It is due to a mutation in a tumour suppressor gene called adenomatous polyposis coli gene
(APC), located on chromosome 5. Genetic testing can be done
by analysing DNA from a patient's white blood cells. Patients generally have a
total colectomy with ileo-anal pouch formation in their twenties.
Patients with FAP are also at risk
from duodenal tumours. A variant of FAP called Gardner's syndrome can also
feature osteomas of the skull and mandible, retinal pigmentation, thyroid
carcinoma and epidermoid cysts on the skin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Crohn's disease: management
Crohn's disease is a form of
inflammatory bowel disease. It commonly affects the terminal ileum and colon
but may be seen anywhere from the mouth to anus. NICE published guidelines on
the management of Crohn's disease in 2012.
General points
·
patients should be strongly advised to stop smoking
·
some studies suggest an increased risk of relapse secondary to
NSAIDs and the combined oral contraceptive pill but the evidence is patchy
Inducing remission
·
glucocorticoids (oral, topical or intravenous) are generally
used to induce remission. Budesonide is an alternative in a subgroup of patients
·
enteral feeding with an elemental diet may be used in addition
to or instead of other measures to induce remission, particularly if there is
concern regarding the side-effects of steroids (for example in young children)
·
5-ASA drugs (e.g. mesalazine) are used second-line to
glucocorticoids but are not as effective
·
azathioprine or mercaptopurine* may be used as an add-on
medication to induce remission but is not used as monotherapy. Methotrexate is
an alternative to azathioprine
·
infliximab is useful in refractory disease and fistulating
Crohn's. Patients typically continue on azathioprine or methotrexate
·
metronidazole is often used for isolated peri-anal disease
Maintaining remission
·
as above, stopping smoking is a priority (remember: smoking
makes Crohn's worse, but may help ulcerative colitis)
·
azathioprine or mercaptopurine is used first-line to maintain
remission
·
methotrexate is used second-line
·
5-ASA drugs (e.g. mesalazine) should be considered if a patient
has had previous surgery
Surgery
·
around 80% of patients with Crohn's disease will eventually have
surgery
·
see below for further detail
Surgical interventions in Crohn's
disease
The commonest disease pattern in
Crohn's is stricturing terminal ileal disease and this often culminates in an
ileocaecal resection. Other procedures performed include segmental small bowel
resections and stricturoplasty. Colonic involvement in patients with Crohn's is
not common and, where found, distribution is often segmental. However, despite
this distribution segmental resections of the colon in patients with Crohn's
disease are generally not advocated because the recurrence rate in the
remaining colon is extremely high, as a result, the standard options of colonic
surgery in Crohn's patients are generally; sub total colectomy,
panproctocolectomy and staged sub total colectomy and proctectomy. Restorative
procedures such as ileoanal pouch have no role in therapy.
Crohn's disease is notorious for
the developmental of intestinal fistulae; these may form between the rectum and
skin (perianal) or the small bowel and skin. Fistulation between loops of bowel
may also occur and result in bacterial overgrowth and malabsorption. Management
of enterocutaneous fistulae involves controlling sepsis, optimising nutrition,
imaging the disease and planning definitive surgical management.
Complications of Crohn's disease
As well as the well-documented
complications described above, patients are also at risk of:
·
small bowel cancer (standard incidence ratio = 40)
·
colorectal cancer (standard incidence ration = 2, i.e. less than
the risk associated with ulcerative colitis)
·
osteoporosis
*assess thiopurine
methyltransferase (TPMT) activity before offering azathioprine or
mercaptopurine
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Hepatic encephalopathy
Hepatic encephalopathy may be seen
in liver disease of any cause. The aetiology is not fully understood but is
thought to include excess absorption of ammonia and glutamine from bacterial breakdown of proteins in the gut.
Whilst hepatic encephalopathy is
often associated with acute liver failure it may also be seen with chronic
disease. It is now recognised that many patients with liver cirrhosis may
develop subtle symptoms such as mild cognitive impairment before the features
become more recognisable ('minimal' or 'covert' hepatic encephalopathy). It has
also been noted that transjugular intrahepatic portosystemic shunting (TIPSS)
may precipitate encephalopathy.
Features
·
confusion, altered GCS (see below)
·
asterix: 'liver flap', arrhythmic negative myoclonus with a
frequency of 3-5 Hz
·
constructional apraxia: inability to draw a 5-pointed star
·
triphasic slow waves on EEG
·
raised ammonia level (not commonly measured anymore)
Grading of hepatic encephalopathy
·
Grade I: Irritability
·
Grade II: Confusion, inappropriate behaviour
·
Grade III: Incoherent, restless
·
Grade IV: Coma
Precipitating factors
·
infection e.g. spontaneous bacterial peritonitis
·
GI bleed
·
post transjugular intrahepatic portosystemic shunt
·
constipation
·
drugs: sedatives, diuretics
·
hypokalaemia
·
renal failure
·
increased dietary protein (uncommon)
Management
·
treat any underlying precipitating cause
·
NICE recommend lactulose first-line, with the
addition of rifaximin for the secondary prophylaxis of hepatic encephalopathy
·
lactulose is thought to work by promoting the excretion of
ammonia and increasing the metabolism of ammonia by gut bacteria
·
antibiotics such as rifaximin are thought to modulate the gut
flora resulting in decreased ammonia production
·
other options include embolisation of portosystemic shunts and
liver transplantation in selected patients
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Hepatocellular carcinoma
Hepatocellular carcinoma (HCC) is
the third most common cause of cancer worldwide. Chronic hepatitis B is the most
common cause of HCC worldwide with chronic hepatitis C being the most common
cause in Europe.
The main risk factor for developing
HCC is liver cirrhosis, for example secondary* to hepatitis B & C, alcohol, haemochromatosis and primary biliary cirrhosis. Other
risk factors include:
·
alpha-1 antitrypsin deficiency
·
hereditary tyrosinosis
·
glycogen storage disease
·
aflatoxin
·
drugs: oral contraceptive pill, anabolic steroids
·
porphyria cutanea tarda
·
male sex
·
diabetes mellitus, metabolic syndrome
Features
·
tends to present late
·
features of liver cirrhosis or failure may be seen: jaundice,
ascites, RUQ pain, hepatomegaly, pruritus, splenomegaly
·
possible presentation is decompensation in a patient with
chronic liver disease
·
raised AFP
Screening with ultrasound (+/-
alpha-fetoprotein) should be considered for high risk groups such as:
·
patients liver cirrhosis secondary to hepatitis B & C or
haemochromatosis
·
men with liver cirrhosis secondary to alcohol
Management options
·
early disease: surgical resection
·
liver transplantation
·
radiofrequency ablation
·
transarterial chemoembolisation
·
sorafenib: a multikinase inhibitor
*Wilson's disease is an exception
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Inflammatory bowel disease: key differences
The two main types of inflammatory
bowel disease are Crohn's disease and ulcerative colitis. They have many
similarities in terms of presenting symptoms, investigation findings and
management options.
|
|
|
|
|
|
Venn diagram showing shared features and differences
between ulcerative colitis and Crohn's disease. Note that whilst some features
are present in both, some are much more common in one of the conditions, for
example colorectal
cancer in ulcerative colitis
There are however some key
differences which are highlighted in table below:
|
|
Crohn's disease (CD) |
Ulcerative colitis (UC) |
|
Features |
Diarrhoea usually non-bloody Weight loss more prominent Upper gastrointestinal symptoms, mouth
ulcers, perianal disease Abdominal mass palpable in the right
iliac fossa |
Bloody diarrhoea more common Abdominal pain in the left lower
quadrant Tenesmus |
|
Extra-intestinal |
Gallstones are more common secondary to reduced bile acid
reabsorption Oxalate renal stones* |
Primary sclerosing cholangitis more common |
|
Complications |
Obstruction, fistula, colorectal cancer |
Risk of colorectal cancer high in UC
than CD |
|
Pathology |
Lesions may be seen anywhere from the
mouth to anus Skip lesions may be present |
Inflammation always starts at rectum
and never spreads beyond ileocaecal valve Continuous disease |
|
Histology |
Inflammation in all layers from mucosa
to serosa ·
increased goblet cells ·
granulomas |
No inflammation beyond submucosa (unless fulminant disease) - inflammatory cell
infiltrate in lamina propria ·
neutrophils migrate through the walls of glands to
form crypt abscesses ·
depletion of goblet cells and
mucin from gland epithelium ·
granulomas are infrequent |
|
Endoscopy |
Deep ulcers, skip lesions - 'cobble-stone' appearance |
Widespread ulceration with preservation
of adjacent mucosa which has the appearance of polyps ('pseudopolyps') |
|
Radiology |
Small bowel enema ·
high sensitivity and specificity for examination of
the terminal ileum ·
strictures: 'Kantor's string sign' ·
proximal bowel dilation ·
'rose thorn' ulcers ·
fistulae |
Barium enema ·
loss of haustrations ·
superficial ulceration, 'pseudopolyps' ·
long standing disease: colon is narrow and short -'drainpipe colon' |
*impaired bile acid rebsorption
increases the loss calcium in the bile. Calcium normally binds oxalate.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Ischaemic hepatitis
Ischaemic hepatitis is a diffuse
hepatic injury resulting from acute
hypoperfusion (sometimes known as 'shock liver').
It is not an inflammatory process. It is diagnosed in the presence of an
inciting event (e.g. a
cardiac arrest) and marked increases in aminotransferase levels
(exceeding 1000 international unit/L or 50 times the upper limit of normal).
Often, it will occur in conjunction with acute kidney injury (tubular necrosis)
or other end-organ dysfunction.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Metoclopramide
Metoclopramide is a D2 receptor antagonist* mainly used in the management of nausea. Other uses include:
·
gastro-oesophageal reflux disease
·
prokinetic action is useful in gastroparesis secondary to
diabetic neuropathy
·
often combined with analgesics for the treatment of migraine
(migraine attacks result in gastroparesis, slowing the absorption of
analgesics)
Adverse effects
·
extrapyramidal effects: oculogyric crisis. This is particularly a problem in
children and young adults
·
hyperprolactinaemia
·
tardive dyskinesia
·
parkinsonism
Metoclopramide should be avoided in bowel obstruction, but may be helpful in paralytic ileus.
*whilst metoclopramide is primarily
a D2 receptor antagonist, the mechanism of action is quite complicated:
·
it is also a mixed 5-HT3 receptor antagonist/5-HT4 receptor
agonist
·
the antiemetic action is due to its antagonist
activity at D2 receptors in the chemoreceptor trigger zone. At higher doses the 5-HT3
receptor antagonist also has an effect
·
the gastroprokinetic activity is
mediated by D2 receptor antagonist activity and 5-HT4 receptor agonist activity
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Peptic ulcer disease (uncomplicated)
Risk factors
·
Helicobacter pylori is associated with the majority of
peptic ulcers:
o 95% of duodenal ulcers
o 75% of gastric ulcers
·
drugs:
o NSAIDs
o SSRIs
o corticosteroids
o bisphosphonates
·
Zollinger-Ellison syndrome: rare cause characterised by
excessive levels of gastrin, usually from a gastrin secreting tumour
·
the role of alcohol and smoking is not clear
Features
·
epigastric pain
·
nausea
·
duodenal ulcers
o more common than gastric ulcers
o epigastric pain
when hungry, relieved by eating
·
gastric ulcers
o epigastric pain worsened by eating
Investigation
·
Helicobacter pylori should be tested for
o either a Urea breath test or stool
antigen test should be used first-line
Management
·
if Helicobacter pylori is negative then proton pump
inhibitors (PPIs) should be given until the ulcer is healed
·
if Helicobacter pylori is positive then eradication
therapy should be given
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Proton pump inhibitors
Proton pump inhibitors (PPI) cause irreversible blockade of H+/K+
ATPase of the gastric parietal cell.
Examples include omeprazole and
lansoprazole.
Adverse effects
·
hyponatraemia, hypomagnasaemia
·
osteoporosis → increased risk of fractures
·
microscopic colitis
·
increased risk of Clostridium difficile infections
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Ulcerative colitis: flares
Most ulcerative colitis flares
occur without an identifiable trigger. However, a number of factors are often
linked:
·
stress
·
medications
o NSAIDs
o antibiotics
·
cessation of smoking
Flares of ulcerative colitis are
usually classified as either mild, moderate or severe:
|
Mild |
Moderate |
Severe |
|
Fewer than four stools daily, with or
without blood No systemic disturbance Normal erythrocyte sedimentation rate
and C-reactive protein values |
Four to six stools a day, with minimal
systemic disturbance |
More than six stools a day, containing
blood Evidence of systemic disturbance, e.g. ·
fever ·
tachycardia ·
abdominal tenderness, distension or reduced bowel
sounds ·
anaemia ·
hypoalbuminaemia |
Patients with evidence of severe
disease should be admitted to hospital.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Acute appendicitis
Acute appendicitis is the most
common acute abdominal condition requiring surgery. It can occur at any age but
is most common in young people aged 10-20 years.
Abdominal pain is seen in the vast
majority of patients:
·
peri-umbilical abdominal pain (visceral stretching of appendix
lumen and appendix is midgut structure) radiating to the right iliac fossa
(RIF) due to localised parietal peritoneal inflammation.
·
the migration of the pain from the centre to the RIF has been
shown to be one of the strongest indicators of appendicitis
·
patients often report the pain being worse on coughing or going
over speed bumps. Children typically can't hop on the right leg due to the
pain.
Other features:
·
vomit once or twice but marked and persistent vomiting is
unusual
·
diarrhoea is rare. However, pelvic appendicitis may cause
localised rectal irritation of some loose stools. A pelvic abscess may also
cause diarrhoea
·
mild pyrexia is common - temperature is usually 37.5-38oC. Higher
temperatures are more typical of conditions like mesenteric adenitis
·
anorexia is very common. It is very unusual for patients with
appendicitis to be hungry
·
around 50% of patients have the typical symptoms of anorexia,
peri-umbilical pain and nausea followed by more localised right lower quadrant
pain
Examination
·
generalised peritonitis if perforation has occurred or localised
peritonism
·
retrocaecal appendicitis may have relatively few signs
·
digital rectal examination may reveal boggy sensation if pelvic
abscess is present, or even right-sided tenderness with a pelvic appendix
·
Rovsing's sign (palpation in the LIF causes pain in the RIF) is now thought to
be of limited value
Diagnosis
·
typically raised inflammatory markers coupled with compatible
history and examination findings should be enough to justify appendicectomy
·
a neutrophil-predominant leucocytosis is seen in 80-90%
·
urine analysis: useful to exclude pregnancy in women, renal
colic and urinary tract infection. In patients with appendicitis, urinalysis
may show mild leucocytosis but no nitrites
·
ultrasound is useful in females where pelvic organ pathology is
suspected. Although it is not always possible to visualise the appendix on
ultrasound, the presence of free fluid (always pathological in males) should
raise suspicion
·
CT scans are widely used in patients with suspected appendicitis
in the US but this practice has not currently reached the UK, due to the
concerns regarding excessive ionising radiation and resource limitations
Management
·
appendicectomy which can be performed via either an open or
laparoscopic approach. Laparoscopic appendicectomy is now the treatment of
choice
·
administration of prophylactic intravenous antibiotics reduces wound infection rates
·
patients with perforated appendicitis (typical around 15-20%)
require copious abdominal lavage.
·
patients without peritonitis who have an appendix mass should
receive broad-spectrum antibiotics and consideration given to performing an
interval appendicectomy.
·
be wary in the older patients who may have either an underlying
caecal malignancy or perforated sigmoid diverticular disease.
·
trials have looked at the use of intravenous antibiotics alone
in the treatment of appendicitis. The evidence currently suggests that whilst
this is successful in the majority of patients, it is associated with a longer
hospital stay and up to 20% of patients go on to have an appendicectomy within
12 months.
|
|
|
|
Image
sourced from Wikipedia |
|

Ultrasound examination may show evidence of lumenal
obstruction and thickening of the appendiceal wall as shown below
|
|
|
|
Image
sourced from Wikipedia |
|

Laparoscopic appendicectomy is becoming increasing
popular as demonstrated below
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Alcoholic ketoacidosis
Alcoholic ketoacidosis is a
non-diabetic euglycaemic form of ketoacidosis. It occurs in people who
regularly drink large amounts of alcohol. Often alcoholics will not eat
regularly and may vomit food that they do eat, leading to episodes of
starvation. Once the person becomes malnourished, after an alcohol binge the
body can start to break down body fat, producing ketones. Hence the patient
develops a ketoacidosis.
It typically presents with a pattern
of:
·
Metabolic acidosis
·
Elevated anion gap
·
Elevated serum ketone levels
·
Normal or low glucose concentration
The most appropriate treatment is
an infusion of saline &
thiamine. Thiamine is required to avoid Wernicke encephalopathy
or Korsakoff psychosis.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Aminosalicylate drugs
5-aminosalicyclic acid (5-ASA) is
released in the colon and is not absorbed. It acts locally as an
anti-inflammatory. The mechanism of action is not fully understood but 5-ASA
may inhibit prostaglandin synthesis
Sulphasalazine
·
a combination of sulphapyridine (a sulphonamide) and 5-ASA
·
many side-effects are due to the sulphapyridine moiety: rashes, oligospermia, headache, Heinz
body anaemia, megaloblastic anaemia, lung fibrosis
·
other side-effects are common to 5-ASA drugs (see mesalazine)
Mesalazine
·
a delayed release form of 5-ASA
·
sulphapyridine side-effects seen in patients taking
sulphasalazine are avoided
·
mesalazine is still however associated with side-effects such as
GI upset, headache, agranulocytosis, pancreatitis*, interstitial nephritis
Olsalazine
·
two molecules of 5-ASA linked by a diazo bond, which is broken
by colonic bacteria
Aminosalicylates are associated
with a variety of haematological
adverse effects, including agranulocytosis - FBC is a
key investigation in an unwell patient taking them.
*pancreatitis is 7 times more
common in patients taking mesalazine than sulfasalazine
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Barrett's oesophagus
Barrett's refers to the metaplasia
of the lower oesophageal mucosa, with the usual squamous epithelium being
replaced by columnar epithelium. There is an increased risk of oesophageal
adenocarcinoma, estimated at 50-100 fold. There are no screening programs for
Barrett's - it's typically identified when patients have an endoscopy for
evaluation of upper gastrointestinal symptoms such as dyspepsia.
Barrett's can be subdivided into
short (<3cm) and long (>3cm). The length of the affected segment
correlates strongly with the chances of identifying metaplasia. The overall
prevalence of Barrett's oesophagus is difficult to determine but may be in the
region of 1 in 20 and is identified in up to 12% of those undergoing endoscopy
for reflux.
Histological features
·
the columnar epithelium may resemble that of either the cardiac
region of the stomach or that of the small intestine (e.g. with goblet cells,
brush border)
Risk factors
·
gastro-oesophageal reflux disease (GORD) is the single strongest
risk factor
·
male gender (7:1 ratio)
·
smoking
·
central obesity
Interestingly alcohol does not seem
to be an independent risk factor for Barrett's although it is associated with
both GORD and oesophageal cancer.
Whilst Barrett's oesophagus itself
is asymptomatic clearly patients will often have coexistent GORD symptoms.
Management
·
endoscopic surveillance with biopsies
·
high-dose proton pump inhibitor: whilst this is commonly used in
patients with Barrett's the evidence base that this reduces the change of
progression to dysplasia or induces regression of the lesion is limited
Endoscopic surveillance
·
for patients with metaplasia (but not dysplasia) endoscopy is
recommended every 3-5 years
If dysplasia of any grade is identified
endoscopic intervention is offered. Options include:
·
endoscopic mucosal resection
·
radiofrequency ablation
|
|
|
|
|
|

Endoscopy image showing a short segment of Barrett's
oesophagus
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Crohn's disease: investigation
Crohn's disease is a form of
inflammatory bowel disease. It commonly affects the terminal ileum and colon
but may be seen anywhere from the mouth to anus
Bloods
·
C-reactive protein correlates well with disease activity
Endoscopy
·
colonoscopy is the investigation of choice
·
features suggest of Crohn's include deep ulcers, skip lesions
Histology
·
inflammation in all layers from mucosa to serosa
·
goblet cells
·
granulomas
Small bowel enema
·
high sensitivity and specificity for examination of the terminal
ileum
·
strictures: 'Kantor's string sign'
·
proximal bowel dilation
·
'rose thorn' ulcers
·
fistulae
|
|
|
|
©
Image used on license from Radiopaedia |
|

Barium study is shown from a patient with worsening
Crohn's disease. Long segment of narrowed terminal ileum in a 'string like'
configuration in keeping with a long stricture segment. Termed 'Kantor's string
sign'.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Hepatomegaly
Common causes of hepatomegaly
·
Cirrhosis: if early disease, later liver decreases in size.
Associated with a non-tender, firm liver
·
Malignancy: metastatic spread or primary hepatoma. Associated with a hard,
irregular. liver edge
·
Right heart failure: firm, smooth, tender liver
edge. May be pulsatile
Other causes
·
viral hepatitis
·
glandular fever
·
malaria
·
abscess: pyogenic, amoebic
·
hydatid disease
·
haematological malignancies
·
haemochromatosis
·
primary biliary cirrhosis
·
sarcoidosis, amyloidosis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Liver cirrhosis
Liver cirrhosis remains a
significant problem in the developed world, account for 60,000 deaths in the UK
each year.
Causes:
·
alcohol
·
non-alcoholic fatty liver disease (NAFLD)
·
viral hepatitis (B and C)
Diagnosis
·
traditionally a liver biopsy was used. This procedure is however
associated with adverse effects such as bleeding and pain
·
other techniques such as transient elastography and acoustic
radiation force impulse imaging are increasingly used and were recommended by
NICE in their 2016 guidelines
·
for patients with NAFLD, NICE recommend using the enhanced liver
fibrosis score to screen for patients who need further testing
What is transient elastography?
·
brand name 'Fibroscan'
·
uses a 50-MHz wave is passed into the liver from a small
transducer on the end of an ultrasound probe
·
measures the 'stiffness' of the liver which is a proxy for
fibrosis
In terms of screening for cirrhosis
NICE made a specific recommendation, suggesting to offer transient elastography
to:
·
people with hepatitis C virus infection
·
men who drink over 50 units of alcohol per week and women who
drink over 35 units of alcohol per week and have done so for several months
·
people diagnosed with alcohol-related liver disease
Further investigations
·
NICE recommend doing an upper endoscopy to check for varices in
patient's with a new diagnosis of cirrhosis
·
liver ultrasound every 6 months (+/- alpha-feto protein) to
check for hepatocellular cancer
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Oesophageal disorders
The table below lists a small group
of less common oesophageal disorders.
|
Disorder |
Notes |
|
Plummer-Vinson syndrome |
Triad of: ·
dysphagia (secondary to oesophageal webs) ·
glossitis ·
iron-deficiency anaemia Treatment includes iron supplementation
and dilation of the webs |
|
Mallory-Weiss syndrome |
Severe vomiting → painful mucosal
lacerations at the gastroesophageal junction resulting in haematemesis.
Common in alcoholics |
|
Boerhaave syndrome |
Severe vomiting → oesophageal rupture |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Peutz-Jeghers syndrome
Peutz-Jeghers syndrome is an autosomal dominant condition characterised by numerous hamartomatous polyps in the
gastrointestinal tract. It is also associated with pigmented freckles on the
lips, face, palms and soles. Although
the polyps themselves don't have malignant potential, around 50% of patients will have died from another
gastrointestinal tract cancer by the age of 60 years.
Genetics
·
autosomal dominant
·
responsible gene encodes serine threonine kinase LKB1 or STK11
Features
·
hamartomatous polyps in GI tract (mainly small bowel)
·
pigmented lesions on lips, oral mucosa, face, palms and soles
·
intestinal obstruction e.g. intussusception
·
gastrointestinal bleeding
Management
·
conservative unless complications develop
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Pharyngeal pouch
A pharyngeal pouch is a
posteromedial diverticulum through Killian's dehiscence. Killian's dehiscence
is a triangular area in the wall of the pharynx between the thyropharyngeus and
cricopharyngeus muscles. It is more common in older
patients and is 5 times more common in men
Features
·
dysphagia
·
regurgitation
·
aspiration
·
neck swelling which gurgles on palpation
·
halitosis
Management
·
surgery
|
|
|
|
©
Image used on license from Radiopaedia |
|

Still image taken from a barium swallow with
fluoroscopy. During swallowing an outpouching of the posterior hypopharyngeal
wall is visualised at the level C5-C6, right above the upper oesophageal
sphincter
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Small bowel bacterial overgrowth syndrome
Small bowel bacterial overgrowth
syndrome (SBBOS) is a disorder characterised by excessive amounts of bacteria
in the small bowel resulting in gastrointestinal symptoms.
Risk factors for SBBOS
·
neonates with congenital gastrointestinal abnormalities
·
scleroderma
·
diabetes mellitus
It should be noted that many of the
features overlap with irritable bowel syndrome:
·
chronic diarrhoea
·
bloating, flatulence
·
abdominal pain
Diagnosis
·
hydrogen breath test
·
small bowel aspiration and culture: this is used less often as
invasive and results are often difficult to reproduce
·
clinicians may sometimes give a course of antibiotics as a
diagnostic trial
Management
·
correction of underlying disorder
·
antibiotic therapy: rifaximin is now the treatment of choice due
to relatively low resistance. Co-amoxiclav or metronidazole are also effective
in the majority of patients.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Helicobacter pylori
Helicobacter pylori is a Gram
negative bacteria associated with a variety of gastrointestinal problems,
principally peptic ulcer disease
Associations
·
peptic ulcer disease (95% of duodenal ulcers, 75% of gastric
ulcers)
·
gastric cancer
·
B cell lymphoma of MALT tissue (eradication of H pylori results
causes regression in 80% of patients)
·
atrophic gastritis
The role of H pylori in
Gastro-oesophageal reflux disease (GORD) is unclear - there is currently no
role in GORD for the eradication of H pylori
Management - eradication may be
achieved with a 7 day course of
·
a proton pump inhibitor + amoxicillin + clarithromycin, or
·
a proton pump inhibitor + metronidazole + clarithromycin
|
|
|
|
|
|

H. pylori colonized on the surface of regenerative epithelium (silver
stain)
From <https://www.passmedicine.com/review/textbook.php?s=#>
Since
almost all Deodenal Ulcer are caused by H. pylori (HP) (in absence of NSAID
therapy) there is no need to perform a CLO test.
There
are many ways to make a diagnosis of HP. Non invasive tests include Urea breath
test, stool for HP antigen. Invasive tests are CLO, histological examination
and culture.
The
Camplyobacter-like organism (CLO) test is based on the fact that mucosal biopsy
specimens can be inoculated into a medium containing urea and phenol red, a dye
that turns pink in a pH of 6.0 or greater.
The
pH will rise above 6.0 when HP, the Campylobacter-like organism, metabolizes
urea to ammonia by way of its urease activity. This test is commercially
available and therefore quite inexpensive. Only one-half hour is required for
diagnosis of infection, and the test has shown 98% sensitivity and 100%
specificity.
In
case of a gastric ulcer (GU), since only 65-70% are due to HP, it is
recommended that the HP status be confirmed (preferably by a biopsy) before
starting therapy. A biopsy will also help rule out malignancy (this is not
usually a concern with DU).
From <https://mle.ncl.ac.uk/cases/page/15729/>
24 December 2020
14:14
Acute abdominal pain: a very basic introduction
Acute abdominal pain is one of the
most common presentations encountered in clinical practice.
Causes
One of the most common ways to
think about the potential causes is the location of the pain. Sometimes
patients present with generalised pain but probably the most common present is
pain in a particular region of the abdomen. Some conditions characteristically
cause central pain before localising to a particular area. A good example is
appendicitis, which typically presents with central abdominal pain before
localising to the right iliac fossa.
|
|
|
|
|
|

Diagram showing stereotypical areas where particular
conditions present. The diagram is not exhaustive and only lists the more
common conditions seen in clinical practice. Note how pain from renal causes
such as renal/ureteric colic and pyelonephritis may radiate and move from the
loins towards the suprapubic area.
This approach, whilst useful, is
however limited as patients commonly present with atypical findings and as
mentioned previously the site of the pain can change over time.
Another way of classifying the
causes of an acute abdomen, or any condition, is by using a surgical sieve:
Infective
·
gastroenteritis
·
appendicitis
·
diverticulitis
·
pyelonephritis
·
cholecystitis
·
cholangitis
·
pelvic inflammatory disease
·
hepatitis
·
pneumonia
Inflammatory
·
pancreatitis
·
peptic ulcer disease
Vascular
·
ruptured abdominal aortic aneurysm
·
mesenteric ischaemia
·
myocardial infarction
Traumatic
·
ruptured spleen
·
perforated viscus (e.g. oesophagus, stomach, bowel)
Metabolic
·
renal/ureteric stone
·
diabetic ketoacidosis
The tables below gives the key
characteristics of common causes of abdominal pain.
Hepatobiliary problems
|
Condition |
Typical location of pain |
Notes |
|
Biliary colic |
Right upper quadrant |
Caused by a gallstone getting lodged in
the bile duct Classically provoked by eating a fatty
meal In contrast to acute cholecystitis no
fever and inflammatory markers are normal |
|
Acute cholecystitis |
Right upper quadrant |
Inflammation/infection of the
gallbladder secondary to impacted gallstones Murphy's sign positive (arrest of
inspiration on palpation of the RUQ) Fever and raised inflammatory markers |
|
Ascending cholangitis |
Right upper quadrant |
Ascending cholangitis is a bacterial
infection of the biliary tree. The most common predisposing factor is
gallstones. Charcot's triad of right upper quadrant
pain, fever and jaundice occurs in about 20-50% of patients |
|
Acute pancreatitis |
Epigastrium, sometimes radiating
through to the back |
Usually due to alcohol or gallstones Pain is often very severe. Examination
may reveal tenderness, ileus and low-grade fever |
Upper gastrointestinal tract
problems
|
Condition |
Typical location of pain |
Notes |
|
Peptic ulcer disease |
Epigastrium |
There may be a history of NSAID use or
alcohol excess. Duodenal ulcers: more common than
gastric ulcers, epigastric pain relieved by eating Gastric ulcers: epigastric pain
worsened by eating Features of upper gastrointestinal
haemorrhage may be seen (haematemesis, melena etc) |
Lower gastrointestinal tract
problems
|
Condition |
Typical location of pain |
Notes |
|
Appendicitis |
Right iliac fossa |
Pain initial in the central abdomen
before localising to the right iliac fossa (RIF). Anorexia is common. Tachycardia,
low-grade pyrexia, tenderness in RIF Rovsing's sign: more pain in RIF than
LIF when palpating LIF |
|
Acute diverticulitis |
Left lower quadrant |
Colicky pain typically in the LLQ Diarrhoea, sometimes bloody. Fever, raised inflammatory markers and
white cells |
|
Intestinal obstruction |
Central |
History of malignancy (intraluminal
obstruction)/previous operations (adhesions) Vomiting. Not opened bowels recently 'Tinkling' bowel sounds |
Urological causes
|
Condition |
Typical location of pain |
Notes |
|
Renal colic |
Loin pain radiating to the groin |
Pain is often severe but intermittent.
Patient's are characteristically restless. Visible or non-visible haematuria may
be present |
|
Acute pyelonephritis |
Loin pain |
Fever and rigors are common as is
vomiting |
|
Urinary retention |
Suprapubic |
Caused by obstruction to the bladder
outflow. Much more common in men, who often have
a history of benign prostatic hyperplasia |
Gynaecological causes
Remember, all women of a
reproductive age who present with abdominal pain should be considered pregnant
until proven otherwise
|
Condition |
Typical location of pain |
Notes |
|
Ectopic pregnancy |
Right or left iliac fossa |
Typically presents with pain and a
history of amenorrhoea for the past 6-9 weeks. Vaginal bleeding may be
present |
Vascular causes
|
Condition |
Typical location of pain |
Notes |
|
Ruptured abdominal aortic aneurysm |
Central abdominal pain radiating to the
back |
Presentation may be catastrophic (e.g.
Sudden collapse) or sub-acute (persistent severe central abdominal pain with
developing shock) Patients may be shocked (hypotension,
tachycardic) Patients may have a history of
cardiovascular disease |
|
Mesenteric ischaemia |
Central abdominal pain |
Patients often have a history of atrial
fibrillation or other cardiovascular disease Diarrhoea, rectal bleeding may be seen A metabolic acidosis is often seen (due
to 'dying' tissue) |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Crohn's disease
Crohn's disease is a form of
inflammatory bowel disease. It commonly affects the terminal ileum and colon
but may be seen anywhere from the mouth to anus.
Pathology
·
cause is unknown but there is a strong genetic susceptibility
·
inflammation occurs in all layers, down to the serosa. This is
why patients with Crohn's are prone to strictures, fistulas and adhesions
Crohn's disease typically presents
in late adolescence or early adulthood. Features include:
·
presentation may be non-specific symptoms such as weight loss and lethargy
·
diarrhoea: the most prominent symptom in adults. Crohn's colitis
may cause bloody diarrhoea
·
abdominal pain: the most prominent symptom in children
·
perianal disease: e.g. Skin tags or ulcers
·
extra-intestinal features are more common in patients with
colitis or perianal disease
Investigations
·
raised inflammatory markers
·
increased faecal calprotectin
·
anaemia
·
low vitamin B12 and vitamin D
Questions regarding the
'extra-intestinal' features of inflammatory bowel disease are common:
|
|
Common to both Crohn's disease (CD) and
Ulcerative colitis (UC) |
Notes |
|
Related to disease activity |
Arthritis: pauciarticular, asymmetric Erythema nodosum Episcleritis Osteoporosis |
Arthritis is the most common
extra-intestinal feature in both CD and UC Episcleritis is more common in CD |
|
Unrelated to disease activity |
Arthritis: polyarticular, symmetric Uveitis Pyoderma gangrenosum Clubbing Primary sclerosing cholangitis |
Primary sclerosing cholangitis is much
more common in UC Uveitis is more common in UC |
|
|
|
|
|
|
Venn diagram showing shared features and differences
between ulcerative colitis and Crohn's disease. Note that whilst some features
are present in both, some are much more common in one of the conditions, for
example colorectal cancer in ulcerative colitis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:14
Drug-induced liver disease
Drug-induced liver disease is
generally divided into hepatocellular, cholestatic or mixed. There is however
considerable overlap, with some drugs causing a range of changes to the liver
The following drugs tend to cause a
hepatocellular picture:
·
paracetamol
·
sodium valproate, phenytoin
·
MAOIs
·
halothane
·
anti-tuberculosis: isoniazid, rifampicin, pyrazinamide
·
statins
·
alcohol
·
amiodarone
·
methyldopa
·
nitrofurantoin
The following drugs tend to cause
cholestasis (+/- hepatitis):
·
combined oral contraceptive pill
·
antibiotics: flucloxacillin, co-amoxiclav, erythromycin*
·
anabolic steroids, testosterones
·
phenothiazines: chlorpromazine, prochlorperazine
·
sulphonylureas
·
fibrates
·
rare reported causes: nifedipine
Liver cirrhosis
·
methotrexate
·
methyldopa
·
amiodarone
*risk may be reduced with
erythromycin stearate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Ferritin
Ferritin is an intracellular
protein that binds iron and stores it to be released in a controlled fashion at
sites where iron is required.
Increased ferritin levels
This is typically defined as >
300 µg/L in men/postmenopausal women and > 200 µµg/L in premenopausal women.
Ferritin is an acute phase protein
and may be synthesised in increased quantities in situations where inflammatory
activity is ongoing. Falsely elevated results may therefore be encountered
clinically and need to be taken in the context of the clinical picture and
blood results.
We can split the causes of
increased ferritin levels into 2 distinct categories;
|
Without
iron overload (around 90% of patients) |
With iron overload (around 10% of
patients) |
|
Inflammation (due to ferritin being an acute
phase reactant) Alcohol excess Liver disease Chronic kidney disease Malignancy |
Primary iron overload (hereditary
haemochromatosis) Secondary iron overload (e.g. following
repeated transfusions) |
The best test to see whether iron
overload is present is transferrin
saturation. Typically, normal values of < 45% in females and
< 50% in males exclude iron overload.
Reduced ferritin levels
Because iron and ferritin are bound
the total body ferritin levels may be decreased in cases of iron deficiency
anaemia.
Measurement of serum ferritin
levels can be useful in determining whether an apparently low haemoglobin and
microcytosis is truly caused by an iron deficiency state.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Gastric cancer
There are 700,000 new cases of
gastric cancer worldwide each year.
Epidemiology
·
overall incidence is decreasing, but incidence of tumours
arising from the cardia is increasing
·
peak age = 70-80 years
·
more common in Japan, China, Finland and Colombia than the West
·
more common in males, 2:1
Histology
·
signet ring cells may be seen in gastric cancer. They contain a
large vacuole of mucin which displaces the nucleus to one side. Higher numbers
of signet ring cells are associated with a worse prognosis
Associations
·
H. pylori infection
·
blood group A: gAstric cAncer
·
gastric adenomatous polyps
·
pernicious anaemia
·
smoking
·
diet: salty, spicy, nitrates
·
may be negatively associated with duodenal ulcer
Features
·
dyspepsia
·
nausea and vomiting
·
anorexia and weight loss
·
dysphagia
Investigation
·
diagnosis: endoscopy with biopsy
·
staging: CT or endoscopic ultrasound - endoscopic ultrasound has
recently been shown to be superior to CT
Surgical aspects
There is some evidence of support a
stepwise progression of the disease through intestinal metaplasia progressing
to atrophic gastritis and subsequent dysplasia, through to cancer. The favoured
staging system is TNM. The risk of lymph node involvement is related to size
and depth of invasion; early cancers confined to submucosa have a 20% incidence
of lymph node metastasis. Tumours of the gastro-oesophageal junction are
classified as below:
|
Type
1 |
True
oesophageal cancers and may be associated with Barrett's oesophagus. |
|
Type
2 |
Carcinoma
of the cardia, arising from cardiac type epithelium or
short segments with intestinal metaplasia at the oesophagogastric junction. |
|
Type
3 |
Sub
cardial cancers that spread across the junction. Involve similar nodal
stations to gastric cancer. |
|
|
|
|
Image
sourced from Wikipedia |
|

Upper GI endoscopy performed for dyspepsia. The addition
of dye spraying (as shown in the bottom right) may facilitate identification of
smaller tumours
Staging
·
CT scanning of the chest abdomen and pelvis is the routine first
line staging investigation in most centres.
·
Laparoscopy to identify occult peritoneal disease
·
PET CT (particularly for junctional tumours)
Treatment
·
Proximally sited disease greater than 5-10cm from the OG
junction may be treated by sub total gastrectomy
·
Total gastrectomy if tumour is <5cm from OG junction
·
For type 2 junctional tumours (extending into oesophagus)
oesophagogastrectomy is usual
·
Endoscopic sub mucosal resection may play a role in early
gastric cancer confined to the mucosa and perhaps the sub mucosa (this is
debated)
·
Lymphadenectomy should be performed. A D2 lymphadenectomy is
widely advocated by the Japanese, the survival advantages of extended
lymphadenectomy have been debated. However, the overall recommendation is that
a D2 nodal dissection be undertaken.
·
Most patients will receive chemotherapy either pre or post
operatively.
Prognosis
UK Data
|
Disease
extent |
Percentage 5 year survival |
|
All RO resections |
54% |
|
Early gastric cancer |
91% |
|
Stage 1 |
87% |
|
Stage 2 |
65% |
|
Stage 3 |
18% |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Gilbert's syndrome
Gilbert's syndrome is an autosomal recessive* condition of defective bilirubin conjugation due to a deficiency of UDP
glucuronosyltransferase. The prevalence is approximately
1-2% in the general population.
Features
·
unconjugated hyperbilirubinaemia (i.e. not in urine)
·
jaundice may only be seen during an intercurrent
illness, exercise or fasting
Investigation and management
·
investigation: rise in bilirubin following prolonged fasting or
IV nicotinic acid
·
no treatment required
*the exact mode of inheritance is
still a matter of debate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Haemochromatosis: features
Haemochromatosis is an autosomal recessive disorder of iron absorption and metabolism resulting in iron
accumulation. It is caused by inheritance of mutations in the HFE gene on both
copies of chromosome
6*. It is often asymptomatic in early disease and initial
symptoms often non-specific e.g. lethargy and arthralgia
Epidemiology
·
1 in 10 people of European descent carry a mutation in the genes
affecting iron metabolism, mainly HFE
·
prevalence in people of European descent = 1 in 200, making it more common than cystic fibrosis
Presenting features
·
early symptoms include fatigue, erectile
dysfunction and arthralgia (often of the hands)
·
'bronze' skin pigmentation
·
diabetes mellitus
·
liver: stigmata of chronic liver disease, hepatomegaly,
cirrhosis, hepatocellular deposition)
·
cardiac failure (2nd to dilated cardiomyopathy)
·
hypogonadism (2nd to cirrhosis and pituitary dysfunction -
hypogonadotrophic hypogonadism)
·
arthritis (especially of the hands)
Questions have previously been
asked regarding which features are reversible with treatment:
|
Reversible
complications |
Irreversible complications |
|
·
Cardiomyopathy ·
Skin pigmentation |
·
Liver cirrhosis** ·
Diabetes mellitus ·
Hypogonadotrophic hypogonadism ·
Arthropathy |
*there are rare cases of families
with classic features of genetic haemochromatosis but no mutation in the HFE
gene
**whilst elevated liver function
tests and hepatomegaly may be reversible, cirrhosis is not
From <https://www.passmedicine.com/review/textbook.php?s=#>
Commonly C282Y or H63D mutations HFE gene
MRI liver heart
Iron studies >50% transferrin sats
Venesection aim <100 ferritin
Refer to liver/endochronology
24 December 2020
14:15
Hepatorenal syndrome: management
The management of hepatorenal
syndrome (HRS) is notoriously difficult. The ideal treatment is liver
transplantation but patients are often too unwell to have surgery and there is
a shortage of donors
The most accepted theory regarding
the pathophysiology of HRS is that vasoactive mediators cause splanchnic vasodilation which in turn reduces the systemic vascular resistance. This
results in 'underfilling' of the kidneys. This is sensed by the juxtaglomerular
apparatus which then activates the renin-angiotensin-aldosterone system,
causing renal vasoconstriction which is not enough to counterbalance the
effects of the splanchnic vasodilation.
Hepatorenal syndrome has been
categorized into two types:
|
Type
1 HRS |
Type 2 HRS |
|
Rapidly progressive Doubling of serum creatinine to >
221 µmol/L or a halving of the creatinine clearance to less than 20 ml/min
over a period of less than 2 weeks Very poor prognosis |
Slowly progressive Prognosis poor, but patients may live
for longer |
Management options
·
vasopressin analogues, for example terlipressin, have a growing
evidence base supporting their use. They work by causing vasoconstriction of
the splanchnic circulation
·
volume expansion with 20% albumin
·
transjugular intrahepatic portosystemic shunt
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Irritable bowel syndrome: management
The management of irritable bowel
syndrome (IBS) is often difficult and varies considerably between patients.
NICE updated it's guidelines in 2015.
First-line pharmacological
treatment - according to predominant symptom
·
pain: antispasmodic agents
·
constipation: laxatives but avoid lactulose
·
diarrhoea: loperamide is first-line
For patients with constipation who
are not responding to conventional laxatives linaclotide may be considered, if:
·
optimal or maximum tolerated doses of previous laxatives from
different classes have not helped and
·
they have had constipation for at least 12 months
Second-line pharmacological
treatment
·
low-dose tricyclic antidepressants (e.g. amitriptyline 5-10 mg)
are used in preference to selective serotonin reuptake inhibitors
Other management options
·
psychological interventions - if symptoms do not respond to
pharmacological treatments after 12 months and who develop a continuing symptom
profile (refractory IBS), consider referring for cognitive behavioural therapy,
hypnotherapy or psychological therapy
·
complementary and alternative medicines: 'do not encourage use
of acupuncture or reflexology for the treatment of IBS'
General dietary advice
·
have regular meals and take time to eat
·
avoid missing meals or leaving long gaps between eating
·
drink at least 8 cups of fluid per day, especially water or
other non-caffeinated drinks such as herbal teas
·
restrict tea and coffee to 3 cups per day
·
reduce intake of alcohol and fizzy drinks
·
consider limiting intake of high-fibre food (for example,
wholemeal or high-fibre flour and breads, cereals high in bran, and whole
grains such as brown rice)
·
reduce intake of 'resistant starch' often found in processed
foods
·
limit fresh fruit to 3 portions per day
·
for diarrhoea, avoid sorbitol
·
for wind and bloating consider increasing intake of oats (for
example, oat-based breakfast cereal or porridge) and linseeds (up to one
tablespoon per day).
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Malnutrition
Malnutrition is an important
consequence of and contributor to chronic disease. It is clearly a complex and
multifactorial problem that can be difficult to manage but there are a number
of key points to remember for the exam.
NICE define malnutrition as the
following:
·
a Body Mass Index (BMI) of less than 18.5; or
·
unintentional weight loss greater than 10% within the last 3-6
months; or
·
a BMI of less than 20 and unintentional weight loss greater than
5% within the last 3-6 months
Around 10% of patients aged over 65
years are malnourished, the vast majority of those living independently, i.e.
not in hospital or care/nursing homes.
Screening for malnutrition if
mostly done using MUST (Malnutrition Universal Screen Tool). A link is provided
to a copy of the MUST score algorithm.
·
it should be done on admission to care/nursing homes and
hospital, or if there is concern. For example an elderly, thin patient with
pressure sores
·
it takes into account BMI, recent weight change and the presence
of acute disease
·
categorises patients into low, medium and high risk
Management of malnutrition is
difficult. NICE recommend the following points:
·
dietician support if the patient is high-risk
·
a 'food-first' approach with clear instructions (e.g. 'add
full-fat cream to mashed potato'), rather than just prescribing oral
nutritional supplements (ONS) such as Ensure
·
if ONS are used they should be taken between meals, rather than
instead of meals
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Melanosis coli
Melanosis coli is a disorder of
pigmentation of the bowel wall. Histology demonstrates pigment-laden
macrophages
It is associated with laxative
abuse, especially anthraquinone compounds such as senna
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Pyogenic liver abscess
The most common organisms found in
pyogenic liver abscesses are Staphylococcus
aureus in children and Escherichia coli in adults.
Management
·
drainage (typically percutaneous) and
antibiotics
·
amoxicillin + ciprofloxacin + metronidazole
·
if penicillin allergic: ciprofloxacin + clindamycin
|
|
|
|
©
Image used on license from Radiopaedia |
|
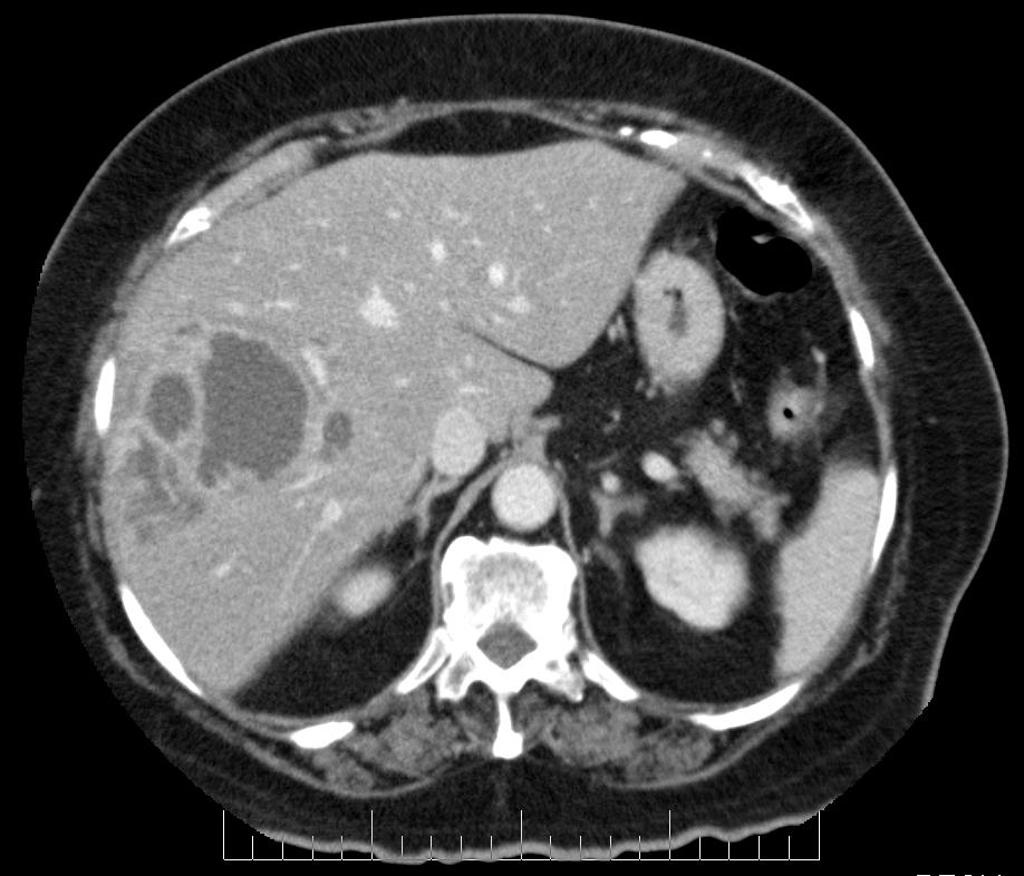
CT showing a pyogenic liver abscess in the right lobe of
the liver.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Refeeding syndrome
Refeeding syndrome describes the
metabolic abnormalities which occur on feeding a person following a period of
starvation. It occurs when an extended
period of catabolism ends abruptly with switching to carbohydrate metabolism. The metabolic consequences include:
·
hypophosphataemia
·
hypokalaemia
·
hypomagnesaemia: may predispose to torsades
de pointes
·
abnormal fluid balance
These abnormalities can lead to
organ failure.
Prevention
NICE produced guidelines in 2006 on
nutritional support. Refeeding syndrome may avoided by identifying patients at
a high-risk of developing refeeding syndrome:
Patients are considered high-risk
if one or more of the following:
·
BMI < 16 kg/m2
·
unintentional weight loss >15% over 3-6 months
·
little nutritional intake > 10 days
·
hypokalaemia, hypophosphataemia or hypomagnesaemia prior to
feeding (unless high)
If two or more of the following:
·
BMI < 18.5 kg/m2
·
unintentional weight loss > 10% over 3-6 months
·
little nutritional intake > 5 days
·
history of: alcohol abuse, drug therapy including insulin,
chemotherapy, diuretics and antacids
NICE recommend that if a patient
hasn't eaten for > 5 days, aim to re-feed at no more than 50% of
requirements for the first 2 days.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Scoring systems for liver cirrhosis
For many years the Child-Pugh classification was used to classify the severity of liver
cirrhosis. However, in recent years the Model for End-Stage Liver
Disease (MELD) has been increasingly used,
particularly patient's who are on a liver transplant waiting list
Child-Pugh classification
|
Score |
1 |
2 |
3 |
|
Bilirubin (µmol/l) |
<34 |
34-50 |
>50 |
|
Albumin (g/l) |
>35 |
28-35 |
<28 |
|
Prothrombin time, prolonged by (s) |
<4 |
4-6 |
>6 |
|
Encephalopathy |
none |
mild |
marked |
|
Ascites |
none |
mild |
marked |
Summation of the scores allows the
severity to be graded either A, B or C:
·
< 7 = A
·
7-9 = B
·
> 9 = C
MELD
Uses a combination of a patient's
bilirubin, creatinine, and the international normalized ratio (INR) to predict
survival. A formula is used to calculate the score:
MELD = 3.78×ln[serum bilirubin
(mg/dL)] + 11.2×ln[INR] + 9.57×ln[serum creatinine (mg/dL)] + 6.43
The 3-month mortality based on MELD
scores:
·
40 or more: 71.3% mortality
·
30 - 39: 52.6% mortality
·
20 - 29: 19.6% mortality
·
10 - 19: 6.0% mortality
·
< 9: 1.9% mortality
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Vitamin C deficiency (scurvy)
Vitamin C (ascorbic acid) is found
in citrus fruits, tomatoes, potatoes, Brussel sprouts, cauliflower, broccoli,
cabbage and spinach. Deficiency (commonly called scurvy) leads to impaired collagen synthesis and disordered connective tissue as ascorbic acid is a cofactor for
enzymes used in the production of proline and lysine. It is associated with severe malnutrition as well as drug and
alcohol abuse, and those living in poverty with limited access to fruits and
vegetables.
Symptoms and signs include:
·
Follicular hyperkeratosis and perifollicular haemorrhage
·
Ecchymosis, easy bruising
·
Poor wound healing
·
Gingivitis with bleeding and receding gums
·
Sjogren's syndrome
·
Arthralgia
·
Oedema
·
Impaired wound healing
·
Generalised symptoms such as weakness, malaise, anorexia and
depression
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Abdominal incisions
|
Midline
incision |
·
Commonest
approach to the abdomen ·
Structures
divided: linea alba, transversalis fascia, extraperitoneal fat, peritoneum
(avoid falciform ligament above the umbilicus) ·
Bladder can
be accessed via an extraperitoneal approach through the space of Retzius |
|
Paramedian
incision |
·
Parallel to
the midline (about 3-4cm) ·
Structures
divided/retracted: anterior rectus sheath, rectus (retracted), posterior
rectus sheath, transversalis fascia, extraperitoneal fat, peritoneum ·
Incision is
closed in layers |
|
Battle |
·
Similar
location to paramedian but rectus displaced medially (and thus denervated) ·
Now seldom
used |
|
Kocher's |
Incision
under right subcostal margin e.g. Cholecystectomy (open) |
|
Lanz |
Incision
in right iliac fossa e.g. Appendicectomy |
|
Gridiron |
Oblique
incision centered over McBurneys point- usually appendicectomy (less
cosmetically acceptable than Lanz |
|
Gable |
Rooftop
incision |
|
Pfannenstiel's |
Transverse
supra pubic, primarily used to access pelvic organs |
|
McEvedy's |
Groin
incision e.g. Emergency repair strangulated femoral hernia |
|
Rutherford
Morrison |
Extraperitoneal
approach to left or right lower quadrants. Gives excellent access to iliac
vessels and is the approach of choice for first time renal transplantation. |
|
|
|
|
Image
sourced from Wikipedia |
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Antidiarrhoeal agents
Opioid agonists include
·
loperamide
·
diphenoxylate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Bile-acid malabsorption
Bile-acid malabsorption is a cause
of chronic diarrhoea. This may be primary, due to excessive production of bile
acid, or secondary to an underlying gastrointestinal disorder causing reduced
bile acid absorption. It can lead to steatorrhoea and vitamin A, D, E, K malabsorption.
Secondary causes are often seen in
patients with ileal disease, such as with Crohn's. Other secondary causes
include:
·
cholecystectomy
·
coeliac disease
·
small intestinal bacterial overgrowth
Investigation
·
the test of choice is SeHCAT
·
nuclear medicine test using a gamma-emitting selenium molecule
in selenium homocholic acid taurine or tauroselcholic acid (SeHCAT)
·
scans are done 7 days apart to assess the retention/loss
of radiolabelled 75SeHCAT
Management
·
bile acid sequestrants e.g. cholestyramine
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Bilirubin
Bilirubin is a chemical by-product
of the breakdown
of heme, a component of red blood cells, and other hepatic
heme-containing proteins, for example, myoglobin. The released heme is
processed within macrophages and oxidized to form biliverdin and iron. Biliverdin
is then reduced to form unconjugated bilirubin, which is released into the
bloodstream.
Unconjugated bilirubin is bound to
albumin in the blood and then taken up by hepatocytes, where it is conjugated,
thus rendering it water-soluble. From hepatocytes, it is excreted into bile and
thus enters the intestines to be broken down by intestinal bacteria. Bacterial
proteases produce urobilinogen from bilirubin within the intestinal lumen, the
majority of which is further processed by intestinal bacteria to form urobilin
and stercobilin and excreted via the faeces. Around 10% of the bilirubin
entering the intestinal system re-enters the portal circulation to be finally
excreted via the kidneys in urine.
Raised levels of unconjugated
bilirubin may occur as a result of haemolysis, which is to say a pre-hepatic
source, for example, autoimmune-mediated haemolytic anaemia. Red blood cell
breakdown exposes heme-containing proteins and, as discussed above, these are
then processed to form unconjugated bilirubin.
Hepatocyte defects, such as a
compromised hepatocyte uptake of unconjugated bilirubin and/or defective
conjugation may occur in liver disease, or deficiency of glucuronyl
transferase.
A mild glucuronyl transferase
deficiency results in Gilbert's Syndrome, whilst a moderate to severe
glucuronyl transferase deficiency may be seen in Crigler-Najjar Syndrome types
I and II respectively. A transient glucuronyl transferase deficiency may also
contribute to physiological neonatal jaundice.
Raised levels of conjugated
bilirubin can result from defective excretion of bilirubin, for example,
Dubin-Johnson Syndrome, or cholestasis.
Jaundice starts to appear when
bilirubin reaches an excess of 35umol/l.
Cholestasis can result from a wide
range of pathologies, which can be largely divided into physical causes, for
example, gallstones, pancreatic and cholangiocarcinoma, or functional causes,
for example, drug-induced, pregnancy-related and post-operative cholestasis.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:15
Constipation
Constipation is a common primary
functional disorder of the bowel but may, of course, develop secondary to
another condition. It may be defined as defecation that is unsatisfactory
because of infrequent stools (< 3 times weekly), difficult stool passage
(with straining or discomfort), or seemingly incomplete defecation.
Features
·
the passage of infrequent hard stools
Complications
·
overflow diarrhoea
·
acute urinary retention
·
haemorrhoids
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Diverticulosis
Diverticulosis is an extremely
common disorder characterised by multiple outpouchings of the bowel wall, most
commonly in the sigmoid colon. Strictly speaking the term diverticular disease
is reserved for patients who are symptomatic - diverticulosis is the more accurate term for diverticula being present.
Risk factors
·
increasing age
·
low-fibre diet
Diverticulosis can present in a
number of ways:
·
painful diverticular disease: altered bowel habit, colicky left
sided abdominal pain. A high fibre diet is usually recommended to minimise
symptoms
·
diverticulitis: see below for more details
Diverticulitis
One of the diverticular become
infected. The classical presentation is:
·
left iliac fossa pain and tenderness
·
anorexia, nausea and vomiting
·
diarrhoea
·
features of infection (pyrexia, raised WBC and CRP)
Management:
·
mild attacks can be treated with oral antibiotics
·
more significant episodes are managed in hospital. Patients are
made nil by mouth, intravenous fluids and intravenous antibiotics (typical a
cephalosporin + metronidazole) are given
Complications of diverticulitis
include:
·
abscess formation
·
peritonitis
·
obstruction
·
perforation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Gastro-oesophageal reflux disease: investigation
Overview
·
poor correlation between symptoms and endoscopy appearance
Indications for upper GI endoscopy:
·
age > 55 years
·
symptoms > 4 weeks or persistent symptoms despite treatment
·
dysphagia
·
relapsing symptoms
·
weight loss
If endoscopy is negative consider
24-hr oesophageal pH monitoring (the gold standard test for diagnosis)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Gastro-oesophageal reflux disease: management
Gastro-oesophageal reflux disease
(GORD) may be defined as symptoms of oesophagitis secondary to refluxed gastric
contents
NICE recommend that GORD which has
not been investigated with endoscopy should be treated as per the dyspepsia
guidelines
Endoscopically proven oesophagitis
·
full dose proton pump inhibitor (PPI) for 1-2 months
·
if response then low dose treatment as required
·
if no response then double-dose PPI for 1 month
Endoscopically negative reflux
disease
·
full dose PPI for 1 month
·
if response then offer low dose treatment, possibly on an
as-required basis, with a limited number of repeat prescriptions
·
if no response then H2RA or prokinetic for one month
Complications
·
oesophagitis
·
ulcers
·
anaemia
·
benign strictures
·
Barrett's oesophagus
·
oesophageal carcinoma
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Hepatitis D
Hepatitis D is a single stranded
RNA virus that is transmitted parenterally. It is an incomplete RNA virus that
requires hepatitis B surface antigen to complete its replication and
transmission cycle.
It is transmitted in a similar
fashion to hepatitis B (exchange of bodily fluids) and patients may be infected
with hepatitis B and hepatitis D at the same time.
Hepatitis D terminology:
·
Co-infection: Hepatitis B and Hepatitis D infection at the same
time.
·
Superinfection: A hepatitis B surface antigen positive patient
subsequently develops a hepatitis D infection.
Superinfection is associated with
high risk of fulminant hepatitis, chronic hepatitis status and cirrhosis.
Diagnosis is made via reverse
polymerase chain reaction of hepatitis D RNA. Interferon is currently used as
treatment, but with a poor evidence base.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Inferior mesenteric artery
The IMA is the main arterial supply
of the embryonic hindgut and originates approximately 3-4 cm superior to the
aortic bifurcation. From its aortic origin it passes immediately inferiorly
across the anterior aspect of the aorta to eventually lie on its left hand
side. At the level of the left common iliac artery it becomes the superior
rectal artery.
Branches
The left colic artery arises from
the IMA near its origin. More distally up to three sigmoid arteries will exit
the IMA to supply the sigmoid colon.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Iron studies
Serum iron
Total iron
binding capacity (TIBC)
·
transferrin
·
raised in iron deficiency anaemia (IDA)
·
raised in pregnancy and by oestrogen
Transferrin saturation
·
calculated by serum iron / TIBC
Ferritin
·
raised in inflammatory disorders
·
low in IDA
Rarer tests
·
transferrin receptors increased in IDA
Anaemia of chronic disease
·
normochromic/hypochromic, normocytic anaemia
·
reduced serum and TIBC
·
normal or raised ferritin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Irritable bowel syndrome
NICE published clinical guidelines
on the diagnosis and management of irritable bowel syndrome (IBS) in 2008
The diagnosis of IBS should be
considered if the patient has had the following for at least 6 months:
·
abdominal pain, and/or
·
bloating, and/or
·
change in bowel habit
A positive diagnosis of IBS should
be made if the patient has abdominal pain relieved by defecation or associated
with altered bowel frequency stool form, in addition to 2 of the following 4
symptoms:
·
altered stool passage (straining, urgency, incomplete
evacuation)
·
abdominal bloating (more common in women than men), distension,
tension or hardness
·
symptoms made worse by eating
·
passage of mucus
Features such as lethargy, nausea,
backache and bladder symptoms may also support the diagnosis
Red flag features should be
enquired about:
·
rectal bleeding
·
unexplained/unintentional weight loss
·
family history of bowel or ovarian cancer
·
onset after 60 years of age
Suggested primary care
investigations are:
·
full blood count
·
ESR/CRP
·
coeliac disease screen (tissue transglutaminase antibodies)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Peptic ulcer disease (perforation)
The symptoms of perforation
secondary to peptic ulcer disease typically develop suddenly
·
epigastric pain, later becoming more generalised
·
patients may describe syncope
Investigations
·
Although the diagnosis is largely clinical, UptoDate recommend
that plain x-rays are the first form of imaging to obtain
·
An upright ('erect') chest x-ray is usually required when a patient
presents with acute upper abdominal pain
·
This is a useful test, as approximately 75% of patients with a
perforated peptic ulcer will have free air under the diaphragm
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Pernicious anaemia
Pernicious anaemia is an autoimmune
disorder affecting the gastric mucosa that results in vitamin B12 deficiency.
It is helpful to remember that pernicious means 'causing harm, especially in a gradual or
subtle way' - the symptoms of signs are often subtle and diagnose
is often delayed.
Whilst pernicious anaemia is the most
common cause of vitamin B12 deficiency, it's not the only cause. Other
causes include atrophic gastritis (e.g. secondary to H. pylori infection), gastrectomy, malnutrition (e.g. alcoholism).
Pathophysiology
·
antibodies to intrinsic factor +/- gastric parietal cells
o intrinsic factor antibodies → bind
to intrinsic factor blocking the vitamin B12 binding site
o gastric parietal cell antibodies →
reduced acid production and atrophic gastritis. Reduced intrinsic factor
production → reduced vitamin B12 absorption
·
vitamin B12 is important in both the production of blood cells
and the myelination of nerves → megaloblastic anaemia and
neuropathy
Risk factors
·
more common in females (F:M = 1.6:1) and typically develops in
middle to old age
·
associated with other autoimmune disorders: thyroid disease, type 1 diabetes
mellitus, Addison's, rheumatoid and vitiligo
·
more common if blood group A
Features
·
anaemia features
o lethargy
o pallor
o dyspnoea
·
neurological features
o peripheral neuropathy: 'pins and
needles', numbness. Typically symmetrical and affects the legs more than the
arms
o subacute combined degeneration of
the spinal cord: progressive weakness, ataxia and paresthesias that may
progress to spasticity and paraplegia
o neuropsychiatric features: memory
loss, poor concentration, confusion, depression, irritabiltiy
·
other features
o mild jaundice: combined with pallor
results in a 'lemon tinge'
o glossitis → sore tongue
Investigation
·
full blood count
o macrocytic anaemia: macrocytosis
may be absent in around of 30% of patients
o hypersegmented polymorphs on blood
film
o low WCC and platelets may also be
seen
·
vitamin B12 and folate levels
o a vitamin B12 level of >= 200
nh/L is generally considered to be normal
·
antibodies
o anti intrinsic factor antibodies:
sensivity is only 50% but highly specific for pernicious anaemia (95-100%)
o anti gastric parietal cell
antibodies in 90% but low specificity so often not useful clinically
·
Schilling test is no longer routinely done
o radiolabelled B12 given on two
occasions, firstly on its own, secondly with oral IF. Urine B12 levels are then
measured
Management
·
vitamin B12 replacement
o usually given intramuscularly
o no neurological features: 3 injections per week for 2 weeks followed by 3 monthly treatment
of vitamin B12 injections
o more frequent doses are given for
patients with neurological features
o there is some evidence that oral
vitamin B12 may be effective for providing maintenance levels of vitamin B12
but it is not yet common practice
·
folic acid supplementation may also be required
Complications other than the
haematological and neurological features detailed above
·
increased risk of gastric cancer
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Vitamin A (retinol)
Vitamin A is a fat soluble vitamin.
Functions
·
converted into retinal, an important visual pigment
·
important in epithelial cell differentiation
·
antioxidant
Consequences of vitamin A
deficiency
·
night blindness
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Vitamin B3 (niacin)
Niacin is a water soluble vitamin
of the B complex group. It is a precursor to NAD+ and NADP+ and hence plays an
essential metabolic role in cells.
Biosynthesis
·
Hartnup's disease: hereditary disorder which reduces absorption
of tryptophan
·
carcinoid syndrome: increased tryptophan metabolism to serotonin
Consequences of niacin deficiency:
·
pellagra: dermatitis, diarrhoea, dementia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Vitamin B6 (pyridoxine)
Vitamin B6 is a water soluble
vitamin of the B complex group. It is converted to pyridoxal phosphate (PLP)
which is a cofactor for many reactions including transamination, deamination
and decarboxylation.
Causes of vitamin B6 deficiency
·
isoniazid therapy
Consequences of vitamin B6
deficiency
·
peripheral neuropathy
·
sideroblastic anemia
|
|
|
|
|
|

Diagram showing the biochemical role of vitamin B12 and
vitamin B6
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Vitamin C (ascorbic acid)
Vitamin C is a water soluble
vitamin.
Functions
·
antioxidant
·
collagen synthesis: acts as a cofactor for enzymes that are
required for the hydroxylation proline and lysine in the synthesis of collagen
·
facilitates iron absorption
·
cofactor for norepinephrine synthesis
Vitamin C deficiency (scurvy) leads
to defective synthesis of collagen resulting in capillary fragility (bleeding
tendency) and poor wound healing
Features vitamin C deficiency
·
gingivitis, loose teeth
·
poor wound healing
·
bleeding from gums, haematuria, epistaxis
·
general malaise
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
14:16
Zollinger-Ellison syndrome
Zollinger-Ellison syndrome is
condition characterised by excessive levels of gastrin, usually from a gastrin
secreting tumour usually of the duodenum or pancreas. Around 30% occur as part
of MEN type I syndrome
Features
·
multiple gastroduodenal ulcers
·
diarrhoea
·
malabsorption
Diagnosis
·
fasting gastrin levels: the single best screen test
·
secretin stimulation test
From <https://www.passmedicine.com/review/textbook.php?s=#>
Liver function tests
04 January 2021
23:14
|
|
|||
|
|
ALP (Isolated) is
physiologically raised in the 3rd trimester of pregnancy plasma half-life of
prothrombin factor 7 is approximately
6 hours 90% of Liver disease is
preventable, with three quarters of people being diagnosed at a late stage. Where Transferases (ALT/AST) >> ALP and GGT ·
Consider
a Hepatic cause Where ALP and GGT >> Transferases (ALT/AST) ·
Consider
a Biliary / Obstructive cause A standardised
serum liver function test usually includes: Bilirubin Albumin Transferases (alanine
transferase (ALT); aspartate transferase (AST) Alkaline phosphatase (ALP) Gamma Glutamyltransferase (GGT) On some testing panels GGT and
AST have to been added on in addition to the
standard panel. It is also
useful to include a serum coagulation or INR when assessing liver function Bilirubin is
formed by the breakdown of haemoglobin within the reticuloendothelial system.
This forms unconjugated bilirubin, which is water-insoluble
and therefore needs to be bound to albumin, where it is taken up
by the liver. In the Liver bilirubin is conjugated to
make it water-soluble. The majority of Conjugated bilirubin is
excreted as bile acid via the bile ducts of the Liver. It is stored within
the gallbladder and released into the small intestine where it aids in the
breakdown of lipids. 95% of bile is reabsorbed in the terminal ileum to
the Entrohepatic circulation. From <https://mle.ncl.ac.uk/cases/page/16351/>
In general the total serum bilirubin is usually measured, but
you can measure both the indirect (unconjugated) and direct
(conjugated) portions. The normal range is usually <21umol/L |
||
|
|
|
||
|
|

Unconjugated
bilirubin
This
usually is elevated due to increased
bilirubin production OR decreased hepatic
uptake/conjugation:
The
commonest causes of raised unconjugated bilirubin in adults are:
·
Gilbert’s syndrome:
o A genetic disorder where less of the enzyme
that breaks down Bilirubin (UDP-glucuronyltransferase) is produced. It affects
5% of the population. There is an increase in the bilirubin often with fasting
or concurrent illness.
o Confirmation of just a predominant
unconjugated hyperbilirubinaemia makes the diagnosis of Gilbert’s syndrome
virtually certain. This does not require any treatment and the patient can be
completely reassured.
o Rarely does it cause a bilirubin above
68umol/L
·
Haemolysis:
o The breakdown of red blood cells. There can by
many causes for this and standard investigations for this would include:
reticulocyte count, LDH, blood film, Haptoglobin, Direct coombs test
·
Drug related, for
example, the antibiotic Rifampicin impairs the uptake of Bilirubin
Conjugated
Bilirubin
In
healthy adults conjugated bilirubin is virtually absent. Levels usually start
to become increased when the liver has lost approximately ½ of its excretory
capacity. It is therefore usually a sign of liver disease, which may be acute
or chronic in nature.
Common
causes for elevated conjugated bilirubin include:
·
Biliary obstruction at
any level of the bile ducts
o Often secondary to gallstones in the common
bile duct, but also from malignancy – commonly Cholangiocarcinoma or Pancreatic
cancer
·
Cholestatic drug
reactions
o Potentially any drug, but commonly antibiotics
such as Nitrofuratoin and Penicillin
·
Autoimmune Cholestatic
disease e.g. Primary Sclerosing Cholangitis (may occur at any level) and
Primary Biliary Cirrhosis (intrahepatic ducts)
·
Hepatitis of any
origin where there is significant impairment in liver function
·
Cirrhosis
ALT and AST
Alanine
aminotransferase (ALT) or aspartate
aminotransferase (AST) is measured in a liver function test profile. Both
these enzymes live predominately in hepatocytes, whilst AST may also be found
diffusely in cardiac and skeletal muscle, renal tissue, along with red blood
cells. This means that ALT is in general more specific to the liver.
Injury
to the liver, whether acute or chronic, will cause inflammation or damage to
hepatocytes (but not necessarily cell death), leading to a release of these
enzymes into the blood stream and resulting in a measureable increase in serum
concentration of aminotransferases.
Therefore
elevated transferase usually reflects a hepatitis of which there could be many
causes.
Common
causes of acute and chronic hepatitis are:
·
Alcohol – including
chronic alcohol abuse and Alcoholic hepatitis
·
Non-alcoholic fatty
liver disease (NAFLD)
·
Viral Hepatitis – both
acute and chronic
·
Autoimmune Hepatitis
·
Drug toxicity
·
Ischaemia – this can
be due to anything which suddenly causes a patient’s blood pressure to drop
·
Metabolic liver
disease (Wilson’s / Haemochromatosis)
Upper
limits may vary between labs and the units that are used, but normal is usually
considered to be less than 40IU/L.
There
is no internationally recognised criteria but generally rises in
aminotransferase can be thought as:
· Mild
(<5 upper limit of normal)
· Moderate
(5-10 upper limit of normal)
· Marked
(> 10 upper limit of normal)
The
degree of rise in transferase can help guide the underlying aetiology, although
there is often significant overlap.
The diagram below illustrates the degree of
ALT rise with associated disease.

A
useful rule of thumb is that an ALT rise of greater than 1,000 IU/L reflects a
significant acute liver injury and is typically only caused by the following:
·
Ischaemia
·
Drugs (Most commonly
Paracetamol)
·
Viruses (Hepatitis A,
B, C and E)
Examining
the ratio of AST to ALT can also be helpful in determining the underlying
cause. In alcohol related liver disease patients are often nutritionally
deficient in vitamin B6. This effects the activity of ALT, resulting in reduced
concentrations, thus typically resulting in an AST/ALT ratio of >2 in
alcoholic liver disease; whilst an AST/ALT ratio of <1.0 would be more
suggestive of non-alcoholic liver disease.
The
circulation half-life for ALT is around 47 hours.
From <https://mle.ncl.ac.uk/cases/page/16748/>
ALP
Alkaline
phosphatase (ALP) is another enzyme, but which predominately comes from cells
that line the biliary tract, however it is also present in bone and the
placenta. Therefore it may be elevated physiologically or pathologically.
A
normal ALP is generally <130 IU/L
Physiological
causes include:
·
3rd Trimester of
pregnancy
·
Increase bone turnover
– adolescents during periods of growth
Pathological
causes include:
·
Hepatic:
o Bile duct obstruction – stones, malignancy
o Primary Sclerosing Cholangitis (PSC)
o Primary Biliary Cirrhosis (PBC)
o Drug induced cholestasis (antibiotics,
anabolic steroids)
·
Extra-hepatic:
o Bone disease: Factures, Pagets disease and
bone metastasis
GGT
The
enzyme Gamma-glutamyltransferase (GGT) is present in cell membranes of bile
ducts, gallbladder, kidneys, pancreas, spleen and heart. It may be raised in
all types of liver disease, however when paired with an elevated ALP it is
highly suggestive of hepatobiliary source.
A
normal GGT is usually < 70 unit/L
Isolated
ALP rises can and do occur in PSC and PBC. However you should also be alert for
other sources, in particular for bone metastasis. Isolated GGT is seen in
alcohol abuse, as well as COPD and renal failure.
Cholestasis
enhances the synthesis and release of ALP. The half-life of ALP is around a
week; therefore levels may rise quickly in bile duct obstruction and decrease
slowly following resolution.
Prothrombin
The
Prothrombin Time (PT) is a measure of the function of the extrinsic and common
coagulation pathways. It represents the time in seconds for the patient’s
plasma to clot after the addition of calcium and thromboplastin (an activator
in the extrinsic pathway). Another way to represent this is the
Internationalised Normalised Ratio, which standardises how the PT is measured -
difficult labs have different ways of measuring PT, meaning it is difficult to
compare PT’s across different laboratories.
The PT and
Internationalised Normalised Ratio (INR) are both useful for measuring Liver
synthetic function because clotting factors II, V, VII, IX, and X are produced
in the Liver. Therefore if the liver is not able to produce these
clotting factors due to dysfunction this is reflected in a prolonged PT/INR.

The PT/INR is particularly useful
in acute liver injury as factor VII has a short half-life – around 6 hours.
Therefore it is useful in acute or fulminant liver failure as a way to monitor
the progression of damage or impairment to the liver.
PT and INR may be
prolonged in chronic liver disease but not until approximately 80% of the
livers synthetic function is compromised. It is therefore a useful indicator of
advanced liver disease, particularly in decompensated liver cirrhosis and is
often included in prognostic scoring systems.
One important thing
to consider is that while a prolonged PT may indicate liver synthetic
dysfunction, it can be prolonged for other reasons. In particular deficiency in
fat-soluble vitamin k, which is used in the generation of factors II, VII, IX,
and X, can be responsible. This is
particularly true in cases of obstructive jaundice where reduced bile acid
excretion impairs intestinal absorption of fat-soluble vitamins.
Acute
liver failure (ALF) is loss of liver function at that occurs rapidly in days or
weeks in the absence of any underlying chronic liver disease. It is
characterized by jaundice, coagulopathy (prolonged PT/INR) and hepatic
encephalopathy. Hepatic Encephalopathy is essential to fulfil the
diagnosis of ALF.
ALF can
be further subdivided into Hyperacute, Acute or Subacute.
·
Hyperacute - Encephalopathy occurs within 7 days of
onset of jaundice
·
Acute
liver failure – 8 to 28 days
from jaundice to encephalopathy
·
Sub
acute failure - Hepatic
encephalopathy occurs within 5-12 weeks of onset of jaundice.
·
Severe
Acute liver injury – Elevated
transferases, prolonged PT and jaundice. But NO hepatic encephalopathy

In
chronic liver disease there is a duration of greater than 28 weeks before the
onset of hepatic encephalopathy.
Acute
on chronic liver disease, or decompensating liver disease share features of
acute liver failure clinically – we know that ¾ of patients present with
advanced liver disease, their first presentation may therefore be with
jaundice, coagulopathy and hepatic encephalopathy.
Clues
to suggest underlying chronic liver disease rely on a thorough clinical
assessment, which includes a full history. Clinical examination to look
for signs secondary to chronic liver disease is particularly helpful (see
later). Portal hypertension is more common in advanced chronic liver
disease (but may also occur in the acute setting), these may be evident
clinically, biochemically (Platelets < 150 due to hypersplenism) or radiologically.
From <https://mle.ncl.ac.uk/cases/page/16558/>
Consequences of portal hypertension include:
Oesophageal and Gastric Varices
Abdominal Ascites
Peripheral oedema
Hepatic Encephalopathy
Low Platelets (due to hypersplenism)
Antimitochondrial antibody - PBC
Anti-smooth
muscle antibody / anti LKM1 / Antinuclear antibody – Autoimmune Hepatitis
pANCA
– PSC
From <https://mle.ncl.ac.uk/cases/page/16583/>
Elevated IgA – often associated with fatty liver disease -such as
alcohol or NAFLD (Non-Alcoholic Fatty Liver Disease)
Elevated IgM – often associated with Primary Biliary Cirrhosis
Elevated IgG – often associated with Autoimmune Hepatitis
From <https://mle.ncl.ac.uk/cases/page/16583/>
¡ Serum ferritin and transferrin saturation – elevated in Haemochromatosis
¡ Copper/Caeruloplasmin – Wilson's disease
¡ Alpha-1 antitrypsin (A1AT) – Hereditary disorder
Alpha-fetoprotein
(AFP) – this should not form part of the
liver screen but instead is used in screening for Hepatocellular Carcinoma – a
common sequelae of Cirrhosis, and chronic Hepatitis B and C infection.
From <https://mle.ncl.ac.uk/cases/page/16583/>
Haemochromatosis
04 January 2021
23:52
Haemochromatosis
A
disorder that results in iron overload, which may affect many organs. There are
two types – primary and secondary.
Primary
An
inherited disorder, the most common being autosomal recessive caused by a
defect in the HFE gene, sometimes called HFE Haemochromatosis. It was thought
this was the only gene associated with Haemochromatosis, however it is now know
that there are other gene associations.
Haemochromatosis.org.uk
This is
the UK’s most common genetic condition.
The two
known mutations of HFE are C282Y and H63D. Testing for these is simple and
cheap. But there are other rare genes that may cause disease
Whilst
this is an autosomal recessive condition, clinically things can be a bit more
complex – this is because gene expression (penetrance) varies. E.g. just
because you have two copies of the defective gene does not mean you will
definitely develop the clinical condition.
·
C282Y/C282Y Homozygous
gives a 95% risk of iron overload
·
C282Y/H63D compound
heterozygotes gives around 4% risk (increased risk with increased alcohol
intake, viral hepatitis)
·
H63D/H63D Homozygous
is least likely to cause iron overload
All
these genes lead to increased intestinal absorption of iron.
Patients
are often identified incidentally due to abnormal liver tests (elevated ALT),
abnormal imaging (fatty liver, iron overload in liver) or elevated serum
ferritin (see later). They can present with vague symptoms or advanced
disease
The
main symptoms patients may present with are:
1.
Joint pain –
especially of the hands and fingers
2.
Fatigue
3.
Mood disorders –
depression / anxiety / mood swings
Other
symptoms include abdominal pain, palpations, shortness of breath, infertility,
hair loss and amenorrhoea.
These
symptoms usually appear later on in the disease – around age 40-60 in males,
and post menopausal for females.
Advanced
disease may present with diabetes, bronzing of the skin, hepatomegaly/cirrhosis
and arthropathy of the 2nd and 3rd metacarpophalangeal joints
If
there is genetic expression then this is likely to be reflected in elevated
serum ferritin and transferrin saturations.
Secondary
Iron
overload due to parental iron-overload e.g. multiple blood transfusions or IV
iron replacement. It can be from several haematological disorders e.g.
myelodysplastic syndrome
Serum
Ferritin (SF)
This is
a measurement of the protein ferritin in the blood. SF usually correlates well
with iron storage.
The
normal range males is 15-300 µg/l and females 15-200 µg/l
In
Haemochromatosis the ferritin is often (but not always) in 1000’s
It is
however important to note that ferritin can also be significantly raised in
those with chronic alcohol abuse or have NAFLD as part of the metabolic
syndrome. It is also an acute phase protein and can be raised in inflammatory
conditions and malignancy. Therefore an additional blood test called
transferrin saturations is also tested.
Transferrin
Saturation (TS)
A
glycoprotein that binds free iron in the bloodstream. When low it means that
there is not much iron available. Conversely when high it indicates that the
free iron levels are high.
The
normal range for males is 16-50%, for females this is 16-45%
Diagnosis
Patients
with elevated SF and T/S should undergo genetic screening for the above genes;
those with a ferritin greater than 1000 µg/l should be referred urgently to
secondary care to exclude Cirrhosis.
Liver
function tests, imaging such as ultrasound and/or fibroscan should be used to
assess degree of liver damage.
Diagnosis
of HFE Haemochromatosis should not be based on C282Y homozygosity. It requires
evidence of increased iron stores.
Those
with HFE genotype, but not gene expression, e.g. normal SF and TS should have
annual iron studies.
Treatment
There
are two main phases to treatment:
1. Acute iron removal – this is done
via venesection (approx. 450ml of blood is removed). This will reduce the SF by
approx. 20-25 µg/l. This is continued until SF are 50-100 µg/l.. Treatment may
be required for 12 to 18months, weekly to 2 weekly.
2. Maintenance phase – 2-4 venesections
a year to keep SF 50-100 µg/l
Some
symptoms may improve with venesection
Patients
with Cirrhosis and haemochromatosis are at a significant increased risk of
Hepatocellular Carcinoma and should be screened every 6 months with ultrasound
imaging and serum AFP.
Haemochromatosis.org.uk
A
patient with confirmed genetic haemochromatosis should be offered genetic
counselling and also genetic screening for any first-degree relatives –
siblings will have a ¼ chance of being homozygote. If the patient has children,
then assuming a patients partner does not carry the gene then any children will
be carriers.
From <https://mle.ncl.ac.uk/cases/page/16603/>
Wilson's disease
04 January 2021
23:53
Wilson’s
disease is a rare progressive genetic disorder, which results in accumulation
of copper in the body’s tissues. In particular it affects the brain, liver and
cornea of the eyes. Untreated it may lead to liver fibrosis and
cirrhosis, along with central nervous system dysfunction.
There
are 500 gene mutations known about. These result in dysfunction in Wilson’s
ATPase, which usually moves copper from along intracellular membranes in the
liver. The defective ATPase results in accumulation of copper in the liver,
resulting in damage. Over time as the liver becomes damaged the copper is
released into the blood and causes other end organ damage.
Damage
may begin to occur as early as age 6, but often does not become apparent until
teenage years (range 5 to 35).
Patients
may present with:
Liver
dysfunction (most common presentation):
· Decompensated liver cirrhosis
· Acute liver failure (often associated with
renal failure and haemolytic anaemia)
Central
nervous system (usually have established liver disease):
· Asymmetrical tremor in ½ patients with CNS
dysfunction
· Poor co-ordination and clumsiness
· Speech and language problems
· Neuropsychiatric illness – commonly severe
depression or neurotic behaviours
Ophthalmological
· Kayser-Fleischer ring present in 95% of those
with neurological disease (seen on slit-lamp), 50% of those without. May occur
in other diseases.
· Sun-flower cataracts – seen on slit lamp. Do not
impair vision
Diagnosis.
Consider
in any patient of any age with unusual liver or neurological abnormalities.
There is no one best test for diagnosis.
Presence
of Kayser-Felischer ring and low serum caeruloplasmin (<0.1g/L) is enough to
establish diagnosis.
Caeruloplasmin
is a protein made in the liver that stores and carries copper around the blood.
This may be low in Wilson’s as copper is not able to bind to the protein
causing instability. Serum Caeruloplasmin is can be affected by many factors
and is not diagnostic on it’s own.
Other
markers of disease include 24hour urinary copper, serum free copper and hepatic
copper (liver biopsy).
A
scoring system also exists to help with diagnosis.
Genetic
screening is complex, many patients are compound heterozygotes (carry two
different defective genes) and it can take many months to complete.
Treatment
Treatment
is life-long. It involves using medication to either promote urinary excretion
or to decrease intestinal absorption. The commonest medication used is
D-Penicillamine.
Genetics
are complex due to the number of gene variations, but essentially siblings (25%
risk) and any offspring (0.5% risk) should be offered genetic screening.
From <https://mle.ncl.ac.uk/cases/page/16604/>
SAAG serum to
ascites albumin gradient
05 January 2021
00:02
A serum
to ascites albumin gradient (SAAG) can help you differentiate the underlying
cause of ascites.
·
The serum-to-ascites
albumin gradient (SAAG) accurately identifies the presence of portal
hypertension and is more useful than the protein-based exudate/transudate
concept
·
The SAAG is easily
calculated by subtracting the ascitic fluid albumin value from the serum
albumin value, which should be obtained the same day. The SAAG generally does
not need to be repeated after the initial measurement.
·
The presence of a
gradient ≥11 g/L predicts that the patient has portal hypertension with 97
percent accuracy
·
This is due to
increased hydrostatic pressure within the blood vessels of the hepatic portal
system, which in turn forces water into the peritoneal cavity but leaves
proteins such as albumin within the vasculature.
·
A gradient <11 g/L
indicates that portal hypertension is not the primary cause of ascites
·
The following table
illustrates some different causes of ascites which are associated with a high
or low SAAG:

From <https://mle.ncl.ac.uk/cases/page/17267/>
Child Pugh score
05 January 2021
00:07
Child
Pugh score is a grading system of cirrhosis and risk of variceal bleeding,
ranging from 5-15. The grading can be used to predict mortality and quantify
need for liver transplantation. Risk of variceal bleeding is much higher if the
score is >8.
Mr
Wilson’s Child-Pugh score is 11, which means he has Child-Pugh class C
cirrhosis. This signifies he has a higher risk of variceal bleeding and higher
mortality rate (1 year survival is 45% compared with 100% & 80% for
Child-Pugh A & B respectively).
From <https://mle.ncl.ac.uk/cases/page/17271/>
Glasgow-Blatchford
score
05 January 2021
00:10
Glasgow-Blatchford
score. This is a prognostic score to assess the likelihood that Mr Wilson will
require an intervention such as endoscopy or blood transfusion following his
upper GI bleed.
Patients
with a Glasgow-Blatchford score of 0 should be considered for discharge and
subsequent outpatient endoscopy. Patients with a score >0 should be
considered for endoscopy. This is shown below:

This
patients scores 10 (4 for urea of 12.1, 3 for Hb 104, 0 for BP, score 1 for
malaena and 2 for hepatic disease).
From <https://mle.ncl.ac.uk/cases/page/17274/>
Summary
05 January 2021
12:46
After
blood tests
most
important next step in NAFLD is to stage the disease; this helps stratify
severity and those that should be managed in primary or secondary care. Most
commonly in primary care this is done using either: FIB 4 score NAFLD score
Tend to use FIB 4 in Newcastle; get students to calculate FIB 4 https://www.mdcalc.com/fibrosis-4-fib-4-index-liver-fibrosis
Answer =1.24 Those with a FIB 4 65) have a low risk of advanced fibrosis and
therefore can be managed in primary care. Management from the GP should concentrate
on weight loss and management of metabolic risk factors including good diabetic
control. Weight loss may include increasing exercise, decrease calories, use of
a Mediterranean diet. Patients may find groups or apps helpful in this (this is
covered in more detail in the NAFLD lecture). Also emphasis that if patient
loses >10% of body weight can have complete resolution of inflammation
Bloods should be repeated at least 3 yearly (but normally performed on an
annual basis) and a FIB 4 recalculated
NICE
guidelines suggest any patient who drinks > 50 units a week should be
screened for significant liver disease with a fibroscan or bloods such as ELF
test (estimation of liver fibrosis – blood test which looks for markers of
fibrosis in the blood and gives an estimation of overall scarring)

Cirrhosis:
All
patients with cirrhosis should be screened for osteoporosis with a DEXA scan
- Screened for varices with an OGD
- All patients (who would be fit enough to be
considered for treatment) require 6 monthly HCC surveillance with USS (and most
also measure alpha-feto protein
ascites/
peripheral oedema -
This is normally done with diuretics, usually
introduce spironolactone first and then add in furosemide if not relieved on
spironolactone alone
- This requires close monitoring of renal
function and particularly sodium between increments of diuretics
-
Some patients develop refractory ascites (persistent ascites despite maximal
doses of diuretics) or renal function/ hyponatraemia preclude increasing
diuretic dose further
-
An option in these patients is large volume paracentesis (drainage of ascites)
done as a day case procedure and can be repeated every few weeks
- If requiring regular paracentesis can
consider TIPSS (transjugular intrahepatic portosystemic shunt) as long as liver
synthetic function good and not had episodes of encephalopathy (as risk of
encephalopathy significantly increases post TIPSS). If TIPSS contraindicated
alternative would be to consider liver transplant
Liver
transplantation criteria for chronic liver disease include:
- Poor synthetic function; this is assessed by
the use of UKELD; this is a score that takes into account bilirubin, INR,
creatinine and sodium https://www.mdcalc.com/unitedkingdom-model-end-stage-liver-disease-ukeld
A UKELD of 49 or more is used as a threshold for eligibility; this confers a 9%
chance of death within a year without transplant
-
Persistent encephalopathy
-
Refractory ascites (not suitable for TIPSS)
- Hepatocellular cancer – there are size
criteria for this to be eligible must be 1 lesion < 5cm or can have up to 5
lesions with all lesions < 3cm
If considering transplant,
patients are put forward for an assessment where lots of factors are taken
into account including overall
fitness, other co-morbidities etc. If accepted for transplant they are
then placed on the transplant
waiting list.
24 December 2020
14:09
Degenerative cervical myelopathy
Degenerative cervical myelopathy
(DCM) has a number of risk factors, which include smoking due to its effects on
the intervertebral discs, genetics and occupation - those exposing patients to
high axial loading [1].
The presentation of DCM is very
variable. Early symptoms are often subtle and can vary in severity day to day,
making the disease difficult to detect initially. However as a progressive
condition, worsening, deteriorating or new symptoms should be a warning sign.
DCM symptoms can include any
combination of [1]:
·
Pain (affecting the neck, upper or lower limbs)
·
Loss of motor function (loss of digital dexterity, preventing
simple tasks such as holding a fork or doing up their shirt buttons, arm or leg
weakness/stiffness leading to impaired gait and imbalance
·
Loss of sensory function causing numbness
·
Loss of autonomic function (urinary or faecal incontinence
and/or impotence) - these can occur and do not necessarily suggest cauda equina
syndrome in the absence of other hallmarks of that condition
·
Hoffman's sign: is a reflex test to assess for cervical
myelopathy. It is performed by gently flicking one finger on a patient's hand.
A positive test results in reflex twitching of the other fingers on the same
hand in response to the flick.
The most common symptoms at
presentation of DCM are unknown, but in one series 50% of patients were initially
incorrectly diagnosed and sometimes treated for carpal tunnel syndrome [2].
An MRI of the cervical spine is the
gold standard test where cervical myelopathy is suspected. It may reveal disc
degeneration and ligament hypertrophy, with accompanying cord signal change.
All patients with degenerative
cervical myelopathy should be urgently referred for assessment by specialist
spinal services (neurosurgery or orthopaedic spinal surgery). This is due to
the importance of early treatment. The timing of surgery is important, as any
existing spinal cord damage can be permanent. Early treatment (within 6 months
of diagnosis) offers the best chance of a full recovery but at present, most
patients are presenting too late. In one study, patients averaged over 5
appointments before diagnosis, representing >2 years.
Currently, decompressive surgery is
the only effective treatment. It has been shown to prevent disease progression.
Close observation is an option for mild stable disease, but anything
progressive or more severe requires surgery to prevent further deterioration.
Physiotherapy should only be initiated by specialist services, as manipulation
can cause more spinal cord damage.
References
1. Baron EM, Young WF. Cervical
spondylotic myelopathy: a brief review of its pathophysiology, clinical course,
and diagnosis. Neurosurgery. 2007 Jan;60(1 Supp1 1):S35-41.
2. Behrbalk E, Salame K, Regev GJ,
Keynan O, Boszczyk B, Lidar Z. Delayed diagnosis of cervical spondylotic
myelopathy by primary care physicians. Neurosurg Focus. 2013 Jul;35(1):E1.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Cluster headache
Cluster headaches are known to be
one of the most painful conditions that patients can have the misfortune to
suffer. The name relates to the pattern of the headaches - they typically occur
in clusters lasting several weeks, with the clusters themselves typically once
a year.
Cluster headaches are more common
in men (3:1) and smokers. Alcohol
may trigger an attack and there also appears to be a
relation to nocturnal sleep.
Features
·
pain typical occurs once or twice a day, each
episode lasting 15 mins - 2 hours
·
clusters typically last 4-12 weeks
·
intense sharp, stabbing pain around one eye (recurrent attacks
'always' affect same side)
·
patient is restless and agitated during an attack
·
accompanied by redness, lacrimation, lid swelling
·
nasal stuffiness
·
miosis and ptosis in a minority
Management
·
acute: 100% oxygen (80% response rate within
15 minutes), subcutaneous triptan (75% response rate within 15 minutes)
·
prophylaxis: verapamil is the drug of choice. There is also some evidence to
support a tapering dose of prednisolone
·
NICE recommend seeking specialist advice from a neurologist if a
patient develops cluster headaches with respect to neuroimaging
Some neurologists use the term
trigeminal autonomic cephalgia to group a number of conditions including
cluster headache, paroxysmal hemicrania and short-lived unilateral neuralgiform
headache with conjunctival injection and tearing (SUNCT). It is recommended
such patients are referred for specialist assessment as specific treatment may be
required, for example it is known paroxysmal hemicrania responds very well to
indomethacin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Status epilepticus
This is a medical emergency. The
priority is termination of seizure activity, which if prolonged will lead to
irreversible brain damage.
Management
·
ABC
o airway adjunct
o oxygen
o check blood glucose
·
First-line drugs are benzodiazepines such as diazepam or
lorazepam
o in the prehospital setting diazepam
may be given rectally
o in hospital IV
lorazepam is generally used. This may be repeated
once after 10-20
minutes
·
If ongoing (or 'established') status it is appropriate to start
a second-line agent such as phenytoin or phenobarbital
infusion
·
If no response ('refractory status') within 45 minutes from
onset, then the best way to achieve rapid control of seizure activity is
induction of general anaesthesia.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Parkinson's disease: management
Parkinsons disease should only be
diagnosed, and management initiated, by a specialist with
expertise in movement disorders. However, it is important for all doctors to be
aware of the medications used in Parkinson's given the prevalence of this
condition. NICE published guidelines in 2017 regarding the management of
Parkinson's disease.
For first-line treatment:
·
if the motor symptoms are affecting the patient's quality of
life: levodopa
·
if the motor symptoms are not affecting the patient's quality of
life: dopamine agonist (non-ergot derived), levodopa or monoamine oxidase B
(MAO‑B) inhibitor
Whilst all drugs used to treat
Parkinson's can cause a wide variety of side-effects NICE produced tables to
help with decision making:
|
|
Levodopa |
Dopamine agonists |
MAO‑B
inhibitors |
|
Motor symptoms |
More improvement in motor symptoms |
Less improvement in motor symptoms |
Less improvement in motor symptoms |
|
Activities of daily living |
More improvement in activities of daily
living |
Less improvement in activities of daily
living |
Less improvement in activities of daily
living |
|
Motor complications |
More motor complications |
Fewer motor complications |
Fewer motor complications |
|
Adverse events |
Fewer specified adverse events* |
More specified adverse events* |
Fewer specified adverse events* |
* excessive sleepiness, hallucinations and impulse control disorders
If a patient continues to have
symptoms despite optimal levodopa treatment or has developed dyskinesia then
NICE recommend the addition of a dopamine agonist, MAO‑B inhibitor or catechol‑O‑methyl
transferase (COMT) inhibitor as an adjunct. Again, NICE summarise the main
points in terms of decision making:
|
|
Dopamine agonists |
MAO‑B
inhibitors |
COMT inhibitors |
Amantadine |
|
Motor symptoms |
Improvement in motor symptoms |
Improvement in motor symptoms |
Improvement in motor symptoms |
No evidence of improvement in motor
symptoms |
|
Activities of daily living |
Improvement in activities of daily
living |
Improvement in activities of daily
living |
Improvement in activities of daily
living |
No evidence of improvement in
activities of daily living |
|
Off time |
More off‑time reduction |
Off‑time reduction |
Off‑time reduction |
No studies reporting this outcome |
|
Adverse events |
Intermediate risk of adverse events |
Fewer adverse events |
More adverse events |
No studies reporting this outcome |
|
Hallucinations |
More risk of hallucinations |
Lower risk of hallucinations |
Lower risk of hallucinations |
No studies reporting this outcome |
Specific points regarding
Parkinson's medication
NICE reminds us of the risk of
acute akinesia or neuroleptic malignant syndrome if medication is not
taken/absorbed (for example due to gastroenteritis) and advise against giving
patients a 'drug holiday' for the same reason.
Impulse control disorders have
become a significant issue in recent years. These can occur with any
dopaminergic therapy but are more common with:
·
dopamine agonist therapy
·
a history of previous impulsive behaviours
·
a history of alcohol consumption and/or smoking
If excessive daytime sleepiness
develops then patients should not drive. Medication should be adjusted to
control symptoms. Modafinil can be considered if alternative strategies fail.
If orthostatic hypotension develops
then a medication review looking at potential causes should be done. If
symptoms persist then midodrine (acts on peripheral alpha-adrenergic receptors
to increase arterial resistance) can be considered.
Consider glycopyrronium bromide to
manage drooling of saliva in people with Parkinson's disease.
Further information regarding
specific anti-Parkinson's medication
Levodopa
·
usually combined with a decarboxylase inhibitor (e.g. carbidopa
or benserazide) to prevent peripheral metabolism of levodopa to dopamine
·
reduced effectiveness with time (usually by 2 years)
·
unwanted effects: dyskinesia (involuntary
writhing movements), 'on-off' effect, dry mouth, anorexia, palpitations, postural hypotension, psychosis, drowsiness
·
no use in neuroleptic induced parkinsonism
·
it is important not to acutely stop levodopa, for example if a patient is
admitted to hospital. If a patient with Parkinson's disease cannot take
levodopa orally, they can be given a dopamine agonist patch as rescue medication to prevent acute dystonia
Dopamine receptor agonists
·
e.g. bromocriptine, ropinirole, cabergoline, apomorphine
·
ergot-derived dopamine receptor agonists (bromocriptine, cabergoline)
have been associated with pulmonary, retroperitoneal and
cardiac fibrosis. The Committee on Safety of Medicines advice that an
echocardiogram, ESR, creatinine and chest x-ray should be obtained prior to
treatment and patients should be closely monitored
·
patients should be warned about the potential for dopamine
receptor agonists to cause impulse control disorders and excessive daytime
somnolence
·
more likely than levodopa to cause hallucinations in older
patients. Nasal congestion and postural hypotension are also seen in some
patients
MAO-B (Monoamine Oxidase-B)
inhibitors
·
e.g. selegiline
·
inhibits the breakdown of dopamine secreted by the dopaminergic
neurons
Amantadine
·
mechanism is not fully understood, probably increases dopamine
release and inhibits its uptake at dopaminergic synapses
·
side-effects include ataxia, slurred
speech, confusion, dizziness and livedo
reticularis
COMT (Catechol-O-Methyl
Transferase) inhibitors
·
e.g. entacapone, tolcapone
·
COMT is an enzyme involved in the breakdown of dopamine, and
hence may be used as an adjunct to levodopa therapy
·
used in conjunction with levodopa in patients with established
PD
Antimuscarinics
·
block cholinergic receptors
·
now used more to treat drug-induced parkinsonism rather than
idiopathic Parkinson's disease
·
help tremor and rigidity
·
e.g. procyclidine, benzotropine, trihexyphenidyl (benzhexol)
|
|
|
|
Image
sourced from Wikipedia |
|

Diagram showing the mechanism of action of Parkinson's
drugs
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Stroke: types
The Bamford/Oxford Stroke
Classification (also known as the Bamford Classification)
classifies strokes based on the initial symptoms. A summary is as follows:
The following criteria should be
assessed:
·
1. unilateral hemiparesis and/or hemisensory loss of the face,
arm & leg
·
2. homonymous hemianopia
·
3. higher cognitive dysfunction e.g. dysphasia
Total anterior circulation infarcts
(TACI, c. 15%)
·
involves middle and anterior cerebral arteries
·
all 3 of the above criteria are present
Partial anterior circulation
infarcts (PACI, c. 25%)
·
involves smaller arteries of anterior circulation e.g. upper or
lower division of middle cerebral artery
·
2 of the above criteria are present
Lacunar infarcts (LACI, c. 25%)
·
involves perforating arteries around the internal capsule,
thalamus and basal ganglia
·
presents with 1 of the following:
·
1. unilateral weakness (and/or sensory deficit) of face and arm,
arm and leg or all three.
·
2. pure sensory stroke.
·
3. ataxic hemiparesis
Posterior circulation infarcts
(POCI, c. 25%)
·
involves vertebrobasilar arteries
·
presents with 1 of the following:
·
1. cerebellar or brainstem syndromes
·
2. loss of consciousness
·
3. isolated homonymous hemianopia
Other recognised patterns of
stroke:
Lateral medullary syndrome
(posterior inferior cerebellar artery)
·
aka Wallenberg's syndrome
·
ipsilateral: ataxia, nystagmus, dysphagia, facial numbness,
cranial nerve palsy e.g. Horner's
·
contralateral: limb sensory loss
Weber's syndrome
·
ipsilateral III palsy
·
contralateral weakness
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Migraine: management
It should be noted that as a
general rule 5-HT receptor agonists are used in the acute treatment of migraine
whilst 5-HT receptor antagonists are used in prophylaxis. NICE produced
guidelines in 2012 on the management of headache, including migraines.
Acute treatment
·
first-line: offer combination therapy with an oral triptan and an
NSAID, or an oral triptan and paracetamol
·
for young people aged 12-17 years consider a nasal triptan in
preference to an oral triptan
·
if the above measures are not effective or not tolerated offer a
non-oral preparation of metoclopramide* or prochlorperazine and consider adding
a non-oral NSAID or triptan
Prophylaxis
·
prophylaxis should be given if patients are experiencing 2 or more attacks per month. Modern treatment is effective in about 60% of patients.
·
NICE advise either topiramate or propranolol 'according to the person's
preference, comorbidities and risk of adverse events'. Propranolol should be
used in preference to topiramate in women of child bearing
age as it may be
teratogenic and it can reduce the effectiveness of hormonal contraceptives
·
if these measures fail NICE recommend 'a course of
up to 10 sessions of acupuncture over 5-8 weeks'
·
NICE recommend: 'Advise people with migraine that riboflavin
(400 mg once a day) may be effective in reducing migraine frequency and
intensity for some people'
·
for women with predictable menstrual
migraine treatment NICE
recommend either frovatriptan (2.5 mg twice a day) or zolmitriptan (2.5 mg
twice or three times a day) as a type of 'mini-prophylaxis'
·
pizotifen is no longer recommend. Adverse effects such as weight
gain & drowsiness are common
*caution should be exercised with
young patients as acute dystonic reactions may develop
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Motor neuron disease: features
Motor neuron disease is a
neurological condition of unknown cause which can present with both upper and
lower motor neuron signs. It rarely presents before 40 years and various
patterns of disease are recognised including amyotrophic lateral sclerosis,
progressive muscular atrophy and bulbar palsy.
There are a number of clues which
point towards a diagnosis of motor neuron disease:
·
fasciculations
·
the absence of sensory signs/symptoms*
·
the mixture of lower motor neuron and
upper motor neuron signs
·
wasting of the small hand muscles/tibialis anterior is common
Other features
·
doesn't affect external ocular muscles
·
no cerebellar signs
·
abdominal reflexes are usually preserved and sphincter
dysfunction if present is a late feature
The diagnosis of motor neuron
disease is clinical, but nerve conduction studies will show normal motor conduction and can help exclude a neuropathy. Electromyography shows a
reduced number of action potentials with increased amplitude. MRI is usually
performed to exclude the differential diagnosis of cervical cord compression
and myelopathy
*vague sensory symptoms may occur
early in the disease (e.g. limb pain) but 'never' sensory signs
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Myasthenia gravis
Myasthenia gravis is an autoimmune
disorder resulting in insufficient functioning acetylcholine receptors. Antibodies to acetylcholine
receptors are seen in 85-90% of cases*.
Myasthenia is more common in women (2:1)
The key feature is muscle fatigability - muscles become progressively weaker during periods of activity
and slowly improve after periods of rest:
·
extraocular muscle weakness: diplopia
·
proximal muscle weakness: face, neck, limb girdle
·
ptosis
·
dysphagia
Associations
·
thymomas in 15%
·
autoimmune disorders: pernicious anaemia, autoimmune thyroid
disorders, rheumatoid, SLE
·
thymic hyperplasia in 50-70%
Investigations
·
single fibre electromyography: high sensitivity (92-100%)
·
CT thorax to exclude thymoma
·
CK normal
·
autoantibodies: around 85-90% of patients have antibodies to
acetylcholine receptors. In the remaining patients, about about 40% are
positive for anti-muscle-specific tyrosine kinase antibodies
·
Tensilon test: IV edrophonium reduces muscle weakness
temporarily - not commonly used anymore due to the risk of cardiac arrhythmia
Management
·
long-acting acetylcholinesterase inhibitors
o pyridostigmine is first-line
·
immunosuppression may be used if
o prednisolone initially
o azathioprine, cyclosporine,
mycophenolate mofetil may also be used
·
thymectomy
Management of myasthenic crisis
·
plasmapheresis
·
intravenous immunoglobulins
*antibodies are less commonly seen
in disease limited to the ocular muscles
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Neuroleptic malignant syndrome
Neuroleptic malignant syndrome is a
rare but dangerous condition seen in patients taking antipsychotic medication. It carries a mortality of up to 10% and can also occur with
atypical antipsychotics. It may also occur with dopaminergic drugs (such as levodopa)
for Parkinson's disease, usually when the drug is suddenly stopped or the dose reduced.
The pathophysiology is unknown but
one theory is that the dopamine blockade induced by antipsychotics triggers
massive glutamate release and subsequent neurotoxicity and muscle damage.
It occurs within hours to days of
starting an antipsychotic (antipsychotics are also known as neuroleptics, hence
the name) and the typical
features are:
·
pyrexia
·
muscle rigidity
·
autonomic lability: typical features include hypertension,
tachycardia and tachypnoea
·
agitated delirium with confusion
A raised creatine kinase is present
in most cases. Acute
kidney injury (secondary to rhabdomyolysis) may
develop in severe cases. A leukocytosis may also be seen
Management
·
stop antipsychotic
·
patients should be transferred to a medical ward if they are on
a psychiatric ward and often they are nursed in intensive care units
·
IV fluids to prevent renal failure
·
dantrolene may be useful in selected cases
o thought to work by decreasing
excitation-contraction coupling in skeletal muscle by binding to the ryanodine
receptor, and decreasing the release of calcium from the sarcoplasmic reticulum
·
bromocriptine, dopamine agonist, may also be used
|
|
|
|
|
|
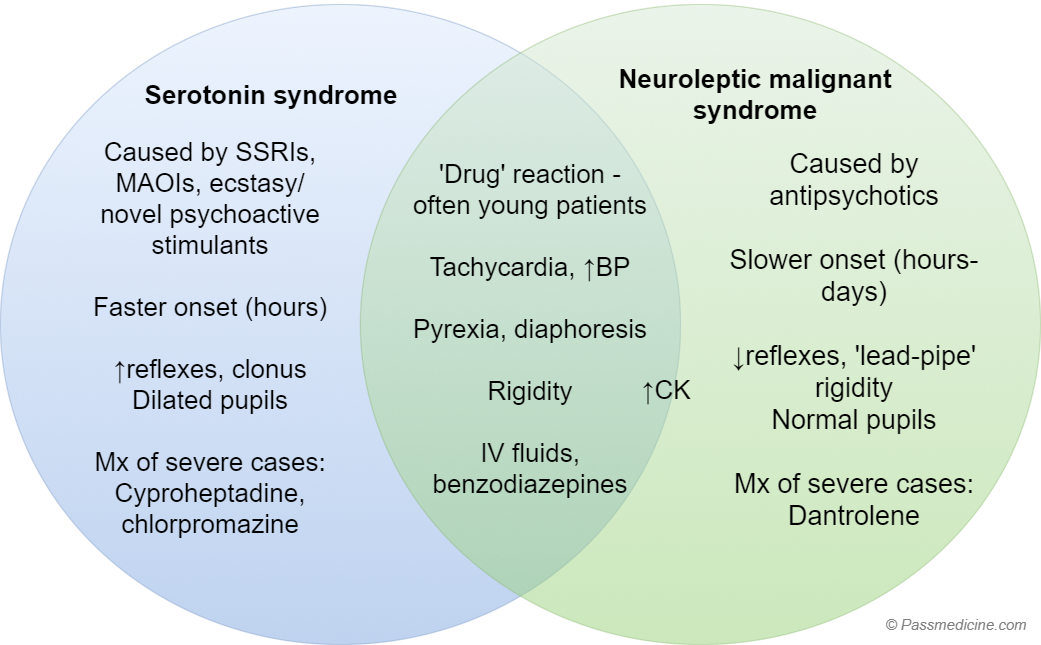
Venn diagram showing contrasting serotonin syndrome with
neuroleptic malignant syndrome. Note that both conditions can cause a raised
creatine kinase (CK) but it tends to be more associated with NMS.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Parkinson's disease: features
Parkinson's disease is a
progressive neurodegenerative condition caused by degeneration of dopaminergic
neurons in the substantia nigra. This results in a classic triad
of features: bradykinesia, tremor and rigidity. The symptoms of Parkinson's disease
are characteristically asymmetrical.
Epidemiology
·
around twice as common in men
·
mean age of diagnosis is 65 years
Bradykinesia
·
poverty of movement also seen, sometimes referred to as
hypokinesia
·
short, shuffling steps with reduced arm swinging
·
difficulty in initiating movement
Tremor
·
most marked at rest, 3-5 Hz
·
worse when stressed or tired, improves
with voluntary movement
·
typically 'pill-rolling', i.e. in the thumb and index finger
Rigidity
·
lead pipe
·
cogwheel: due to superimposed tremor
Other characteristic features
·
mask-like facies
·
flexed posture
·
micrographia
·
drooling of saliva
·
psychiatric features: depression is the most
common feature (affects about 40%); dementia, psychosis and sleep disturbances may also occur
·
impaired olfaction
·
REM sleep behaviour disorder
·
fatigue
·
autonomic dysfunction:
o postural hypotension
Drug-induced parkinsonism has slightly
different features to Parkinson's disease:
·
motor symptoms are generally rapid onset and bilateral
·
rigidity and rest tremor are uncommon
Diagnosis is usually clinical.
However, if there is difficulty differentiating between essential tremor and
Parkinson's disease NICE recommend considering 123I‑FP‑CIT single photon emission computed
tomography (SPECT).
|
|
|
|
Image
sourced from Wikipedia |
|

A Lewy body (stained brown) in a brain cell of the
substantia nigra in Parkinson's disease. The brown colour is positive
immunohistochemistry staining for alpha-synuclein.
|
|
|
|
Image
sourced from Wikipedia |
|

Discoloration of the substantia nigra due to loss of
pigmented nerve cells.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:17
Tuberous sclerosis
Tuberous sclerosis (TS) is a
genetic condition of autosomal dominant inheritance. Like neurofibromatosis,
the majority of features seen in TS are neurocutaneous.
Cutaneous features
·
depigmented 'ash-leaf' spots which fluoresce under UV light
·
roughened patches of skin over lumbar spine
(Shagreen patches)
·
adenoma sebaceum (angiofibromas): butterfly distribution over nose
·
fibromata beneath nails (subungual
fibromata)
·
café-au-lait spots* may be seen
Neurological features
·
developmental delay
·
epilepsy (infantile spasms or partial)
·
intellectual impairment
Also
·
retinal hamartomas: dense white areas on retina (phakomata)
·
rhabdomyomas of the heart
·
gliomatous changes can occur in the brain lesions
·
polycystic kidneys, renal angiomyolipomata
·
lymphangioleiomyomatosis: multiple lung cysts
|
|
|
|
|
|

Comparison of neurofibromatosis and tuberous sclerosis.
Note that whilst they are both autosomal dominant neurocutaneous disorders
there is little overlap otherwise
*these of course are more commonly
associated with neurofibromatosis. However a 1998 study of 106 children with TS
found café-au-lait spots in 28% of patients
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Brachial plexus
|
Origin |
Anterior
rami of C5 to T1 |
|
Sections
of the plexus |
·
Roots,
trunks, divisions, cords, branches ·
Mnemonic:Real
Teenagers Drink Cold Beer |
|
Roots |
·
Located in
the posterior triangle ·
Pass between
scalenus anterior and medius |
|
Trunks |
·
Located
posterior to middle third of clavicle ·
Upper and
middle trunks related superiorly to the subclavian artery ·
Lower trunk
passes over 1st rib posterior to the subclavian artery |
|
Divisions |
Apex
of axilla |
|
Cords |
Related
to axillary artery |
Diagram illustrating the branches
of the brachial plexus
|
|
|
|
Image
sourced from Wikipedia |
|

Cutaneous sensation of the upper
limb
|
|
|
|
Image
sourced from Wikipedia |
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Multiple system atrophy
There are 2 predominant types of
multiple system atrophy
·
1) MSA-P - Predominant Parkinsonian features
·
2) MSA-C - Predominant Cerebellar features
Shy-Drager syndrome is a type of
multiple system atrophy.
Features
·
parkinsonism
·
autonomic disturbance
o erectile dysfunction: often an
early feature
o postural hypotension
o atonic bladder
·
cerebellar signs
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Psychogenic non-epileptic seizures
Psychogenic nonepileptic seizures
are sometimes referred to as pseudoseizures.
Factors favouring pseudoseizures
·
pelvic thrusting
·
family member with epilepsy
·
much more common in females
·
crying after seizure
·
don't occur when alone
·
gradual onset
Factors favouring true epileptic
seizures
·
tongue biting
·
raised serum prolactin*
Video telemetry is useful for
differentiating
*why prolactin is raised following
seizures is not fully understood. It is hypothesised that there is spread of
electrical activity to the ventromedial hypothalamus, leading to release of a
specific prolactin regulator into the hypophyseal portal system
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Subdural haemorrhage
A subdural haematoma is a
collection of blood deep to the dural layer of the meninges. The blood is not
within the substance of the brain and is therefore called an ‘extra-axial’ or
‘extrinsic’ lesion. They can be unilateral or bilateral.
Subdural haematomas can be
classified in terms of their age:
·
Acute
·
Subacute
·
Chronic
Although the collection of blood is
within the same anatomical compartment, acute and chronic subdurals have
important differences in terms of their mechanisms, associated clinical
features and management:
Acute subdural haematoma
An acute subdural haematoma is a
collection of fresh blood within the subdural space and is most commonly caused
by high-impact trauma. Since it is associated with high-impact injuries, there
is often other brain underlying brain injuries.
There is a spectrum of severity of
symptoms and presentation depending on the size of the compressive acute
subdural haematoma and the associated injuries. Presentation ranges from an
incidental finding in trauma to severe coma and coning due to herniation.
CT imaging is the first-line
investigation and will show a crescentic collection, not limited by suture
lines. They will appear hyperdense (bright) in comparison to the brain. Large
acute subdural haematomas will push on the brain (‘mass effect’) and cause
midline shift or herniation.
Small or incidental acute subdurals
can be observed conservatively. Surgical options include monitoring of
intracranial pressure and decompressive craniectomy.
Chronic subdural haematoma
A chronic subdural haematoma is a
collection of blood within the subdural space that has been present for weeks
to months.
Rupture of the small bridging veins
within the subdural space rupture and cause slow bleeding. Elderly and
alcoholic patients are particularly at risk of subdural haematomas since they
have brain atrophy and therefore fragile or taut bridging veins.
Presentation is typically a several
week to month progressive history of either confusion, reduced consciousness or
neurological deficit.
Infants also have fragile bridging
veins and can rupture in shaken baby syndrome.
On CT imaging they similarly are
crescentic in shape, not restricted by suture lines and compress the brain
(‘mass effect’). In contrast to acute subdurals, chronic subdurals are hypodense (dark) compared to the substance of the brain.
If the chronic subdural is an
incidental finding or if it is small in size with no associated neurological
deficit then it can be managed conservatively with the hope that it will
dissolve with time. If the patient is confused, has an associated neurological
deficit or has severe imaging findings then surgical decompression with burr
holes is required.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Third nerve palsy
Features
·
eye is deviated 'down and out'
·
ptosis
·
pupil may be dilated (sometimes called a 'surgical' third nerve
palsy)
Causes
·
diabetes mellitus
·
vasculitis e.g. temporal arteritis, SLE
·
false localizing sign* due to uncal herniation through tentorium
if raised ICP
·
posterior communicating artery aneurysm
o pupil dilated
o often associated pain
·
cavernous sinus thrombosis
·
Weber's syndrome: ipsilateral third nerve palsy with
contralateral hemiplegia -caused by midbrain strokes
·
other possible causes: amyloid, multiple sclerosis
*this term is usually associated
with sixth nerve palsies but it may be used for a variety of neurological
presentations
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Trigeminal neuralgia
Trigeminal neuralgia is a pain
syndrome characterised by severe unilateral pain. The vast majority of cases
are idiopathic but compression of the trigeminal roots by tumours or vascular
problems may occur.
The International Headache Society
defines trigeminal neuralgia as:
·
a unilateral disorder characterised by brief electric shock-like
pains, abrupt in onset and termination, limited to one or more divisions of the
trigeminal nerve
·
the pain is commonly evoked by light touch, including washing,
shaving, smoking, talking, and brushing the teeth (trigger factors), and
frequently occurs spontaneously
·
small areas in the nasolabial fold or chin may be particularly
susceptible to the precipitation of pain (trigger areas)
·
the pains usually remit for variable periods
NICE Clinical Knowledge Summaries
list the following as red flag symptoms and signs suggesting a serious
underlying cause:
·
Sensory changes
·
Deafness or other ear problems
·
History of skin or oral lesions that could spread perineurally
·
Pain only in the ophthalmic division of the trigeminal nerve
(eye socket, forehead, and nose), or bilaterally
·
Optic neuritis
·
A family history of multiple sclerosis
·
Age of onset before 40 years
Management
·
carbamazepine is first-line
·
failure to respond to treatment or atypical features (e.g. <
50 years old) should prompt referral to neurology
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Epilepsy: localising features of focal seizures
|
Location |
Typical seizure type |
|
Temporal lobe (HEAD) |
Hallucinations (auditory/gustatory/olfactory),
Epigastric rising/Emotional, Automatisms (lip
smacking/grabbing/plucking), Deja vu/Dysphasia post-ictal) |
|
Frontal lobe (motor) |
Head/leg movements, posturing, post-ictal weakness, Jacksonian march |
|
Parietal lobe (sensory) |
Paraesthesia |
|
Occipital lobe (visual) |
Floaters/flashes |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Facial nerve palsy
The facial nerve is the main nerve
supplying the structures of the second embryonic branchial arch. It is
predominantly an efferent nerve to the muscles of facial expression, digastric
muscle and also to many glandular structures. It contains a few afferent fibres
which originate in the cells of its genicular ganglion and are concerned with
taste.
Supply - 'face, ear, taste, tear'
·
face: muscles of facial expression
·
ear: nerve to stapedius
·
taste: supplies anterior two-thirds of tongue
·
tear: parasympathetic fibres to lacrimal glands, also salivary
glands
Causes of bilateral facial nerve
palsy
·
sarcoidosis
·
Guillain-Barre syndrome
·
Lyme disease
·
bilateral acoustic neuromas (as in neurofibromatosis type 2)
·
as Bell's palsy is relatively common it accounts for up to 25%
of cases f bilateral palsy, but this represents only 1% of total Bell's palsy
cases
Causes of unilateral facial nerve
palsy - as above plus
|
Lower
motor neuron ·
Bell's palsy ·
Ramsay-Hunt syndrome (due to herpes zoster) ·
acoustic neuroma ·
parotid tumours ·
HIV ·
multiple sclerosis* ·
diabetes mellitus |
Upper motor neuron ·
stroke |
LMN vs. UMN
·
upper motor neuron lesion 'spares' upper face i.e. forehead
·
lower motor neuron lesion affects all facial muscles
*may also cause an UMN palsy
Path
Subarachnoid path
·
Origin: motor- pons, sensory- nervus intermedius
·
Pass through the petrous temporal bone into the internal
auditory meatus with the vestibulocochlear nerve. Here they combine to become
the facial nerve.
Facial canal path
·
The canal passes superior to the vestibule of the inner ear
·
At the medial aspect of the middle ear, it becomes wider and
contains the geniculate ganglion.
- 3 branches:
·
1. greater petrosal nerve
·
2. nerve to stapedius
·
3. chorda tympani
Stylomastoid foramen
·
Passes through the stylomastoid foramen (tympanic cavity
anterior and mastoid antrum posteriorly)
·
Posterior auricular nerve and branch to posterior belly of
digastric and stylohyoid muscle
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Neuropathic pain
Neuropathic pain may be defined as
pain which arises following damage or disruption of the nervous system. It is
often difficult to treat and responds poorly to standard analgesia.
Examples include:
·
diabetic neuropathy
·
post-herpetic neuralgia
·
trigeminal neuralgia
·
prolapsed intervertebral disc
NICE updated their guidance on the
management of neuropathic pain in 2013:
·
first-line treatment*: amitriptyline, duloxetine, gabapentin or
pregabalin
o if the first-line drug treatment
does not work try one of the other 3 drugs
o in contrast to standard analgesics,
drugs for neuropathic pain are typically used as monotherapy, i.e. if not working then drugs should be switched, not added
·
tramadol may be used as 'rescue therapy' for exacerbations of
neuropathic pain
·
topical capsaicin may be used for localised neuropathic pain
(e.g. post-herpetic neuralgia)
·
pain management clinics may be useful in patients with resistant
problems
*please note that for some specific
conditions the guidance may vary. For example carbamazepine is used first-line
for trigeminal neuralgia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Peripheral neuropathy
Peripheral neuropathy may be
divided into conditions which predominately cause a motor or sensory loss
Predominately motor loss
·
Guillain-Barre syndrome
·
porphyria
·
lead poisoning
·
hereditary sensorimotor neuropathies (HSMN) -
Charcot-Marie-Tooth
·
chronic inflammatory demyelinating polyneuropathy (CIDP)
·
diphtheria
Predominately sensory loss
·
diabetes
·
uraemia
·
leprosy
·
alcoholism
·
vitamin B12 deficiency
·
amyloidosis
Alcoholic neuropathy
·
secondary to both direct toxic effects and reduced absorption of
B vitamins
·
sensory symptoms typically present prior to motor symptoms
Vitamin B12 deficiency
·
subacute combined degeneration of spinal cord
·
dorsal column usually affected first (joint position, vibration)
prior to distal paraesthesia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Phenytoin
Phenytoin is used in the management
of seizures.
Mechanism of action
·
binds to sodium channels increasing their refractory period
Adverse effects
Phenytoin is associated with a
large number of adverse effects. These may be divided into acute, chronic,
idiosyncratic and teratogenic. Phenytoin
is also an inducer of the P450 system.
Acute
·
initially: dizziness, diplopia, nystagmus, slurred
speech, ataxia
·
later: confusion, seizures
Chronic
·
common: gingival hyperplasia (secondary to increased expression
of platelet derived growth factor, PDGF), hirsutism, coarsening
of facial features, drowsiness
·
megaloblastic anaemia (secondary to altered folate
metabolism)
·
peripheral neuropathy
·
enhanced vitamin D metabolism causing osteomalacia
·
lymphadenopathy
·
dyskinesia
Idiosyncratic
·
fever
·
rashes, including severe reactions such as toxic epidermal necrolysis
·
hepatitis
·
Dupuytren's contracture*
·
aplastic anaemia
·
drug-induced lupus
Teratogenic
·
associated with cleft palate and congenital heart
disease
Monitoring
Phenytoin levels do not need to be
monitored routinely but trough
levels, immediately before dose should be checked if:
·
adjustment of phenytoin dose
·
suspected toxicity
·
detection of non-adherence to the prescribed medication
*although not listed in the BNF
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Stroke by anatomy
|
Site
of the lesion |
Associated effects |
|
Anterior cerebral artery |
Contralateral hemiparesis and sensory
loss, lower extremity > upper |
|
Middle cerebral artery |
Contralateral hemiparesis and sensory
loss, upper extremity > lower Contralateral homonymous hemianopia Aphasia |
|
Posterior cerebral artery |
Contralateral homonymous hemianopia
with macular sparing Visual agnosia |
|
Weber's syndrome
(branches of the posterior cerebral artery that supply the midbrain) |
Ipsilateral CN III palsy Contralateral weakness of upper and
lower extremity |
|
Posterior inferior cerebellar artery (lateral medullary syndrome, Wallenberg syndrome) |
Ipsilateral: facial pain and
temperature loss Contralateral: limb/torso pain and
temperature loss Ataxia, nystagmus |
|
Anterior inferior cerebellar artery (lateral pontine syndrome) |
Symptoms are similar to Wallenberg's
(see above), but: Ipsilateral: facial paralysis and
deafness |
|
Retinal/ophthalmic artery |
Amaurosis fugax |
|
Basilar artery |
'Locked-in' syndrome |
Lacunar strokes
·
present with either isolated hemiparesis, hemisensory loss or
hemiparesis with limb ataxia
·
strong association with hypertension
·
common sites include the basal ganglia, thalamus and internal
capsule
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Syringomyelia
Syringomyelia (‘syrinx’ for short)
describes a collection of cerebrospinal fluid within the spinal cord.
Syringobulbia is a similar
phenomenon in which there is a fluid-filled cavity within the medulla of the
brainstem. This is often an extension of the syringomyelia but in rare cases
can be an isolated finding.
Causes include:
·
a Chiari malformation: strong association
·
trauma
·
tumours
·
idiopathic
The classical presentation of a
syrinx is a patient who has a ‘cape-like’ (neck and arms) loss of sensation to
temperature but preservation of light touch, proprioception and vibration.
Classic examples are of patients who accidentally burn their hands without
realising. This is due to the crossing spinothalamic tracts in the anterior
commissure of the spinal cord being the first tracts to be affected. Other
symptoms and signs include spastic weakness (predominantly of the upper limbs),
paraesthesia, neuropathic pain, upgoing plantars and bowel and bladder
dysfunction. Scoliosis will occur over a matter of years if the syrinx is not
treated. It may cause a Horner’s syndrome due to compression of the sympathetic
chain, but this is rare.
Investigation requires a full spine
MRI with contrast to exclude a tumour or tethered cord. A brain MRI is also
needed to exclude a Chiari malformation.
Treatment will be directed at
treating the cause of the syrinx. In patients with a persistent or symptomatic
syrinx, a shunt into the syrinx can be placed.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Wernicke's encephalopathy
Wernicke's encephalopathy is a
neuropsychiatric disorder caused by thiamine deficiency which is most commonly
seen in alcoholics. Rarer causes include: persistent vomiting, stomach cancer,
dietary deficiency. A classic triad of ophthalmoplegia/nystagmus, ataxia and
confusion may occur. In Wernicke's encephalopathy petechial haemorrhages occur
in a variety of structures in the brain including the mamillary bodies and ventricle
walls.
Features
·
nystagmus (the most common ocular sign)
·
ophthalmoplegia
·
ataxia
·
confusion, altered GCS
·
peripheral sensory neuropathy
Investigations
·
decreased red cell transketolase
·
MRI
Treatment is with urgent
replacement of thiamine
Relationship with Korsakoff
syndrome
If not treated Korsakoff's syndrome
may develop as well. This is termed Wernicke-Korsakoff syndrome and is
characterised by the addition of antero- and retrograde amnesia and
confabulation in addition to the above symptoms.
|
|
|
|
|
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
5-HT3 antagonists
5-HT3 antagonists are antiemetics
used mainly in the management of chemotherapy-related nausea. They mainly act in the chemoreceptor trigger zone area
of the medulla oblongata.
Examples
·
ondansetron
·
granisetron
Adverse effects
·
constipation is common
·
prolonged QT interval
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Brain tumours
The majority of adult tumours are
supratentorial, where as the majority of childhood tumours are infratentorial.
|
Type
of tumour |
Features |
|
Metastases |
Metastatic brain cancer is the most
common form of brain tumours. They are often multiple and not treatable with
surgical intervention. Tumours that most commonly spread
to the brain include: ·
lung (most common) ·
breast ·
bowel ·
skin (namely melanoma) ·
kidney |
|
Gliolastoma multiforme |
• Glioblastoma is the most
common primary tumour in adults and is
associated with a poor prognosis (~ 1yr). • On imaging they are solid tumours
with central necrosis and a rim that enhances with contrast. Disruption of
the blood-brain barrier and therefore are associated with vasogenic oedema. • Histology: Pleomorphic tumour
cells border necrotic areas • Treatment is surgical with
postoperative chemotherapy and/or radiotherapy. Dexamethasone is used to
treat the oedema. |
|
Meningioma |
• The second most common primary brain
tumour in adults • Meningiomas are typically benign,
extrinsic tumours of the central nervous system. They arise from the dura
mater of the meninges and cause symptoms
by compression rather than invasion. • They typically are located at the
falx cerebri, superior sagittal sinus, convexity or skull base. • Histology: Spindle cells in
concentric whorls and calcified psammoma bodies • Investigation is with CT (will show contrast
enhancement) and MRI, and treatment will involve
either observation, radiotherapy or surgical resection. |
|
Vestibular schwannoma |
• A vestibular schwannoma (previously
termed acoustic neuroma) is a benign tumour arising from the eighth cranial
nerve (vestibulocochlear nerve). Often seen in the cerebellopontine
angle. It presents with hearing loss, facial
nerve palsy (due to compression of the nearby facial nerve) and tinnitus. • Neurofibromatosis
type 2 is associated with bilateral vestibular schwannomas. • Histology: Antoni A or B
patterns are seen. Verocay bodies (acellular areas surrounded by nuclear palisades) • Treatment may involve observation,
radiotherapy or surgery. |
|
Pilocytic astrocytoma |
• The most common
primary brain tumour in children • Histology: Rosenthal
fibres (corkscrew eosinophilic bundle) |
|
Medulloblastoma |
• A medulloblastoma is an aggressive
paediatric brain tumour that arises within the infratentorial compartment. It
spreads through the CSF system. Treatment is surgical resection and
chemotherapy. • Histology: Small, blue cells.
Rosette pattern of cells with many mitotic figures |
|
Ependymoma |
• Commonly seen in the 4th
ventricle • May cause hydrocephalus • Histology: perivascular
pseudorosettes |
|
Oligodendroma |
• Benign, slow-growing tumour
common in the frontal lobes • Histology: Calcifications with
'fried-egg' appearance |
|
Haemangioblastoma |
• Vascular tumour of
the cerebellum • Associated with von
Hippel-Lindau syndrome • Histology: foam cells and high
vascularity |
|
Pituitary adenoma |
• Pituitary adenomas are benign tumours
of the pituitary gland. They are either secretory (producing a hormone in
excess) or non-secretory. They may be divided into microadenomas (smaller
than 1cm) or macroadenoma (larger than 1cm). • Patients will present with the
consequences of hormone excess (e.g. Cushing’s due to ACTH, or acromegaly due
to GH) or depletion. Compression of the optic chiasm will cause a bitemporal
hemianopia due to the crossing nasal fibers. • Investigation requires a pituitary
blood profile and MRI. Treatment can either be hormonal or surgical (e.g.
transphenoidal resection). |
|
Craniopharyngioma |
• Most common paediatric supratentorial
tumour • A craniopharyngioma is a solid/cystic
tumour of the sellar region that is derived from the remnants of Rathke’s
pouch. It is common in children, but can present in adults also. It may
present with hormonal disturbance, symptoms of hydrocephalus or bitemporal
hemianopia. • Histology: Derived from remnants
of Rathke pouch • Investigation requires pituitary
blood profile and MRI. Treatment is typically surgical with or without
postoperative radiotherapy. |
|
|
|
|
©
Image used on license from Radiopaedia |
|

Meningioma - MRI showing the typical well-circumscribed appearance. A dural
tail can be where the tumour 'connects' to the dura. It is seen in around 65%
of meningiomas.
|
|
|
|
©
Image used on license from Radiopaedia |
|

Glioblastoma multiforme - CT showing a peripherally enhancing lesion within the
left frontal lobe. Note the contrast to the more homogenous meningioma above.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Carbamazepine
Carbamazepine is chemically similar
to the tricyclic antidepressant drugs. It is most commonly used in the
treatment of epilepsy, particularly partial seizures, where carbamazepine
remains a first-line medication. Other uses include
·
trigeminal neuralgia
·
bipolar disorder
Mechanism of action
·
binds to sodium channels increases their refractory period
Adverse effects
·
P450 enzyme inducer
·
dizziness and ataxia
·
drowsiness
·
headache
·
visual disturbances (especially diplopia)
·
Steven-Johnson syndrome
·
leucopenia and agranulocytosis
·
hyponatraemia secondary to syndrome of inappropriate ADH secretion
Carbamazepine is known to exhibit autoinduction, hence when patients start carbamazepine they may see a return
of seizures after 3-4 weeks of treatment.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Common peroneal nerve lesion
The sciatic nerve divides into the
tibial and common peroneal nerves. Injury often occurs at the neck of the
fibula
The most characteristic feature of
a common peroneal nerve lesion is foot drop.
Other features include:
·
weakness of foot dorsiflexion
·
weakness of foot eversion
·
weakness of extensor hallucis longus
·
sensory loss over the dorsum of the foot and the lower lateral
part of the leg
·
wasting of the anterior tibial and peroneal muscles
From <https://www.passmedicine.com/review/textbook.php?s=#>
Meningitis
Most common adult cause (mortality)
·
meningococcus (10%)
·
pneumococcus (25%)
Diagnosis
·
if partially treated with antibiotics, negative CSF culture, but
glucose, protein and white cells unchanged
Neurological sequalae
·
sensorineural hearing loss (most common)
·
other neurological: epilepsy, paralysis
·
infective: sepsis, intracerebral abscess
·
pressure: brain herniation, hydrocephalus
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:18
Meningitis
Most common adult cause (mortality)
·
meningococcus (10%)
·
pneumococcus (25%)
Diagnosis
·
if partially treated with antibiotics, negative CSF culture, but
glucose, protein and white cells unchanged
Neurological sequalae
·
sensorineural hearing loss (most common)
·
other neurological: epilepsy, paralysis
·
infective: sepsis, intracerebral abscess
·
pressure: brain herniation, hydrocephalus
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Migraine: diagnostic criteria
The International Headache Society
has produced the following diagnostic criteria for migraine without aura:
|
Point |
Criteria |
|
A |
At least 5 attacks fulfilling criteria
B-D |
|
B |
Headache attacks lasting 4-72 hours*
(untreated or unsuccessfully treated) |
|
C |
Headache has at least two of the
following characteristics: ·
1. unilateral location* ·
2. pulsating quality (i.e., varying with the
heartbeat) ·
3. moderate or severe pain intensity ·
4. aggravation by or causing avoidance of routine
physical activity (e.g., walking or climbing stairs) |
|
D |
During headache at least one of the
following: ·
1. nausea and/or vomiting* ·
2. photophobia and phonophobia |
|
E |
Not attributed to another disorder
(history and examination do not suggest a secondary headache disorder or, if
they do, it is ruled out by appropriate investigations or headache attacks do
not occur for the first time in close temporal relation to the other
disorder) |
*In children, attacks may be
shorter-lasting, headache is more commonly bilateral, and gastrointestinal
disturbance is more prominent.
Migraine with aura (seen in around
25% of migraine patients) tends to be easier to diagnose with a typical aura
being progressive in nature and may occur hours prior to the headache. Typical
aura include a transient hemianopic disturbance or a spreading scintillating
scotoma ('jagged crescent'). Sensory symptoms may also occur
If we compare these guidelines to
the NICE criteria the following points are noted:
·
NICE suggests migraines may be unilateral or bilateral
·
NICE also give more detail about typical auras:
Auras may occur with or without
headache and:
·
are fully reversible
·
develop over at least 5 minutes
·
last 5-60 minutes
The following aura symptoms are
atypical and may prompt further investigation/referral;
·
motor weakness
·
double vision
·
visual symptoms affecting only one eye
·
poor balance
·
decreased level of consciousness.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Multiple sclerosis
Multiple sclerosis is chronic
cell-mediated autoimmune disorder characterised by demyelination in the central
nervous system.
Epidemiology
·
3 times more common in women
·
most commonly diagnosed in people aged 20-40 years
·
much more common at higher latitudes (5 times more common than
in tropics)
Genetics
·
monozygotic twin concordance = 30%
·
dizygotic twin concordance = 2%
A variety of subtypes have been
identified:
Relapsing-remitting disease
·
most common form, accounts for around 85% of patients
·
acute attacks (e.g. last 1-2 months) followed by periods of
remission
Secondary progressive disease
·
describes relapsing-remitting patients who have deteriorated and
have developed neurological signs and symptoms between relapses
·
around 65% of patients with relapsing-remitting disease go on to
develop secondary progressive disease within 15 years of diagnosis
·
gait and bladder disorders are generally seen
Primary progressive disease
·
accounts for 10% of patients
·
progressive deterioration from onset
·
more common in older people
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Neurofibromatosis
There are two types of
neurofibromatosis, NF1 and NF2. Both are inherited in an autosomal dominant fashion
NF1 is also known as von
Recklinghausen's syndrome. It is caused by a gene mutation on chromosome 17 which encodes neurofibromin and affects around 1 in 4,000
NF2 is caused by gene mutation on chromosome 22 and affects around 1 in 100,000
Features
|
NF1 |
NF2 |
|
Café-au-lait spots (>= 6, 15 mm in diameter) Axillary/groin freckles Peripheral neurofibromas Iris hamatomas (Lisch nodules) in > 90% Scoliosis Pheochromocytomas |
Bilateral vestibular schwannomas Multiple intracranial schwannomas,
mengiomas and ependymomas |
|
|
|
|
|
|
Comparison of neurofibromatosis and tuberous sclerosis.
Note that whilst they are both autosomal dominant neurocutaneous disorders
there is little overlap otherwise
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Normal pressure hydrocephalus
Normal pressure hydrocephalus is a
reversible cause of dementia seen in elderly patients. It is thought to be
secondary to reduced CSF absorption at the arachnoid villi. These changes may
be secondary to head injury, subarachnoid haemorrhage or meningitis.
A classical triad of features is
seen
·
urinary incontinence
·
dementia and bradyphrenia
·
gait abnormality (may be similar to Parkinson's disease)
It is thought around 60% of
patients will have all 3 features at the time of diagnosis. Symptoms typically
develop over a few months.
Imaging
·
hydrocephalus with an enlarged fourth ventricle
·
in addition to the ventriculomegaly there is typically an
absence of substantial sulcal atrophy
Management
·
ventriculoperitoneal shunting
·
around 10% of patients who have shunts experience significant
complications such as seizures, infection and intracerebral haemorrhages
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Radial nerve
Continuation of posterior cord of
the brachial plexus (root values C5 to T1)
Path
·
In the axilla: lies posterior to the axillary artery on
subscapularis, latissimus dorsi and teres major.
·
Enters the arm between the brachial artery and the long head of
triceps (medial to humerus).
·
Spirals around the posterior surface of the humerus in the
groove for the radial nerve.
·
At the distal third of the lateral border of the humerus it then
pierces the intermuscular septum and descends in front of the lateral
epicondyle.
·
At the lateral epicondyle it lies deeply between brachialis and
brachioradialis where it then divides into a superficial and deep terminal
branch.
·
Deep branch crosses the supinator to become the posterior
interosseous nerve.
|
|
|
|
Image
sourced from Wikipedia |
|

In the image above the relationships of the radial nerve
can be appreciated
Regions innervated
|
Motor
(main nerve) |
·
Triceps ·
Anconeus ·
Brachioradialis ·
Extensor
carpi radialis |
|
Motor
(posterior interosseous branch) |
·
Supinator ·
Extensor
carpi ulnaris ·
Extensor
digitorum ·
Extensor
indicis ·
Extensor
digiti minimi ·
Extensor
pollicis longus and brevis ·
Abductor
pollicis longus |
|
Sensory |
The
area of skin supplying the proximal phalanges on the dorsal aspect of the
hand is supplied by the radial nerve (this does not apply to the little
finger and part of the ring finger) |
Muscular innervation and effect of
denervation
|
Anatomical
location |
Muscle affected |
Effect of paralysis |
|
Shoulder |
Long head of triceps |
Minor effects on shoulder stability in
abduction |
|
Arm |
Triceps |
Loss of elbow extension |
|
Forearm |
Supinator Brachioradialis Extensor carpi radialis longus and
brevis |
Weakening of supination of prone hand
and elbow flexion in mid prone position |
Patterns of damage
·
wrist drop
·
sensory loss to small area between the dorsal aspect of the 1st
and 2nd metacarpals
Axillary damage
·
as above
·
paralysis of triceps
|
|
|
|
Image
sourced from Wikipedia |
|

The cutaneous sensation of the upper limb- illustrating
the contribution of the radial nerve
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Thoracic outlet syndrome
Thoracic outlet syndrome (TOS) is a
disorder involving compression of brachial plexus, subclavian artery or vein at
the site of the thoracic outlet. TOS can be neurogenic or vascular; the former
accounts for 90% of the cases.
Epidemiology
·
given the lack of widely agreed diagnostic criteria, the
epidemiology of TOS is not well documented
·
patients are typically young thin women possessing long neck and
drooping shoulders
·
peak onset occurs in the 4th decade
Aetiology
·
TOS develops when neck trauma occurs to individuals with
anatomical predispositions
·
neck trauma can either be a single acute incident or repeated
stresses
·
anatomical anomalies can either be in the form of soft tissue
(70%) or osseous structures (30%)
·
a well-known osseous anomaly is the presence
of cervical rib
·
examples of soft tissue causes are scalene muscle hypertrophy
and anomalous bands
·
there is usually a history of neck trauma preceding TOS
Clinical presentation of neurogenic
TOS
·
painless muscle wasting of hand muscles, with patients
complaining of hand weakness e.g. grasping
·
sensory symptoms such as numbness and tingling may be present
·
if autonomic nerves are involved, the patient may experience
cold hands, blanching or swelling
Clinical presentation of vascular
TOS:
·
subclavian vein compression leads to painful diffuse arm
swelling with distended veins
·
subclavian artery compression leads to painful arm claudication
and in severe cases, ulceration and gangrene
Examinations:
·
neurological examination and musculoskeletal examination are
necessary
·
stress manoeuvres such as Adson's manoeuvres may be attempted
although they have limited utility
·
careful examinations should aim to rule out other pathologies of
the cervical spine, the shoulder or peripheral nerves. For instance, cervical
radiculopathy, shoulder injuries and carpal tunnel syndrome
Investigations:
·
chest and cervical spine plain radiographs to check for any
obvious osseous abnormalities e.g. cervical ribs, exclude malignant tumours or
other differentials e.g. cervical spine degenerative changes
·
other imaging modalities may be helpful e.g. CT or MRI to rule
out cervical root lesions
·
venography or angiography may be helpful in vascular TOS
·
an anterior scalene block may be used to confirm neurogenic TOS
and check the likelihood of successful surgical treatment
Treatment:
·
there is a limited evidence base
·
conservative management with education, rehabilitation,
physiotherapy, or taping is typically the first-line management for neurogenic
TOS
·
surgical decompression is warranted where conservative
management has failed especially if there is a physical anomaly. Early
intervention may prevent brachial plexus degeneration
·
in vascular TOS, surgical treatment may be preferred
·
other therapies being investigated include botox injection
Further reading
1. Huang JH, Zager EL; Thoracic
outlet syndrome. Neurosurgery. 2004 Oct55(4):897-902
2. Al-Hashel JY, El Shorbgy AA,
Ahmed SF, et al; Early versus Late Surgical Treatment for Neurogenic Thoracic
Outlet Syndrome. ISRN Neurol. 2013 Sep 102013:673020. doi: 10.1155/2013/673020.
3. Kuhn, J. E., Lebus V, G. F.,
& Bible, J. (2015). Thoracic outlet syndrome. Journal of the American
Academy of Orthopaedic Surgeons, 23(4), 222-232. https://doi.org/10.5435/JAAOS-D-13-00215
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Aphasia
The table below lists the major
types of aphasia. Remember that dysarthria is different and refers to a motor
speech disorder.
|
Type
of aphasia |
Notes |
|
Wernicke's (receptive) aphasia |
Due to a lesion of the superior temporal gyrus. It is typically supplied by the inferior division
of the left MCA This area 'forms' the speech before
'sending it' to Broca's area. Lesions result in sentences that make no sense,
word substitution and neologisms but speech remains fluent Comprehension is impaired |
|
Broca's (expressive)
aphasia |
Due to a lesion of the
inferior frontal gyrus. It is typically supplied by the
superior division of the left MCA Speech is non-fluent, laboured, and
halting Comprehension is normal |
|
Conduction aphasia |
Classically due to a stroke affecting
the arcuate fasiculus - the connection between Wernicke's and Broca's area Speech is fluent but repetition is
poor. Aware of the errors they are making Comprehension is normal |
|
Global aphasia |
Large lesion affecting all 3 of the
above areas resulting in severe expressive and receptive aphasia May still be able to communicate using
gestures |
|
|
|
|
|
|

Diagram showing the main types of aphasia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Arnold-Chiari malformation
Arnold-Chiari malformation
describes the downward displacement, or herniation, of the cerebellar
tonsils through the foramen magnum. Malformations may be
congenital or acquired through trauma.
Features
·
non-communicating hydrocephalus may develop as a result of
obstruction of cerebrospinal fluid (CSF) outflow
·
headache
·
syringomyelia
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Autonomic dysreflexia
This clinical syndrome occurs in
patients who have had a spinal cord injury at, or above T6 spinal level. Briefly, afferent signals, most commonly triggered
by faecal impaction or
urinary retention (but many other triggers have been
reported) cause a sympathetic spinal reflex via thoracolumbar outflow. The
usual, centrally mediated, parasympathetic response however is prevented by the
cord lesion. The result is an unbalanced physiological response, characterised
by extreme hypertension,
flushing and sweating above the level of the cord lesion, agitation, and in untreated cases severe consequences of
extreme hypertension have been reported, e.g. haemorrhagic stroke.
Management of autonomic dysreflexia
involves removal/control
of the stimulus and treatment of any life-threatening hypertension and/or
bradycardia.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Dermatomes
The table below lists the major
dermatome landmarks:
|
Nerve
root |
Landmark |
Mnemonics |
|
C2 |
Posterior half of the skull (cap) |
|
|
C3 |
High turtleneck shirt |
|
|
C4 |
Low-collar shirt |
|
|
C5 |
Ventral axial line of upper limb |
|
|
C6 |
Thumb + index finger |
Make a 6 with your left hand by touching the tip of the thumb
& index finger together - C6 |
|
C7 |
Middle finger + palm of hand |
|
|
C8 |
Ring + little finger |
|
|
T4 |
Nipples |
T4 at the Teat Pore |
|
T5 |
Inframammary fold |
|
|
T6 |
Xiphoid process |
|
|
T10 |
Umbilicus |
BellybuT-TEN |
|
L1 |
Inguinal ligament |
L for ligament, 1 for 1nguinal |
|
L4 |
Knee caps |
Down on aLL fours - L4 |
|
L5 |
Big toe, dorsum of foot (except lateral
aspect) |
L5 = Largest of the 5 toes |
|
S1 |
Lateral foot, small toe |
S1 = the smallest one |
|
S2, S3 |
Genitalia |
|
|
|
|
|
|
|

|
|
|
|
|
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Epilepsy: a very basic introduction
Epilepsy is a common neurological
condition characterised by recurrent seizures. There are around 500,000 people
in the UK with epilepsy, of whom around two-thirds achieve satisfactory seizure
control with antiepileptic medication.
Epilepsy most commonly occurs in
isolation although certain conditions have an association with epilepsy:
·
cerebral palsy: around 30% have epilepsy
·
tuberous sclerosis
·
mitochondrial diseases
It should be remembered that
epilepsy is not the only reason people have seizures. The table below shows
some of the more common causes of recurrent seizures seen in clinical practice.
Patients may of course develop one-off seizures following any insult to the
brain, for example infection, trauma or metabolic disturbance.
|
Disorder |
Notes |
|
Febrile convulsions |
·
typically occur in children between the ages of 6
months and 5 years ·
around 3% of children will have at least one
febrile convulsion ·
usually occur early in a viral infection as the
temperature rises rapidly ·
seizures are typically brief and generalised
tonic/tonic-clonic in nature |
|
Alcohol withdrawal seizures |
·
occur in patients with a history of alcohol excess
who suddenly stop drinking, for example following admission to hospital ·
chronic alcohol consumption enhances GABA mediated
inhibition in the CNS (similar to benzodiazepines) and inhibits NMDA-type
glutamate receptors.Alcohol withdrawal is thought to be lead to the opposite
(decreased inhibitory GABA and increased NMDA glutamate transmission) ·
the peak incidence of seizures is at around 36
hours following cessation of drinking ·
patients are often given benzodiazepines following
cessation of drinking to reduce the risk |
|
Psychogenic non-epileptic seizures |
·
previously termed pseudoseizures, this term
describes patients who present with epileptic-like seizures but do not have
characteristic electrical discharges ·
patients may have a history of mental health
problems or a personality disorder |
Classification of seizures
The basic classification of
epilepsy has changed in recent years. The new basic seizure classification is
based on 3 key features:
·
1. Where seizures begin in the brain
·
2. Level of awareness during a seizure (important as can affect
safety during seizure)
·
3. Other features of seizures
Focal seizures
·
previously termed partial seizures
·
these start in a specific area, on one side of the brain
·
the level of awareness can vary in focal seizures. The terms focal aware (previously termed 'simple partial'), focal
impaired awareness (previously termed 'complex partial') and awareness unknown are used to
further describe focal seizures
·
further to this, focal seizures can be classified as being motor
(e.g. Jacksonian march), non-motor (e.g. déjà vu, jamais vu; ) or having other
features such as aura
Generalised
·
these engage or involve networks on both sides of the brain at
the onset
·
consciousness lost immediately. The level of awareness in the
above classification is therefore not needed, as all patients lose
consciousness
·
generalised seizures can be further subdivided into motor (e.g.
tonic-clonic) and non-motor (e.g. absence)
·
specific types include:
·
→ tonic-clonic (grand mal)
·
→ tonic
·
→ clonic
·
→ typical absence (petit mal)
·
→ myoclonic: brief, rapid muscle jerks
·
→ atonic
Unknown onset
·
this termed is reserved for when the origin of the seizure is
unknown
Focal to bilateral seizure
·
starts on one side of the brain in a specific area before
spreading to both lobes
·
previously termed secondary generalized seizures
In addition a number of special
forms of epilepsy are recognised in children:
|
Syndrome |
Notes |
|
Infantile spasms (West's
syndrome) |
Brief spasms beginning in first few
months of life ·
1. Flexion of head, trunk, limbs → extension of
arms (Salaam attack); last 1-2 secs, repeat up to 50 times ·
2. Progressive mental handicap ·
3. EEG: hypsarrhythmia ·
usually 2nd to serious neurological abnormality
(e.g. TS, encephalitis, birth asphyxia) or may be cryptogenic ·
poor prognosis |
|
Lennox-Gastaut syndrome |
May be extension of infantile spasms
(50% have hx) ·
onset 1-5 yrs ·
atypical absences, falls, jerks ·
90% moderate-severe mental handicap ·
EEG: slow spike ·
ketogenic diet may help |
|
Benign rolandic epilepsy |
·
paraesthesia (e.g. unilateral face), usually on
waking up |
|
Juvenile myoclonic epilepsy (Janz
syndrome) |
Typical onset in the teens, more common
in girls ·
1. Infrequent generalized seizures, often in
morning ·
2. Daytime absences ·
3. Sudden, shock like myoclonic seizure ·
usually good response to sodium valproate |
Symptoms and signs
As well as the seizure activity
described above patients who have had generalised seizures may
·
bite their tongue
·
experience incontinence of urine
Asking about such features can be
useful way of detecting epileptic seizures when taking a history from a patient
who presents with a 'blackout' or 'collapse'.
Following a seizure patients
typically have a postictal phase where they feel drowsy and tired for around 15 minutes.
Investigations
Following their first seizure
patients generally have both an electroencephalogram (EEG) and neuroimaging
(usually a MRI).
Management
Most neurologists now start
antiepileptics following a second epileptic seizure.
As a general rule:
·
sodium valproate is used first-line for patients with
generalised seizures
·
carbamazepine is used first-line for patients with partial
seizures
Antiepileptics are one of the few
drugs where it is recommended that we prescribe by brand, rather than generically, due to
the risk of slightly different bioavailability resulting in a lowered seizure
threshold.
It is useful when thinking about
the management of epilepsy to consider certain groups of patients:
·
patients who drive: generally patients cannot drive for
6 months following a seizure. For patients with established epilepsy they must
be fit free for 12 months before being able to drive
·
patients taking other medications: antiepileptics can induce/inhibit
the P450 system resulting in varied metabolism of other medications, for
example warfarin
·
women wishing to get pregnant: antiepileptics are generally
teratogenic, particularly sodium valproate. It is important that women take
advice from a neurologist prior to becoming pregnant, to ensure they are on the
most suitable antiepileptic medication. Breastfeeding is generally considered
safe for mothers taking antiepileptics with the possible exception of the
barbiturates
·
women taking contraception: both the effect of the
contraceptive on the effectiveness of the anti-epileptic medication and the
effect of the anti-epileptic on the effectiveness of the contraceptive need to
be considered
The table below looks at some of
the more commonly used antiepileptics:
|
Drug |
Mechanism of action |
Uses |
Adverse effects |
|
Sodium valproate |
Increases GABA activity |
First-line for generalised seizures |
·
increased appetite and weight gain ·
alopecia: regrowth may be curly ·
P450 enzyme inhibitor ·
ataxia ·
tremor ·
hepatitis ·
pancreatitis ·
thrombocytopaenia ·
teratogenic (neural tube defects) |
|
Carbamazepine |
Binds to sodium channels increasing
their refractory period |
First-line for partial seizures |
·
P450 enzyme inducer ·
dizziness and ataxia ·
drowsiness ·
leucopenia and agranulocytosis ·
syndrome of inappropriate ADH secretion ·
visual disturbances (especially diplopia) |
|
Lamotrigine |
Sodium channel blocker |
Used second-line for a variety of
generalised and partial seizures |
·
Stevens-Johnson syndrome |
|
Phenytoin |
Binds to sodium channels increasing
their refractory period |
No longer used first-line due to
side-effect profile |
·
P450 enzyme inducer ·
dizziness and ataxia ·
drowsiness ·
gingival hyperplasia, hirsutism, coarsening of facial features ·
megaloblastic anaemia ·
peripheral neuropathy ·
enhanced vitamin D metabolism causing osteomalacia ·
lymphadenopathy |
Acute management of seizures
Most seizures terminate
spontaneously. When seizures don't terminate after 5-10 minutes then it is
often appropriate to administer medication to terminate the seizure. Patients
are often prescribed these so family members may administer them in this
eventuality, often termed 'rescue medication'. Benzodiazepines such as diazepam are typically used are may be administered
rectally or intranasally/under the tongue.
If a patient continues to fit
despite such measures then they are termed to have status epilepticus. This is a medical emergency requiring hospital treatment.
Management options include further benzodiazepine medication, infusions of
antiepileptics or even the use of general anaesthetic agents.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Fourth nerve palsy
Overview
·
supplies superior oblique (depresses eye, moves inward)
Features
·
vertical diplopia
o classically noticed when reading a book or going downstairs
·
subjective tilting of objects (torsional
diplopia)
·
the patient may develop a head tilt, which they may or may not
be aware of
·
when looking straight ahead, the affected eye appears to deviate
upwards and is rotated outwards
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:19
Headache
Headache accounts for a large
proportion of medical consultations. The table below summarises the main
characteristics of common or important causes:
|
Condition |
Notes |
|
Migraine |
Recurrent, severe headache which is
usually unilateral and throbbing in nature May be be associated with aura, nausea
and photosensitivity Aggravated by, or causes avoidance of,
routine activities of daily living. Patients often describe 'going to bed'. In women may be associated with
menstruation |
|
Tension headache |
Recurrent, non-disabling, bilateral
headache, often described as a 'tight-band' Not aggravated by routine activities of
daily living |
|
Cluster headache* |
Pain typical occurs once or twice a
day, each episode lasting 15 mins - 2 hours with clusters typically lasting
4-12 weeks Intense pain around one eye (recurrent
attacks 'always' affect same side) Patient is restless during an attack Accompanied by redness, lacrimation,
lid swelling More common in men and smokers |
|
Temporal arteritis |
Typically patient > 60 years old Usually rapid onset (e.g. < 1 month)
of unilateral headache Jaw claudication (65%) Tender, palpable temporal artery Raised ESR |
|
Medication overuse headache |
Present for 15 days or more per month Developed or worsened whilst taking
regular symptomatic medication Patients using opioids and triptans are
at most risk May be psychiatric co-morbidity |
Other causes of headache
Acute single episode
·
meningitis
·
encephalitis
·
subarachnoid haemorrhage
·
head injury
·
sinusitis
·
glaucoma (acute closed-angle)
·
tropical illness e.g. Malaria
Chronic headache
·
chronically raised ICP
·
Paget's disease
·
psychological
*some neurologists use the term
trigeminal autonomic cephalgia to group a number of conditions including
cluster headache, paroxysmal hemicrania and short-lived unilateral neuralgiform
headache with conjunctival injection and tearing (SUNCT). It is recommended
such patients are referred for specialist assessment as specific treatment may
be required, for example it is known paroxysmal hemicrania responds very well
to indomethacin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
HSMN
Hereditary sensorimotor neuropathy
(HSMN) is a relatively new term which encompasses Charcot-Marie-Tooth disease
(also known as peroneal muscular atrophy). Over 7 types have been characterised
- however only 2 are common to clinical practice
·
HSMN type I: primarily due to demyelinating pathology
·
HSMN type II: primarily due to axonal pathology
HSMN type I
·
autosomal dominant
·
due to defect in PMP-22 gene (which codes for myelin)
·
features often start at puberty
·
motor symptoms predominate
·
distal muscle wasting, pes cavus, clawed toes
·
foot drop, leg weakness often first features
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Lambert-Eaton syndrome
Lambert-Eaton myasthenic syndrome
is seen in association with small
cell lung cancer and to a lesser extent breast and
ovarian cancer. It may also occur independently as an autoimmune disorder.
Lambert-Eaton myasthenic syndrome is caused by an antibody directed against
presynaptic voltage-gated calcium channel in the
peripheral nervous system.
Features
·
repeated muscle contractions lead to increased muscle strength
(in contrast to myasthenia gravis)
o in reality, this is seen in only
50% of patients and following prolonged muscle use muscle strength will
eventually decrease
·
limb-girdle weakness (affects lower limbs first)
·
hyporeflexia
·
autonomic symptoms: dry mouth, impotence, difficulty micturating
·
ophthalmoplegia and ptosis not commonly a feature (unlike in myasthenia
gravis)
EMG
·
incremental response to repetitive electrical stimulation
Management
·
treatment of underlying cancer
·
immunosuppression, for example with prednisolone and/or
azathioprine
·
3,4-diaminopyridine is currently being trialled
o works by blocking potassium channel
efflux in the nerve terminal so that the action potential duration is
increased. Calcium channels can then be open for a longer time and allow
greater acetylcholine release to the stimulate muscle at the end plate
·
intravenous immunoglobulin therapy and plasma exchange may be
beneficial
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Median nerve
The median nerve is formed by the
union of a lateral and medial root respectively from the lateral (C5,6,7) and
medial (C8 and T1) cords of the brachial plexus; the medial root passes
anterior to the third part of the axillary artery. The nerve descends lateral
to the brachial artery, crosses to its medial side (usually passing anterior to
the artery). It passes deep to the bicipital aponeurosis and the median cubital
vein at the elbow.
It passes between the two heads of
the pronator teres muscle, and runs on the deep surface of flexor digitorum
superficialis (within its fascial sheath).
Near the wrist it becomes
superficial between the tendons of flexor digitorum superficialis and flexor
carpi radialis, deep to palmaris longus tendon. It passes deep to the flexor
retinaculum to enter the palm, but lies anterior to the long flexor tendons
within the carpal tunnel.
Branches
|
Region |
Branch |
|
Upper arm |
No branches, although the nerve
commonly communicates with the musculocutaneous nerve |
|
Forearm |
Pronator teres Flexor carpi radialis Palmaris longus Flexor digitorum superficialis Flexor pollicis longus Flexor digitorum profundus (only the
radial half) |
|
Distal forearm |
Palmar cutaneous branch |
|
Hand (Motor) |
Motor supply (LOAF) ·
Lateral 2 lumbricals ·
Opponens pollicis ·
Abductor pollicis brevis ·
Flexor pollicis brevis |
|
Hand (Sensory) |
·
Over thumb and lateral 2 ½ fingers ·
On the palmar aspect this projects proximally, on
the dorsal aspect only the distal regions are innervated with the radial
nerve providing the more proximal cutaneous innervation. |
Patterns of damage
Damage at wrist
·
e.g. carpal tunnel syndrome
·
paralysis and wasting of thenar eminence muscles and opponens
pollicis (ape hand deformity)
·
sensory loss to palmar aspect of lateral (radial) 2 ½ fingers
Damage at elbow, as above plus:
·
unable to pronate forearm
·
weak wrist flexion
·
ulnar deviation of wrist
Anterior interosseous nerve (branch
of median nerve)
·
leaves just below the elbow
·
results in loss of pronation of forearm and weakness of long
flexors of thumb and index finger
Topography of the median nerve
|
|
|
|
Image
sourced from Wikipedia |
|
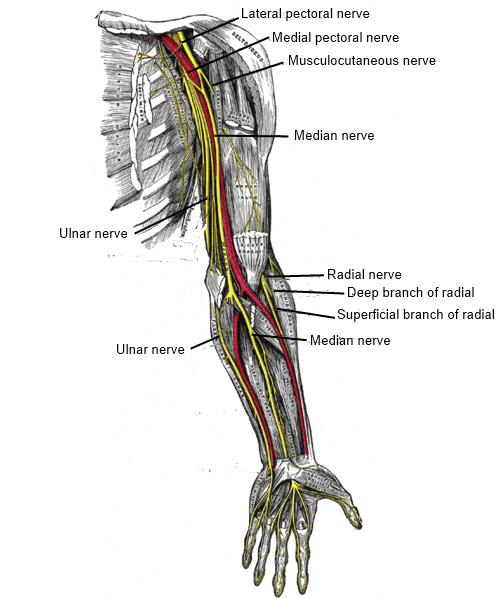
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Migraine: pregnancy, contraception and other hormonal
factors
SIGN produced guidelines in 2008 on
the management of migraine, the following is selected highlights:
Migraine during pregnancy
·
paracetamol 1g is first-line
·
NSAIDs can be used second-line in the first and second trimester
·
avoid aspirin and opioids such as codeine during pregnancy
Migraine and the combined oral
contraceptive (COC) pill
·
if patients have migraine with aura then the COC is absolutely
contraindicated due to an increased risk of stroke (relative risk 8.72)
Migraine and menstruation
·
many women find that the frequency and severity of migraines
increase around the time of menstruation
·
SIGN recommends that women are treated with mefanamic acid or a
combination of aspirin, paracetamol and caffeine. Triptans are also recommended
in the acute situation
Migraine and hormone replacement
therapy (HRT)
·
safe to prescribe HRT for patients with a history of migraine
but it may make migraines worse
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Myasthenia gravis: exacerbating factors
The most common exacerbating factor
is exertion resulting in fatigability, which is the hallmark feature of
myasthenia gravis . Symptoms become more marked during the day
The following drugs may exacerbate
myasthenia:
·
penicillamine
·
quinidine, procainamide
·
beta-blockers
·
lithium
·
phenytoin
·
antibiotics: gentamicin, macrolides, quinolones, tetracyclines
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Reflexes
The common reflexes are listed
below:
|
Reflex |
Root |
|
Ankle |
S1-S2 |
|
Knee |
L3-L4 |
|
Biceps |
C5-C6 |
|
Triceps |
C7-C8 |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Sodium valproate
Sodium valproate is used in the
management of epilepsy and is first-line therapy for generalised seizures. It
works by increasing GABA activity.
Adverse effects
·
teratogenic
o maternal use of sodium valproate is
associated with a significant risk of neurodevelopmental delay in children
o guidance is now clear that sodium
valproate should not be used during pregnancy and in women of childbearing age
unless clearly necessary. Women of childbearing age should not start treatment
without specialist neurological or psychiatric advice.
·
P450 inhibitor
·
gastrointestinal: nausea
·
increased appetite and weight gain
·
alopecia: regrowth may be curly
·
ataxia
·
tremor
·
hepatotoxicity
·
pancreatitis
·
thrombocytopaenia
·
hyponatraemia
·
hyperammonemic encephalopathy: L-carnitine may be used as treatment if this
develops
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Spinal cord lesions
The diagram belows shows
cross-section view of the spinal cord:
|
|
|
|
Image
sourced from Wikipedia |
|

Motor lesions
Amyotrophic lateral sclerosis (motor neuron
disease)
·
affects both upper (corticospinal tracts) and lower motor
neurons
·
results in a combination of upper and lower motor neuron signs
Poliomyelitis
·
affects anterior horns resulting in lower motor neuron signs
Combined motor and sensory lesions
|
Disorder |
Tracts affected |
Clinical notes |
|
Brown-Sequard syndrome (spinal cord hemisection) |
1. Lateral corticospinal tract 2. Dorsal columns 3. Lateral spinothalamic tract |
1. Ipsilateral spastic paresis below
lesion 2. Ipsilateral loss of proprioception
and vibration sensation 3. Contralateral loss of pain and
temperature sensation |
|
Subacute combined degeneration of the
spinal cord (vitamin B12 & E deficiency) |
1. Lateral corticospinal tracts 2. Dorsal columns 3. Spinocerebellar tracts |
1. Bilateral spastic paresis 2. Bilateral loss of proprioception and
vibration sensation 3. Bilateral limb ataxia |
|
Friedrich's ataxia |
Same as subacute combined degeneration of the spinal cord (see above) |
Same as subacute combined degeneration
of the spinal cord (see above) In addition cerebellar ataxia → other
features e.g. intention tremor |
|
Anterior spinal
artery occlusion |
1. Lateral corticospinal tracts 2. Lateral spinothalamic tracts |
1. Bilateral spastic paresis 2. Bilateral loss of pain and
temperature sensation |
|
Syringomyelia |
1. Ventral horns 2. Lateral spinothalamic tract |
1. Flacid paresis (typically affecting
the intrinsic hand muscles) 2. Loss of pain and temperature
sensation |
|
Multiple sclerosis |
Asymmetrical, varying spinal tracts
involved |
Combination of motor, sensory and
ataxia symptoms |
Sensory lesions
|
Disorder |
Tracts affected |
Clinical notes |
|
Neurosyphilis (tabes dorsalis) |
1. Dorsal columns |
1. Loss of proprioception and vibration
sensation |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Stroke management: other issues
This background note focuses on
other issues in acute stroke management, particularly management of fluids,
glycaemic control, blood pressure management, feeding assessment/management and
disability scales.
Fluid management
·
As in all patients in hospital, regular assessment for fluid
status must be undertaken to ensure patients remain normovolaemic
·
The NICE guidelines recommend assessing the hydration of all
patients with acute stroke on admission, with regular review during their stay
·
Greater than 80% of patients who cannot swallow post stroke will
recover within 2-4 weeks
·
However, it is important to manage fluids in this immediate
post-event period as hypovolaemia can worsen the ischaemic penumbra, as well as
increase risk of other complications such as infection, deep vein thrombosis,
constipation and delirium
·
Conversely, over-hydration can also complicate matters by
leading to cerebral oedema, cardiac failure and hyponatraemia, therefore it is
important to regularly review fluid status in these patients
·
Recommendations for management:
o Oral hydration is preferable in all
patients who are able to safely swallow
o Intravenous hydration may be
necessary otherwise, and although studies have remained contentious regarding
choice of intravenous fluid, UptoDate currently recommend isotonic saline
without dextrose as the agent of choice in most patients
o Other factors to take into
consideration when choosing fluid agent include electrolyte disturbances and/or
cardiovascular status
Glycaemic control
·
It is important to closely monitor and control blood sugar,
particularly if they are nil by mouth due to concerns regarding swallowing
safety post stroke, and/or in diabetics
·
Post stroke, patients with hyperglycaemia have increased
mortality independent from their age and the severity of stroke
o This is likely due to increased
tissue acidosis from anaerobic metabolism, free radical generation, and
increased blood brain barrier permeability post injury
·
The NICE guidelines recommend maintaining a blood sugar level between
4 and 11 mmol/L in people with acute stroke
·
Diabetic patients
o It is important to provide
intensive management for diabetics post acute stroke
o The NICE guidelines suggest
optimising insulin treatment using intravenous insulin and glucose infusions
o Hypoglycaemia also needs to be
managed appropriately, as alone it can cause neuronal injury as well as mimic
stroke-related neurological deficits
Blood pressure management
·
Use of anti-hypertensive medications should only be used for
blood pressure control in patients post ischaemic stroke if there is a
hypertensive emergency with one or more of the following serious concomitant
medical issues (according to the NICE guidelines):
o Hypertensive encephalopathy
o Hypertensive nephropathy
o Hypertensive cardiac
failure/myocardial infarction
o Aortic dissection
o Pre-eclampsia/eclampsia
·
This is because lowering blood pressure too much can potentially
compromise collateral blood flow to the affected region, and possibly hasten
the time to complete and irreversible tissue infarction
·
If if treatment is indicated, UptoDate recommend cautious
lowering of blood pressure by approximately 15% in the first 24-hours after
stroke onset
·
UptoDate suggest using intravenous labetalol, nicardipine and
clevidipine as first-line agents, due to the possibility for rapid and safe
titration to control blood pressure
·
However, in patients who are candidates for thrombolytic therapy
for acute stroke, blood pressure should be reduced to 185/110mmHg or lower
o Elevated BP can affect thrombolytic
eligibility and delay treatment
o Timely management of elevated BP is
crucial when patients are otherwise eligible for intravenous thrombolysis
o After thrombolytic therapy,
UptoDate recommend ensuring that the blood pressure is stabilised and maintained
at or below 180/105mmHg for at least 24 hours after treatment
Feeding assessment and management
·
All patients presenting with acute stroke must be screened for safe swallowing function prior to further oral
intake, as dysphagia is common after stroke
o This is to reduce the risk of
aspiration and subsequent complications
o This includes prior to any oral
intake of food, fluids, and/or medications
·
If there are any concerns regarding swallowing, the NICE
guidelines recommend specialist assessment of swallowing
o This should preferably within 24
hours of admission and not greater than 72 hours after
o Prior to assessment is undertaken,
a patient should remain nil by mouth to prevent complications
·
Recommendations for patients deemed unsafe for oral intake:
o Patients should receive nasogastric
tube feeding, ideally within 24 hours of admission, unless they have had
thrombolytic therapy
o If nasogastric tube feeding is not
tolerated, patients should be considered for a nasal bridle tube/gastrostomy
instead
o Medications need to be assessed to
determine if formulations are available for nasogastric feeding, or if
conversion to subcutaneous or intravenous forms are required
·
Nutritional support may be required for patients at risk of
malnutrition post stroke, whether a result from dysphagia, poor oral health or
reduced ability to self-feed due to weakness or paralysis
Disability scales
·
Stroke can result in a number of complications and subsequent
disability, therefore disability scales are often used as a measure of
functional decline post event and subsequent improvement after medical
intervention
·
Disability, often measured in terms of functional status
(notably, basic activities of daily living), is often the leading cause of
morbidity after stroke
·
After a patient is medically stabilised after a stroke, they may
require transfer to a rehabilitation team for ongoing treatment depending on
their level of disability
·
Disability is most commonly measured using the Barthel index (BI), an outcome measure for stroke
o Describes 10 tasks, and is scored
according to amount of time or assistance required by the patient for each
given task
o Tasks: feeding, moving from
wheelchair to bed, personal toileting, getting on/off toilet, bathing, walking
on level surface, ascending/descending stairs, dressing, controlling bowels and
controlling bladder
o The total score is from 0 to 100,
with 0 being completely dependent, and 100 being completely independent
·
This index should be used to assess the functional status of a
patient post stroke, and to monitor their improvement with ongoing
rehabilitation to regain independence after the event
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Ulnar nerve
Overview
·
arises from medial cord of brachial plexus (C8, T1)
Motor to
·
medial two lumbricals
·
aDductor pollicis
·
interossei
·
hypothenar muscles: abductor digiti minimi, flexor digiti minimi
·
flexor carpi ulnaris
Sensory to
·
medial 1 1/2 fingers (palmar and dorsal aspects)
Path
·
the ulnar nerve travels through the posteromedial aspect of the
upper arm to the flexor compartment of the forearm
·
it then enters the palm of the hand via the Guyon's canal, superficial to the flexor retinaculum and lateral to the
pisiform bone
|
|
|
|
Image
sourced from Wikipedia |
|
Branches
|
Branch |
Supplies |
|
Muscular branch |
Flexor carpi ulnaris Medial half of the flexor digitorum
profundus |
|
Palmar cutaneous branch (Arises near
the middle of the forearm) |
Skin on the medial part of the palm |
|
Dorsal cutaneous branch |
Dorsal surface of the medial part of
the hand |
|
Superficial branch |
Cutaneous fibres to the anterior
surfaces of the medial one and one-half digits |
|
Deep branch |
Hypothenar muscles All the interosseous muscles Third and fourth lumbricals Adductor pollicis Medial head of the flexor pollicis
brevis |
Patterns of damage
Damage at wrist
·
'claw hand' - hyperextension of the metacarpophalangeal joints
and flexion at the distal and proximal interphalangeal joints of the 4th and
5th digits
·
wasting and paralysis of intrinsic hand muscles (except lateral
two lumbricals)
·
wasting and paralysis of hypothenar muscles
·
sensory loss to the medial 1 1/2 fingers (palmar and dorsal
aspects)
Damage at elbow
·
as above (however, ulnar paradox - clawing is more severe in
distal lesions)
·
radial deviation of wrist
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Absence seizures
Absence seizures (petit mal) are a
form of generalised epilepsy that is mostly seen in children. The typical age
of onset of 3-10 years old and girls are affected twice as commonly as boys
Features
·
absences last a few seconds and are associated with a quick recovery
·
seizures may be provoked by hyperventilation or stress
·
the child is usually unaware of the seizure
·
they may occur many times a day
·
EEG: bilateral, symmetrical 3Hz
spike and wave pattern
Management
·
sodium valproate and ethosuximide are first-line treatment
·
good prognosis - 90-95% become seizure free in adolescence
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Brachial plexus injuries
Erb-Duchenne paralysis
·
damage to C5,6 roots
·
winged scapula
·
may be caused by a breech presentation
Klumpke's paralysis
·
damage to T1
·
loss of intrinsic hand muscles
·
due to traction
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Brown-Sequard syndrome
Overview
·
caused by lateral hemisection of the spinal cord
Features
·
ipsilateral weakness below lesion
·
ipsilateral loss of proprioception and vibration sensation
·
contralateral loss of pain and temperature sensation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Cataplexy
Cataplexy describes the sudden and transient loss of
muscular tone caused by strong emotion (e.g. laughter, being frightened). Around two-thirds of patients
with narcolepsy have cataplexy.
Features range from buckling knees
to collapse.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Cavernous sinus
The cavernous sinuses are paired
and are situated on the body of the sphenoid bone. It runs from the superior
orbital fissure to the petrous temporal bone.
Relations
|
Medial |
Lateral |
|
Pituitary fossa Sphenoid sinus |
Temporal lobe |
Contents
|
Lateral
wall components |
(from top to bottom:) Oculomotor nerve Trochlear nerve Ophthalmic nerve Maxillary nerve |
|
Contents of the sinus |
(from medial to lateral:) Internal carotid artery (and
sympathetic plexus) Abducens nerve |
Blood supply
Ophthalmic vein, superficial
cortical veins, basilar plexus of veins posteriorly.
Drains into the internal jugular
vein via: the superior and inferior petrosal sinuses
|
|
|
|
Image
sourced from Wikipedia |
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Cerebellar syndrome
Unilateral cerebellar lesions cause
ipsilateral signs.
Useful and well-known mnemonic to
remember symptoms of cerebellar disease is DANISH:
·
D - Dysdiadochokinesia, Dysmetria (past-pointing), patients may
appear 'Drunk'
·
A - Ataxia (limb, truncal)
·
N - Nystamus (horizontal = ipsilateral
hemisphere)
·
I - Intention tremour
·
S - Slurred staccato speech, Scanning
dysarthria
·
H - Hypotonia
Causes
·
Friedreich's ataxia, ataxic telangiectasia
·
neoplastic: cerebellar haemangioma
·
stroke
·
alcohol
·
multiple sclerosis
·
hypothyroidism
·
drugs: phenytoin, lead poisoning
·
paraneoplastic e.g. secondary to lung cancer
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Cerebral perfusion pressure
The cerebral perfusion pressure
(CPP) is defined as being the net pressure gradient causing blood flow to the
brain. The CPP is tightly autoregulated to maximise cerebral perfusion. A sharp
rise in CPP may result in a rising ICP, a fall in CPP may result in
cerebral ischaemia. It may be calculated by the
following equation:
CPP= Mean arterial pressure - Intra
cranial pressure
Following trauma, the CPP has to be
carefully controlled and the may require invasive monitoring of the ICP and
MAP.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Cerebrospinal fluid
The CSF fills the space between the
arachnoid mater and pia mater (covering surface of the brain). The total volume
of CSF in the brain is approximately 150ml. Approximately 500 ml is produced by
the ependymal cells in the choroid plexus (70%), or blood vessels (30%). It is
reabsorbed via the arachnoid granulations which project into the venous
sinuses.
Circulation
1. Lateral ventricles (via foramen
of Munro)
2. 3rd ventricle
3. Cerebral aqueduct (aqueduct of
Sylvius)
4. 4th ventricle (via foramina of
Magendie and Luschka)
5. Subarachnoid space
6. Reabsorbed into the venous
system via arachnoid granulations into superior sagittal sinus
Composition
·
Glucose: 50-80mg/dl
·
Protein: 15-40 mg/dl
·
Red blood cells: Nil
·
White blood cells: 0-3 cells/ mm3
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Charcot-Marie-Tooth disease
Charcot-Marie-Tooth Disease is the most common hereditary peripheral
neuropathy. It results in a predominantly motor loss. There is no
cure, and management is focused on physical and occupational therapy.
Features:
·
There may be a history of frequently sprained ankles
·
Foot drop
·
High-arched feet (pes cavus)
·
Hammer toes
·
Distal muscle weakness
·
Distal muscle atrophy
·
Hyporeflexia
·
Stork leg deformity
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
CNS tumours
- 60% = Glioma and metastatic
disease
·
20% = Meningioma
·
10% = Pituitary lesions
In paediatric practice
medulloblastomas (neuroectodermal tumours) were the commonest lesions,
astrocytomas now account for the majority.
Tumours arising in right temporal
and frontal lobe may reach considerable size before becoming symptomatic.
Whereas tumours in the speech and visual areas will typically produce early
symptoms.
Diagnosis
MRI Scanning provides the best
resolution.
Treatment
Usually surgery, even if tumour
cannot be completely resected conditions such as rising ICP can be addressed
with tumour debulking and survival and quality of life prolonged.
Curative surgery can usually be
undertaken with lesions such as meningiomas. Gliomas have a marked propensity
to invade normal brain and resection of these lesions is nearly always
incomplete.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Complex regional pain syndrome
Complex regional pain syndrome
(CRPS) is the modern, umbrella term for a number of conditions such as reflex
sympathetic dystrophy and causalgia. It describes a number of neurological and
related symptoms which typically occur following surgery or a minor injury.
CRPS is 3 times more common in women.
There are two types of CRPS:
·
type I (most common): there is no demonstrable lesion to a major
nerve
·
type II: there is a lesion to a major nerve
Features
·
progressive, disproportionate symptoms to the original
injury/surgery
·
allodynia
·
temperature and skin colour changes
·
oedema and sweating
·
motor dysfunction
·
the Budapest Diagnostic Criteria are commonly used in the UK
Management
·
early physiotherapy is important
·
neuropathic analgesia in-line with NICE guidelines
·
specialist management (e.g. Pain team) is required
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Dystrophinopathies
Overview
·
X-linked recessive
·
due to mutation in the gene encoding dystrophin, dystrophin gene
on Xp21
·
dystrophin is part of a large membrane associated protein in
muscle which connects the muscle membrane to actin, part of the muscle
cytoskeleton
·
in Duchenne muscular dystrophy there is a frameshift mutation
resulting in one or both of the binding sites are lost leading to a severe form
·
in Becker muscular dystrophy there is a non-frameshift insertion
in the dystrophin gene resulting in both binding sites being preserved leading
to a milder form
Duchenne muscular dystrophy
·
progressive proximal muscle weakness from 5 years
·
calf pseudohypertrophy
·
Gower's sign: child uses arms to stand up from a squatted
position
·
30% of patients have intellectual impairment
Becker muscular dystrophy
·
develops after the age of 10 years
·
intellectual impairment much less common
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Electromyography
Electromyography (EMG) is used to
evaluate the physiological properties of muscles at rest and whilst contracting
General characteristics of an
abnormal EMG are listed below
|
Condition |
Characteristic |
|
Neuropathy |
• Increased action potential duration • Increased action potential amplitude |
|
Myopathy |
• Decreased action potential duration • Decreased action potential amplitude |
Specific characteristics of
abnormal EMGs are shown in the table below
|
Condition |
Characteristic |
|
Myasthenia gravis |
Diminished response to repetitive
stimulation |
|
Lambert-Eaton syndrome |
Incremental response to repetitive
stimulation |
|
Myotonic syndromes |
extended series of repetitive
discharges lasting up to 30 seconds |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Encephalitis
Features
·
fever, headache, psychiatric symptoms, seizures, vomiting
·
focal features e.g. aphasia
·
peripheral lesions (e.g. cold sores) have no relation to
presence of HSV encephalitis
Pathophysiology
·
HSV-1 responsible for 95% of cases in adults
·
typically affects temporal and inferior frontal lobes
Investigation
·
CSF: lymphocytosis, elevated protein
·
PCR for HSV
·
CT: medial temporal and inferior frontal changes (e.g. petechial
haemorrhages) - normal in one-third of patients
·
MRI is better
·
EEG pattern: lateralised periodic discharges at 2 Hz
Management
·
intravenous aciclovir should be started in all cases of
suspected encephalitis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:20
Epilepsy in children: syndromes
Infantile spasms (West's syndrome)
·
brief spasms beginning in first few (4-6) months of life; M>F
·
1. Flexion of head, trunk, limbs → extension of arms (Salaam
attack); last 1-2 secs, repeat up to 50 times
·
2. Progressive mental handicap
·
3. EEG: hypsarrhythmia
·
usually 2nd to serious neurological abnormality (e.g. TS,
encephalitis, birth asphyxia) or may be cryptogenic
·
poor prognosis
·
vigabatrin/steroids
Typical (petit mal) absence
seizures
·
onset 4-8 yrs
·
duration few-30 secs; no warning, quick recovery; often many per
day
·
EEG: 3Hz generalized, symmetrical
·
sodium valproate, ethosuximide
·
good prognosis: 90-95% become seizure free in adolescence
Lennox-Gastaut syndrome
·
may be extension of infantile spasms (50% have hx)
·
onset 1-5 yrs
·
atypical absences, falls, jerks
·
90% moderate-severe mental handicap
·
EEG: slow spike
·
ketogenic diet may help
Benign rolandic epilepsy
·
most common in childhood, M>F
·
paraesthesia (e.g. unilateral face), usually on waking up
Juvenile myoclonic epilepsy (Janz
syndrome)
·
onset: teens; F:M = 2:1
·
1. Infrequent generalized seizures, often in morning
·
2. Daytime absences
·
3. Sudden, shock like myoclonic seizure (these
may develop before seizures)
·
usually good response to sodium valproate
Neonatal period - try vitamin B6
·
2nd: hypoglycaemia, meningitis, head trauma
·
pyridoxine dependency (AR, IV B6)
·
benign familial neonatal seizures (AD)
·
benign neonatal convulsions (5th day)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:21
Extradural haematoma
An extradural (or ‘epidural’)
haematoma is a collection of blood that is between the skull and the dura. It
is almost always caused by trauma and most typically by ‘low-impact’ trauma
(e.g. a blow to the head or a fall). The collection is often in the temporal
region since the thin skull at the pterion overlies the middle meningeal artery and is therefore vulnerable to injury.
The classical presentation is of a
patient who initially loses, briefly regains and then loses again consciousness
after a low-impact head injury. The brief regain in consciousness is termed the ‘lucid interval’ and is lost eventually due to the expanding haematoma and brain
herniation. As the haematoma expands the uncus of the temporal lobe herniates
around the tentorium cerebelli and the patient develops a fixed and dilated
pupil due to the compression of the parasympathetic fibers of the third cranial
nerve.
On imaging, an extradural haematoma
appears as a biconvex
(or lentiform), hyperdense collection around the
surface of the brain. They are limited
by the suture lines of the skull.
In patients who have no
neurological deficit, cautious clinical and radiological observation is
appropriate. The definitive treatment is craniotomy and evacuation of the
haematoma.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:21
Foot drop
Foot drop is a result of weakness
of the foot dorsiflexors.
Possible causes include:
·
common peroneal nerve lesion - the most common cause
·
L5 radiculopathy
·
sciatic nerve lesion
·
superficial or deep peroneal nerve lesion
·
other possible includes central nerve lesions (e.g. stroke) but
other features are usually present
A common peroneal nerve lesion is
the most common cause . This is often secondary to
compression at the neck of the fibula. This may be caused by certain positions
such as leg
crossing, squatting or kneeling. Prolonged confinement, recent
weight loss, Baker's cysts and plaster casts to the lower leg are also known to
be precipitating factors.
Examination
·
if the patient has an isolated peroneal neuropathy there will be
weakness of foot dorsiflexion and eversion. Reflexes will be normal
·
weakness of hip abduction is suggestive of a L5 radiculopathy
Bilateral symptoms, fasiculations
or other abnormal neurological findings (e.g. hyperreflexia) are indications
for specialist referral.
If the examination suggests a
peroneal neuropathy then conservative management is appropriate. Leg crossing,
squatting and kneeling should be avoided. Symptoms typically improve over 2-3
months.*
*BMJ 2015;350:h1736 - Foot drop
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:21
Guillain-Barre syndrome
Guillain-Barre syndrome describes
an immune mediated demyelination of the peripheral nervous system often
triggered by an infection (classically Campylobacter jejuni)
Pathogenesis
·
cross reaction of antibodies with gangliosides in the peripheral
nervous system
·
correlation between anti-ganglioside antibody (e.g. anti-GM1)
and clinical features has been demonstrated
·
anti-GM1 antibodies in 25% of patients
Miller Fisher syndrome
·
variant of Guillain-Barre syndrome
·
associated with ophthalmoplegia, areflexia and ataxia. The eye
muscles are typically affected first
·
usually presents as a descending paralysis rather than ascending
as seen in other forms of Guillain-Barre syndrome
·
anti-GQ1b antibodies are present in 90% of cases
From <https://www.passmedicine.com/review/textbook.php?s=#>
Guillian-Barré
Syndrome
GBS is
a rare condition, but is important to recognise as it can be life-threatening.
GBS will be covered in more detail in another tutorial.
The
take-home points for GBS are:
·
Often triggered by a
viral illness, commonly campylobacter gastroenteritis
·
Driven by an
auto-immune process causing demyelination of the nerves
·
Motor function and
muscle weakness is the most prominent feature
·
Pattern starts
distally and ascends inwards towards the body
·
Progresses for up to 4
weeks
·
The big threat is
weakness to the breathing and swallowing muscles
·
Treated with immune
modifying therapies
·
Recovery takes a LONG
time ("GBS - Gets Better Slowly")
The Time Place Type description
for this disease would be:
Acute
symmetrical diffuse sensorimotor polyneuropathy.
From <https://mle.ncl.ac.uk/cases/page/17650/>
24 December 2020
17:21
Internuclear ophthalmoplegia
Overview
·
a cause of horizontal disconjugate eye movement
·
due to a lesion in the medial longitudinal
fasciculus (MLF)
o controls horizontal eye movements
by interconnecting the IIIrd, IVth and VIth cranial nuclei
o located in the paramedian area of the midbrain and pons
Features
·
impaired adduction of the eye on the same side as the lesion
·
horizontal nystagmus of the abducting eye on the contralateral
side
Causes
·
multiple sclerosis
·
vascular disease
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:21
Intracranial venous thrombosis
Overview
·
can cause cerebral infarction, much lesson common than arterial
causes
·
50% of patients have isolated sagittal sinus thromboses - the
remainder have coexistent lateral sinus thromboses and cavernous sinus
thromboses
Features
·
headache (may be sudden onset)
·
nausea & vomiting
Sagittal sinus thrombosis
·
may present with seizures and hemiplegia
·
parasagittal biparietal or bifrontal haemorrhagic infarctions
are sometimes seen
Cavernous sinus thrombosis
·
other causes of cavernous sinus syndrome: local infection (e.g.
sinusitis), neoplasia, trauma
·
periorbital oedema
·
ophthalmoplegia: 6th nerve damage typically occurs before 3rd
& 4th
·
trigeminal nerve involvement may lead to hyperaesthesia of upper
face and eye pain
·
central retinal vein thrombosis
Lateral sinus thrombosis
·
6th and 7th cranial nerve palsies
|
|
|
|
©
Image used on license from Radiopaedia |
|

CT with contrast demonstrating a superior sagittal sinus
thrombosis showing the typical empty delta
sign. Look at the 'bottom' of the scan for the triangular shaped dural sinus.
This should normally be white due to it being filled with contrast. The empty
delta sign occurs when the thrombus fails to enhance within the dural sinus and
is outlined by enhanced collateral channels in the falx. This sign is seen in
only about 25%-30% of cases but is highly diagnostic for sagittal sinus
thrombosis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:21
Lamotrigine
Lamotrigine is an antiepileptic
used second-line for a variety of generalised and partial seizures.
Mechanism of action
·
sodium channel blocker
Adverse effects
·
Stevens-Johnson syndrome
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Levodopa
Overview
·
usually combined with a decarboxylase inhibitor (e.g. carbidopa
or benserazide) to prevent peripheral metabolism of L-dopa to dopamine
·
reduced effectiveness with time (usually by 2 years)
·
no use in neuroleptic induced parkinsonism
Adverse effects
·
dyskinesia
·
'on-off' effect
·
postural hypotension
·
cardiac arrhythmias
·
nausea & vomiting
·
psychosis
·
reddish discolouration of urine upon standing
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Migraine
Migraine is a common type of
primary headache. It is characterised typically by:
·
a severe, unilateral, throbbing headache
·
associated with nausea, photophobia and phonophobia
·
attacks may last up to 72 hours
·
patients characteristically go to a darkened, quiet room during
an attack
·
'classic' migraine attacks are precipitated by an aura. These
occur in around one-third of migraine patients
·
typical aura are visual, progressive, last 5-60 minutes and are
characterised by transient hemianopic disturbance or a spreading scintillating
scotoma
·
formal diagnostic criteria are produced by the International
Headache Society (see below)
Epidemiology
·
3 times more common in women
·
prevalence in men is around 6%, in women 18%
Common triggers for a migraine
attack
·
tiredness, stress
·
alcohol
·
combined oral contraceptive pill
·
lack of food or dehydration
·
cheese, chocolate, red wines, citrus fruits
·
menstruation
·
bright lights
Migraine diagnostic criteria
|
A |
At least 5 attacks fulfilling criteria
B-D |
|
B |
Headache attacks lasting 4-72 hours*
(untreated or unsuccessfully treated) |
|
C |
Headache has at least two of the
following characteristics: ·
1. unilateral location* ·
2. pulsating quality (i.e., varying with the heartbeat) ·
3. moderate or severe pain intensity ·
4. aggravation by or causing avoidance of routine
physical activity (e.g., walking or climbing stairs) |
|
D |
During headache at least one of the
following: ·
1. nausea and/or vomiting* ·
2. photophobia and phonophobia |
|
E |
Not attributed to another disorder
(history and examination do not suggest a secondary headache disorder or, if
they do, it is ruled out by appropriate investigations or headache attacks do
not occur for the first time in close temporal relation to the other
disorder) |
*In children, attacks may be
shorter-lasting, headache is more commonly bilateral, and gastrointestinal
disturbance is more prominent.
From <https://www.passmedicine.com/review/textbook.php?s=#>
The
mnemonic CHOCOLATE is useful for remembering the common precipitants.
·
Chocolate
·
Hangovers
·
Orgasms
·
Cheese
·
Caffeine
·
The oral contraceptive
pill
·
Lie-ins
·
Alcohol
·
Travel
·
Exercise
From <https://www.passmedicine.com/question/questions.php?q=0>
24 December 2020
17:22
Motor neuron disease: management
Motor neuron disease is a
neurological condition of unknown cause which can present with both upper and
lower motor neuron signs. It rarely presents before 40 years and various
patterns of disease are recognised including amyotrophic lateral sclerosis,
progressive muscular atrophy and bulbar palsy
Riluzole
·
prevents stimulation of glutamate receptors
·
used mainly in amyotrophic lateral sclerosis
·
prolongs life by about 3 months
Respiratory care
·
non-invasive ventilation (usually BIPAP) is used at night
·
studies have shown a survival benefit of around 7 months
Prognosis
·
poor: 50% of patients die within 3 years
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Multiple sclerosis: investigation
Diagnosis requires demonstration of
lesions disseminated in time and space
MRI with contrast should be used
to view demyelinating lesions
MRI
·
high signal T2 lesions
·
periventricular plaques
·
Dawson fingers: often seen on FLAIR images - hyperintense
lesions penpendicular to the corpus callosum
CSF
·
oligoclonal bands (and not in serum)
·
increased intrathecal synthesis of IgG
Visual evoked potentials
·
delayed, but well preserved waveform
|
|
|
|
©
Image used on license from Radiopaedia |
|

MRI showing multiple white matter plaques penpendicular
to the corpus callosum giving the appearance of Dawson fingers
|
|
|
|
©
Image used on license from Radiopaedia |
|

MRI from a young patient with multiple sclerosis.
Widespread periventricular, juxtacortical, post fossa and upper cervical cord
high T2 regions are noted. Note the difference in the lesions with varying
degrees of contrast enhancement and restricted diffusion indicating active/recent
demyelination. This satisfies the diagnostic criteria in terms of separation in
terms of time space.
|
|
|
|
©
Image used on license from Radiopaedia |
|

MRI FLAIR from the same patient as above. The numerous
lesions are more easily identified than in the above T2 image.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Narcolepsy
Overview
·
associated with HLA-DR2
·
it is associated with low levels of orexin
(hypocretin), a protein which
is responsible for controlling appetite and sleep patterns
·
early onset of REM sleep
Features
·
typical onset in teenage years
·
hypersomnolence
·
cataplexy (sudden loss of muscle tone often triggered by
emotion)
·
sleep paralysis
·
vivid hallucinations on going to sleep or waking up
Investigation
·
multiple sleep latency EEG
Management
·
daytime stimulants (e.g. modafinil) and nighttime sodium oxybate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Nutrition - Refeeding syndrome
Refeeding syndrome describes the
metabolic abnormalities which occur on feeding a person following a period of
starvation. The metabolic consequences include:
·
Hypophosphataemia
·
Hypokalaemia
·
Hypomagnesaemia
·
Abnormal fluid balance
These abnormalities can lead to
organ failure.
Re-feeding problems
If patient not eaten for > 5
days, aim to re-feed at < 50% energy and protein levels
High risk for re-feeding problems
If one or more of the following:
·
BMI < 16 kg/m2
·
Unintentional weight loss >15% over 3-6 months
·
Little nutritional intake > 10 days
·
Hypokalaemia, Hypophosphataemia or hypomagnesaemia prior to
feeding (unless high)
If two or more of the following:
·
BMI < 18.5 kg/m2
·
Unintentional weight loss > 10% over 3-6 months
·
Little nutritional intake > 5 days
·
History of: alcohol abuse, drug therapy including insulin,
chemotherapy, diuretics and antacids
Prescription
·
Start at up to 10 kcal/kg/day increasing to full needs over 4-7
days
·
Start immediately before and during feeding: oral thiamine
200-300mg/day, vitamin B co strong 1 tds and supplements
·
Give K+ (2-4 mmol/kg/day), phosphate
(0.3-0.6 mmol/kg/day), magnesium (0.2-0.4 mmol/kg/day)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Paroxysmal hemicrania
Paroxysmal hemicrania (PH) is
defined by attacks of severe, unilateral headache, usually in the orbital,
supraorbital or temporal region. These attacks are often associated with
autonomic features, usually last less than 30 minutes and can occur multiple
times a day.
PH sits within the group of
disorders called trigeminal autonomic cephalgias which also contains cluster
headache, a condition which shares many features with PH.
Importantly, PH is completely
responsive to treatment with indomethacin.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Post-lumbar puncture headache
Headache following lumbar puncture
(LP) occurs in approximately one-third of patients. The pathophysiology of is
unclear but may relate to a 'leak' of CSF following dural puncture. Post-LP
headaches are more common in young females with a low body mass index
Typical features
·
usually develops within 24-48 hours following LP but may occur
up to one week later
·
may last several days
·
worsens with upright position
·
improves with recumbent position
|
Factors
which may contribute to headache |
Factors which do not contribute to
headache |
|
Increased needle size Direction of bevel Not replacing the stylet Increased number of LP attempts |
Increased volume of CSF removed Bed rest following procedure Increased fluid intake post procedure Opening pressure of CSF Position of patient |
Management
·
supportive initially (analgesia, rest)
·
if pain continues for more than 72 hours then specific treatment
is indicated, to prevent subdural haematoma
·
treatment options include: blood patch, epidural saline and
intravenous caffeine
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Progressive supranuclear palsy
Overview
·
aka Steele-Richardson-Olszewski syndrome
·
a 'Parkinson Plus' syndrome
Features
·
postural instability and falls
o patients tend to have a stiff,
broad-based gait
·
impairment of vertical gaze (down gaze worse than up gaze -
patients may complain of difficultly reading or descending stairs)
·
parkinsonism
o bradykinesia is prominent
·
cognitive impairment
o primarily frontal lobe dysfunction
Management
·
poor response to L-dopa
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Raised intracranial pressure
As the brain and ventricles are
enclosed by a rigid skull, they have a limited ability to accommodate
additional volume. Additional volume (e.g. haematoma, tumour, excessive CSF)
will therefore lead to a rise in intracranial pressure (ICP).
Pathophysiology
·
the normal ICP is 7-15 mmHg in adults in the supine position
·
cerebral perfusion pressure (CPP) is the net pressure gradient
causing cerebral blood flow to the brain
·
CPP = mean arterial pressure - ICP
Causes
·
idiopathic intracranial hypertension
·
traumatic head injuries
·
infection
o meningitis
·
tumours
·
hydrocephalus
Features
·
headache
·
vomiting
·
reduced levels of consciousness
·
papilloedema
·
Cushing's triad
o widening pulse pressure
o bradycardia
o irregular breathing
Investigations and monitoring
·
neuroimaging (CT/MRI) is key to investigate the underlying cause
·
invasive ICP monitoring
o catheter placed into the lateral
ventricles of the brain to monitor the pressure
o may also be used to take collect
CSF samples and also to drain small amounts of CSF to reduce the pressure
o a cut-off of > 20 mmHg is often
used to determine if further treatment is needed to reduce the ICP
Management
·
investigate and treat the underlying cause
·
head elevation to 30º
·
IV mannitol may be used as an osmotic diuretic
·
controlled hyperventilation
o aim is to reduce pCO2 →
vasoconstriction of the cerebral arteries → reduced ICP
o leads to rapid, temporary lowering
of ICP. However, caution needed as may reduce blood flow to already ischaemic
parts of the brain
·
removal of CSF, different techniques include:
o drain from intraventricular monitor
(see above)
o repeated lumbar puncture (e.g.
idiopathic intracranial hypertension)
o ventriculoperitoneal shunt (for
hydrocephalus)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Restless legs syndrome
Restless legs syndrome (RLS) is a
syndrome of spontaneous, continuous lower limb movements that may be associated
with paraesthesia. It is extremely common, affecting between 2-10% of the
general population. Males and females are equally affected and a family history
may be present
Clinical features
·
uncontrollable urge to move legs (akathisia). Symptoms initially
occur at night but as condition progresses may occur during the day. Symptoms
are worse at rest
·
paraesthesias e.g. 'crawling' or 'throbbing' sensations
·
movements during sleep may be noted by the partner - periodic
limb movements of sleeps (PLMS)
Causes and associations
·
there is a positive family history in 50% of patients with
idiopathic RLS
·
iron deficiency anaemia
·
uraemia
·
diabetes mellitus
·
pregnancy
The diagnosis is clinical although
bloods such as ferritin to exclude iron deficiency anaemia may be appropriate
Management
·
simple measures: walking, stretching, massaging affected limbs
·
treat any iron deficiency
·
dopamine agonists are first-line treatment (e.g. Pramipexole, ropinirole)
·
benzodiazepines
·
gabapentin
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Seizures: acute management
Most seizures are self-limiting and
stop spontaneously but prolonged seizures may be potentially life-threatening.
Basics
·
check the airway and apply oxygen if appropriate
·
place the patient in the recovery position
·
if the seizure is prolonged give benzodiazepines
BNF recommend dose for rectal
diazepam, repeated once after 10-15 minutes if necessary
|
Neonate |
1.25 - 2.5 mg |
|
Child 1 month - 1 year |
5 mg |
|
Child 2 years - 11 years |
5 - 10 mg |
|
Child 12 years - 17 years |
10 mg |
|
Adult |
10 - 20 mg (max. 30 mg) |
|
Elderly |
10 mg (max. 15 mg) |
Midazolam oromucosal solution may
also be used:
|
Neonate |
300 mcg/kg (unlicensced) |
|
Child 1 - 2 months |
300 mcg/kg (max. 2.5mg, unlicensced) |
|
Child 3 - 11 months |
2.5 mg |
|
Child 1 - 4 years |
5 mg |
|
Child 5 - 9 years |
7.5 mg |
|
Child 10 - 17 years |
10 mg |
|
Adult |
10 mg (unlicensced) |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Spontaneous intracranial hypotension
Spontaneous intracranial
hypotension is a very rare cause of headaches that results from a CSF leak. The
leak is typically from the thoracic nerve root sleeves.
Risk factors include connective
tissue disorders such as Marfan's syndrome.
Key features
·
strong postural relationship with the headache generally much
worse when upright. Patients may, therefore, be bed-bound
Investigations
·
MRI with gadolinium: typically shows pachymeningeal enhancement
Management
·
usually conservative
·
if this fails an epidural blood patch may be tried
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:22
Stroke: a very basic introduction
Strokes represent an important
cause of morbidity and mortality. In the UK alone there are over 150,000
strokes per year, with over 1.2 million stroke survivors. Stroke is the fourth
largest cause of death in the UK and kills twice as many women than breast
cancer each year.
The prevention and treatment of
strokes has undergone significant changes over the past decade. What was
previously considered a devastating but untreatable condition is now viewed
more as a 'brain attack', a condition which requires emergency assessment to see
if patients may benefit from new treatments such as thrombolysis.
|
|
|
|
©
Image used on license from PathoPic |
|

Pathological specimen showing the results of an
ischaemic stroke to the occipito-parietal region of the cerebrum. Note there
has been some secondary haemorrhage in the affected area.
What is a stroke?
A stroke (also known as
cerebrovascular accident,CVA) represents a sudden interruption in the vascular
supply of the brain. Remember that neural tissue is completely dependent on
aerobic metabolism so any problem with oxygen supply can quickly lead to
irreversible damage.
There are two main types of
strokes:
·
ischaemic: these can be further subdivided between into episodes
which last greater than 24 hours (termed an ischaemic stroke) and episodes
where symptoms and signs last less than 24 hours (transient ischaemic attacks,
TIAs, sometimes termed 'mini-strokes' by patients)
·
haemorrhagic
The table below shows the basic
differences:
|
|
Ischaemic |
Haemorrhagic |
|
Essential problem |
'Blockage' in the blood vessel stops
blood flow |
Blood vessel 'bursts' leading to
reduction in blood flow |
|
Proportion of strokes |
85% |
15% |
|
Subtypes |
Thrombotic stroke ·
thrombosis from large vessels e.g. carotid Embolic stroke ·
usually a blood clot but fat, air or clumps of
bacteria may act as an embolus ·
atrial fibrillation is
an important cause of emboli forming in the heart |
Intracerebral haemorrhage ·
bleeding within the brain Subarachnoid haemorrhage ·
bleeding on the surface of the brain |
|
Risk factors |
General risk factors for cardiovascular
disease ·
age ·
hypertension ·
smoking ·
hyperlipidaemia ·
diabetes mellitus Risk factors for cardioembolism ·
atrial fibrillation |
Risk factors ·
age ·
hypertension ·
arteriovenous malformation ·
anticoagulation therapy |
Symptoms and signs
Stroke is defined by the World
Health Organization as a clinical syndrome consisting of 'rapidly developing
clinical signs of focal (at times global) disturbance of cerebral function,
lasting more than 24 hours or leading to death with no apparent cause other
than that of vascular origin'. In contrast, with a TIA the symptoms and signs
resolve within 24 hours.
Features include:
·
motor weakness
·
speech problems (dysphasia)
·
swallowing problems
·
visual field defects (homonymous hemianopia)
·
balance problems
Cerebral hemisphere infarcts may
have the following symptoms:
·
contralateral hemiplegia: initially flaccid then spastic
·
contralateral sensory loss
·
homonymous hemianopia
·
dysphasia
Brainstem infarction
·
may result in more severe symptoms including quadriplegia and
lock-in-syndrome
Lacunar infarcts
·
small infarcts around the basal ganglia, internal capsule,
thalamus and pons
·
this may result in pure motor, pure sensory, mixed motor and
sensory signs or ataxia
|
|
|
|
©
Image used on license from PathoPic |
|

An example of a lacunar infarct affecting the internal
capsule.
One formal classification system
that is sometimes used is the Oxford
Stroke Classification (also known as the Bamford
Classification), whichclassifies strokes based on the initial symptoms. A
summary is as follows:
The following criteria should be
assessed:
·
1. unilateral hemiparesis and/or hemisensory loss of the face,
arm & leg
·
2. homonymous hemianopia
·
3. higher cognitive dysfunction e.g. dysphasia
|
Stroke
type |
Notes |
|
Total anterior circulation infarcts
(TACI, c. 15%) |
·
involves middle and anterior cerebral arteries ·
all 3 of the above criteria are present |
|
Partial anterior circulation infarcts
(PACI, c. 25%) |
·
involves smaller arteries of anterior circulation
e.g. upper or lower division of middle cerebral artery ·
2 of the above criteria are present |
|
Lacunar infarcts (LACI, c. 25%) |
·
involves perforating arteries around the internal
capsule, thalamus and basal ganglia ·
presents with 1 of the following: ·
1. unilateral weakness (and/or sensory deficit) of
face and arm, arm and leg or all three. ·
2. pure sensory stroke. ·
3. ataxic hemiparesis |
|
Posterior circulation infarcts (POCI,
c. 25%) |
·
involves vertebrobasilar arteries ·
presents with 1 of the following: ·
1. cerebellar or brainstem
syndromes ·
2. loss of consciousness ·
3. isolated homonymous hemianopia |
Whilst symptoms alone cannot be
used to differentiate haemorrhagic from ischaemic strokes, patients who've
suffered haemorrhages are more likely to have:
·
decrease in the level of consciousness: seen in up to 50% of
patients with a haemorrhagic stroke
·
headache is also much more common in haemorrhagic stroke
·
nausea and vomiting is also common
·
seizures occur in up to 25% of patients
|
|
|
|
©
Image used on license from PathoPic |
|

Pathological specimen showing the consequence of an
intracerebral haemorrhage
Over recent years there has been a
public health campaign to raise awareness of stroke symptoms. The FAST campaign uses the following mnemonic:
·
Face - 'Has their face fallen on one side? Can they smile?'
·
Arms - 'Can they raise both arms and keep them there?'
·
Speech - 'Is their speech slurred?'
·
Ttime - 'Time to call 999 if you see any single one of these
signs.'
Investigations
Patients with suspected stroke need
to have emergency neuroimaging. The main cause for urgency is to see whether a
patient may be suitable for thrombolytic therapy to treat early ischaemic
strokes. The two types of neuroimaging used in this setting are:
·
CT
·
MRI
|
|
|
|
Image
sourced from Wikipedia |
|

CT scan of the brain showing a right-hemispheric
ischemic stroke
Management
Ischaemic strokes
Urgent neuroimaging classifies the
stroke as either ischaemic or haemorrhagic. If the stroke is ischaemic, and
certain criteria are met, the patient should be offered thrombolysis. Example criteria include:
·
patients present with 4.5 hours of onset of stroke symptoms
·
the patient has not had a previous intracranial haemorrhage,
uncontrolled hypertension, pregnant etc
Once haemorrhagic stroke has been
excluded patients should be given aspirin 300mg as soon as possible and antiplatelet
therapy should be continued.
Transient ischaemic attacks
Remember with TIAs the, by
definition, symptoms last less than 24 hours although in the vast majority of
cases the duration is much shorter, typically 1 hour or so. For this reason
most patients symptoms will have resolved before they see a doctor.
The ABCD2 prognostic score has
previously been used to risk stratify patients who present with a suspected
TIA. However, data from studies have suggested it performs poorly and it is
therefore no longer recommended by NICE Clinical Knowledge Summaries. Instead,
NICE recommend:
Immediate antithrombotic therapy:
·
give aspirin 300 mg immediately, unless contraindicated e.g. the
patient has a bleeding disorder or is taking an anticoagulant (needs immediate
admission for imaging to exclude a haemorrhage)
If the patient has had more than 1
TIA ('crescendo TIA') or has a suspected cardioembolic source or severe carotid
stenosis:
·
discuss the need for admission or observation urgently with a
stroke specialist
If the patient has had a suspected
TIA in the last 7 days:
·
arrange urgent assessment (within 24 hours) by a specialist
stroke physician
If the patient has had a suspected
TIA which occurred more than a week previously:
·
refer for specialist assessment as soon as possible within 7
days
Haemorrhagic strokes
If imaging confirms a haemorrhagic
stroke neurosurgical consultation should be considered for advice on further
management. The vast majority of patients however are not suitable for surgical
intervention. Management is therefore supportive as per haemorrhagic stroke.
Anticoagulants (e.g. warfarin) and antithrombotic medications (e.g. clopidogrel)
should be stopped to minimise further bleeding. If a patient is anticoagulated
this should be reversed as quickly as possible. Trials have shown improved
outcomes in patients who have their blood pressure lowered acutely and this is
now part of many protocols for haemorrhagic strokes.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
17:23
Multiple sclerosis: management
Treatment in multiple sclerosis is
focused at reducing the frequency and duration of relapses. There is no cure.
Acute relapse
High dose steroids (e.g. oral or IV
methylprednisolone) may be given for 5 days to shorten the length of an acute
relapse. It should be noted that steroids shorten the duration of a relapse and
do not alter the degree of recovery (i.e. whether a patient returns to baseline
function)
Disease modifying drugs
Beta-interferon has been shown to
reduce the relapse rate by up to 30%. Certain criteria have to be met before it
is used:
·
relapsing-remitting disease + 2 relapses in past 2 years + able
to walk 100m unaided
·
secondary progressive disease + 2 relapses in past 2 years +
able to walk 10m (aided or unaided)
·
reduces number of relapses and MRI changes, however doesn't
reduce overall disability
Other drugs used in the management
of multiple sclerosis include:
·
glatiramer acetate: immunomodulating drug - acts as an 'immune
decoy'
·
natalizumab: a recombinant monoclonal antibody that antagonises
Alpha-4 Beta-1-integrin found on the surface of leucocytes, thus inhibiting
migration of leucocytes across the endothelium across the blood-brain barrier
·
fingolimod: sphingosine 1-phosphate receptor modulator, prevents
lymphocytes from leaving lymph nodes. An oral formulation is available
Some specific problems
Fatigue
·
once other problems (e.g. anaemia, thyroid or depression) have
been excluded NICE recommend a trial of amantadine
·
other options include mindfulness training and CBT
Spasticity
·
baclofen and gabapentin are first-line. Other options include
diazepam, dantrolene and tizanidine
·
physiotherapy is important
·
cannabis and botox are undergoing evalulation
Bladder dysfunction
·
may take the form of urgency, incontinence, overflow etc
·
guidelines stress the importance of getting an ultrasound first
to assess bladder emptying - anticholinergics may worsen symptoms in some
patients
·
if significant residual volume → intermittent
self-catheterisation
·
if no significant residual volume → anticholinergics may improve
urinary frequency
Oscillopsia (visual fields apper to
oscillate)
·
gabapentin is first-line
From <https://www.passmedicine.com/review/textbook.php?s=#>
Tuesday, 22 December 2020
18:30
Subacute combined degeneration of spinal cord
Basics
·
due to vitamin B12 deficiency
·
dorsal + lateral columns affected
·
joint position and vibration sense lost first then distal
paraesthesia
·
upper motor neuron signs typically develop in the legs,
classically extensor plantars, brisk knee reflexes, absent ankle jerks
·
if untreated stiffness and weakness persist
21 December 2020
21:52
Stroke: management
The Royal College of Physicians
(RCP) published guidelines on the diagnosis and management of patients
following a stroke in 2004. NICE updated their stroke guidelines in 2019.
Selected points relating to the
management of acute stroke include:
·
blood glucose, hydration, oxygen saturation and temperature
should be maintained within normal limits
·
blood pressure should not be lowered in the acute phase unless there are
complications e.g. Hypertensive encephalopathy*
·
aspirin 300mg orally or rectally should be given as soon as
possible if a haemorrhagic stroke has been excluded
·
with regards to atrial fibrillation, the RCP state:
'anticoagulants should not be started until brain imaging has excluded
haemorrhage, and usually not until 14 days have passed from the onset of an
ischaemic stroke'
·
if the cholesterol is > 3.5 mmol/l patients should be
commenced on a statin. Many physicians will delay treatment until after at
least 48 hours due to the risk of haemorrhagic transformation
Thrombolysis for acute ischaemic
stroke
Thrombolysis with alteplase should
only be given if:
·
it is administered within 4.5 hours of onset of stroke symptoms (unless as part
of a clinical trial)
·
haemorrhage has been definitively excluded (i.e. Imaging has
been performed)
Contraindications to thrombolysis:
|
Absolute |
Relative |
|
- Previous intracranial haemorrhage - Seizure at onset of stroke - Intracranial neoplasm - Suspected subarachnoid haemorrhage - Stroke or traumatic brain injury in
preceding 3 months - Lumbar puncture in preceding 7 days - Gastrointestinal haemorrhage in
preceding 3 weeks - Active bleeding - Pregnancy - Oesophageal varices - Uncontrolled hypertension
>200/120mmHg |
- Concurrent anticoagulation (INR
>1.7) - Haemorrhagic diathesis - Active diabetic haemorrhagic
retinopathy - Suspected intracardiac thrombus - Major surgery / trauma in the
preceding 2 weeks |
Thrombectomy for acute ischaemic
stroke
Mechanical thrombectomy is an
exciting new treatment option for patients with an acute ischaemic stroke. NICE
incorporated recommendations into their 2019 guidelines. It is important to
remember the significant resources and senior personnel to provide such a
service 24 hours a day. NICE recommend that all decisions about thrombectomy
take into account a patient's overall clinical status:
·
NICE recommend a pre-stroke functional status of less than 3 on
the modified Rankin scale and a score of more than 5 on the National Institutes
of Health Stroke Scale (NIHSS)
Offer thrombectomy as soon as possible
and within 6
hours of symptom onset, together with intravenous thrombolysis (if
within 4.5 hours), to people who have:
acute ischaemic stroke and
·
confirmed occlusion of the proximal
anterior circulation demonstrated by computed tomographic angiography (CTA) or
magnetic resonance angiography (MRA)
Offer thrombectomy as soon as
possible to people who were last known to be well between 6 hours and 24 hours
previously (including wake-up strokes):
·
confirmed occlusion of the proximal
anterior circulation demonstrated by CTA or MRA and
·
if there is the potential to salvage brain tissue, as shown by imaging such as CT
perfusion or diffusion-weighted MRI sequences showing limited infarct core
volume
Consider thrombectomy
together with intravenous thrombolysis (if within 4.5 hours) as soon as
possible for people last known to be well up to 24 hours previously (including
wake-up strokes):
·
who have acute ischaemic stroke and confirmed occlusion of the proximal posterior circulation (that is, basilar or posterior
cerebral artery) demonstrated by CTA or MRA and
·
if there is the potential to salvage brain tissue, as shown by
imaging such as CT perfusion or diffusion-weighted MRI sequences showing
limited infarct core volume
Secondary prevention
NICE also published a technology
appraisal in 2010 on the use of clopidogrel and dipyridamole
Recommendations from NICE include:
·
clopidogrel is now recommended by NICE ahead of combination use of
aspirin plus modified-release (MR) dipyridamole in people who have had an
ischaemic stroke
·
aspirin plus MR dipyridamole is now recommended after an
ischaemic stroke only if clopidogrel is contraindicated or not tolerated, but
treatment is no longer limited to 2 years' duration
·
MR dipyridamole alone is recommended after an ischaemic stroke only if
aspirin or clopidogrel are contraindicated or not tolerated, again with no
limit on duration of treatment
With regards to carotid artery
endarterectomy:
·
recommend if patient has suffered stroke or TIA in the carotid territory and are not severely disabled
·
should only be considered if carotid stenosis > 70% according
ECST** criteria or > 50% according to NASCET*** criteria
*the 2009 Controlling hypertension
and hypotension immediately post-stroke (CHHIPS) trial may change thinking on
this but guidelines have yet to change to reflect this
**European Carotid Surgery
Trialists' Collaborative Group
***North American Symptomatic
Carotid Endarterectomy Trial
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:52
Visual field defects
The main points for the exam are:
·
left homonymous hemianopia means visual field defect to the
left, i.e. Lesion of right optic tract
·
homonymous quadrantanopias: PITS (Parietal-Inferior,
Temporal-Superior)
·
incongruous defects = optic tract lesion; congruous defects =
optic radiation lesion or occipital cortex
A congruous defect simply means
complete or symmetrical visual field loss and conversely an incongruous defect
is incomplete or asymmetric. Please see the link for an excellent diagram.
Homonymous hemianopia
·
incongruous defects: lesion of optic tract
·
congruous defects: lesion of optic radiation or occipital cortex
·
macula sparing: lesion of occipital cortex
Homonymous quadrantanopias*
·
superior: lesion of the inferior optic
radiations in the temporal lobe (Meyer's loop)
·
inferior: lesion of the superior optic radiations in the
parietal lobe
·
mnemonic = PITS (Parietal-Inferior, Temporal-Superior)
Bitemporal hemianopia
·
lesion of optic chiasm
·
upper quadrant defect > lower quadrant
defect = inferior chiasmal compression, commonly a pituitary tumour
·
lower quadrant defect > upper quadrant
defect = superior chiasmal compression, commonly a craniopharyngioma
*this is very much the 'exam
answer'. Actual studies suggest that the majority of quadrantanopias are caused
by occipital lobe lesions. Please see the link for more details.
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
23:04
Tremor
The table below lists the main
characteristics of the most important causes of tremor
|
Conditions |
Notes |
|
Parkinsonism |
Resting, 'pill-rolling' tremor Bradykinesia Rigidity Flexed posture, short, shuffling steps Micrographia 'Mask-like' face Depression & dementia are common May be history of anti-psychotic use |
|
Essential tremor |
Postural tremor: worse if arms
outstretched Improved by alcohol and rest Titubation Often strong family history |
|
Anxiety |
History of depression |
|
Thyrotoxicosis |
Usual thyroid signs e.g. Weight loss,
tachycardia, feeling hot etc |
|
Hepatic encephalopathy |
History of chronic liver disease |
|
Carbon dioxide retention |
History of chronic obstructive
pulmonary disease |
|
Cerebellar disease |
Intention tremor Cerebellar signs e.g. Past-pointing,
nystagmus etc |
Other causes
·
drug withdrawal: alcohol, opiates
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
16:35
Parkinsonism
Causes of Parkinsonism
·
Parkinson's disease
·
drug-induced e.g. antipsychotics, metoclopramide*
·
progressive supranuclear palsy
·
multiple system atrophy
·
Wilson's disease
·
post-encephalitis
·
dementia pugilistica (secondary to chronic head trauma e.g. boxing)
·
toxins: carbon monoxide, MPTP
*Domperidone does not cross the
blood-brain barrier and therefore does not cause extra-pyramidal side-effects.
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
19:18
Triptans
Triptans are specific 5-HT1B and 5-HT1D agonists used in the acute treatment of migraine. They are generally used
first-line in combination therapy with an NSAID or paracetamol.
Prescribing points
·
should be taken as soon as possible after
the onset of headache, rather than at onset of aura
·
oral, orodispersible, nasal spray and subcutaneous injections
are available
Adverse effects
·
'triptan sensations' - tingling, heat, tightness
(e.g. throat and chest), heaviness, pressure
Contraindications
·
patients with a history of, or significant risk factors for, ischaemic heart disease or cerebrovascular disease
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
19:20
Transient ischaemic attack
The original definition of a
transient ischaemic attack (TIA) was time-based: a sudden onset of a focal
neurologic symptom and/or sign lasting less than 24 hours, brought on by a
transient decrease in blood flow. However, this has now changed as it is recognised
that even short periods of ischaemia can result in pathological changes to the
brain. Therefore, a new 'tissue-based' definition is
now used: a transient episode
of neurologic dysfunction caused by focal brain, spinal cord, or retinal
ischaemia, without acute infarction.
Patients often use the term
'mini-stroke' for TIAs.
Assessment and referral
The ABCD2 prognostic score has
previously been used to risk stratify patients who present with a suspected
TIA. However, data from studies have suggested it performs poorly and it is
therefore no longer recommended by NICE Clinical Knowledge Summaries. Instead,
NICE recommend:
Immediate antithrombotic therapy:
·
give aspirin 300 mg immediately, unless
·
1. the patient has a bleeding disorder or is taking an
anticoagulant (needs immediate admission for imaging to
exclude a haemorrhage)
·
2. the patient is already taking low-dose aspirin regularly:
continue the current dose of aspirin until reviewed by a specialist
·
3. Aspirin is contraindicated: discuss management urgently with
the specialist team
If the patient has had more than 1
TIA ('crescendo TIA') or has a suspected cardioembolic source or severe carotid
stenosis:
·
discuss the need for admission or observation urgently with a
stroke specialist
If the patient has had a suspected
TIA in the last 7 days:
·
arrange urgent assessment (within 24 hours) by a specialist stroke
physician
If the patient has had a suspected
TIA which occurred more than a week previously:
·
refer for specialist assessment as soon as possible within 7
days
Advise the person not to drive
until they have been seen by a specialist.
Further management
Antithrombotic therapy
·
clopidogrel is recommended first-line (as for patients who've
had a stroke)
·
aspirin + dipyridamole should be given to patients who cannot
tolerate clopidogrel
·
these recommendations follow the 2012 Royal College of
Physicians National clinical guideline for stroke. Please see the link for more
details (section 5.5)
·
these guidelines may change following the CHANCE study (NEJM
2013;369:11). This study looked at giving high-risk TIA patients aspirin +
clopidogrel for the first 90 days compared to aspirin alone. 11.7% of aspirin
only patients had a stroke over 90 days compared to 8.2% of dual antiplatelet
patients
With regards to carotid artery
endarterectomy:
·
recommend if patient has suffered stroke or TIA in the carotid
territory and are not severely disabled
·
should only be considered if carotid
stenosis > 70% according ECST* criteria or > 50% according to NASCET**
criteria
*European Carotid Surgery
Trialists' Collaborative Group
**North American Symptomatic
Carotid Endarterectomy Trial
From <https://www.passmedicine.com/question/questions.php?q=0>
Wednesday, 23 December 2020
00:56
Brain abscess
Brain abscesses may result from a
number of causes including, extension of sepsis from middle ear or
sinuses, trauma or surgery to the scalp, penetrating head injuries
and embolic events from endocarditis
The presenting symptoms will depend
upon the site of the abscess (those in critical areas e.g. motor cortex) will
present earlier. Abscesses have a considerable mass effect in the brain and
raised intracranial pressure is common.
·
headache
o often dull, persistent
·
fever
o may be absent and usually not the
swinging pyrexia seen with abscesses at other sites
·
focal neurology
o e.g. oculomotor nerve palsy or
abducens nerve palsy secondary to raised intracranial pressure
·
other features consistent with raised intracranial pressure
o nausea
o papilloedema
o seizures
Investigations
·
Assessment of the patient includes imaging with CT scanning
Management
·
surgery
o a craniotomy is performed and the
abscess cavity debrided
o the abscess may reform because the
head is closed following abscess drainage.
·
IV antibiotics: IV 3rd-generation cephalosporin +
metronidazole
·
intracranial pressure management: e.g. dexamethasone
22 December 2020
19:33
Brain lesions
The following neurological
disorders/features may allow localisation of a brain lesion:
Gross anatomy
Parietal lobe lesions
·
sensory inattention
·
apraxias
·
astereognosis (tactile agnosia)
·
inferior homonymous quadrantanopia
·
Gerstmann's syndrome (lesion of dominant parietal): alexia, acalculia, finger agnosia and right-left
disorientation
Occipital lobe lesions
·
homonymous hemianopia (with macula sparing)
·
cortical blindness
·
visual agnosia
Temporal lobe lesion
·
Wernicke's aphasia: this area 'forms' the speech before 'sending
it' to Brocas area. Lesions result in word
substituion, neologisms but speech remains fluent
·
superior homonymous quadrantanopia
·
auditory agnosia
·
prosopagnosia (difficulty recognising faces)
Frontal lobes lesions
·
expressive (Broca's) aphasia: located on the posterior aspect of
the frontal lobe, in the inferior frontal gyrus. Speech is non-fluent,
laboured, and halting
·
disinhibition
·
perseveration
·
anosmia
·
inability to generate a list
Cerebellum lesions
·
midline lesions: gait and truncal ataxia
·
hemisphere lesions: intention tremor, past pointing,
dysdiadokinesis, nystagmus
More specific areas
|
Area |
Associated conditions |
|
Medial thalamus and mammillary bodies
of the hypothalamus |
Wernicke and Korsakoff syndrome |
|
Subthalamic nucleus of the basal
ganglia |
Hemiballism |
|
Striatum (caudate nucleus) of the basal
ganglia |
Huntington chorea |
|
Substantia nigra of the basal ganglia |
Parkinson's disease |
|
Amygdala |
Kluver-Bucy syndrome (hypersexuality,
hyperorality, hyperphagia, visual agnosia |
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
19:40
Cranial nerves
The table below lists the major
characteristics of the 12 cranial nerves:
From <https://www.passmedicine.com/question/questions.php?q=0#>
|
I
(Olfactory) |
Smell |
|
Cribriform plate |
|
II (Optic) |
Sight |
|
Optic canal |
|
III (Oculomotor) |
Eye movement (MR, IO, SR, IR) Pupil constriction Accomodation Eyelid opening |
Palsy results in ·
ptosis ·
'down and out' eye ·
dilated, fixed pupil |
Superior orbital fissure (SOF) |
|
IV (Trochlear) |
Eye movement (SO) |
Palsy results in defective downward
gaze → vertical diplopia |
SOF |
|
V (Trigeminal) |
Facial sensation Mastication |
Lesions may cause: ·
trigeminal neuralgia ·
loss of corneal reflex (afferent) ·
loss of facial sensation ·
paralysis of mastication muscles ·
deviation of jaw to weak side |
V1: SOF, V2: Foramen
rotundum, V3: Foramen ovale |
|
VI (Abducens) |
Eye movement (LR) |
Palsy results in defective abduction →
horizontal diplopia |
SOF |
|
VII (Facial) |
Facial movement Taste (anterior 2/3rds of tongue) Lacrimation Salivation |
Lesions may result in: ·
flaccid paralysis of upper + lower face ·
loss of corneal reflex (efferent) ·
loss of taste ·
hyperacusis |
Internal auditory meatus |
|
VIII (Vestibulocochlear) |
Hearing, balance |
Hearing loss Vertigo, nystagmus Acoustic neuromas are Schwann cell
tumours of the cochlear nerve |
Internal auditory meatus |
|
IX (Glossopharyngeal) |
Taste (posterior 1/3rd of tongue) Salivation Swallowing Mediates input from carotid body &
sinus |
Lesions may result in; ·
hypersensitive carotid sinus reflex ·
loss of gag reflex (afferent) |
Jugular foramen |
|
X (Vagus) |
Phonation Swallowing Innervates viscera |
Lesions may result in; ·
uvula deviates away from site of lesion ·
loss of gag reflex (efferent) |
Jugular foramen |
|
XI (Accessory) |
Head and shoulder movement |
Lesions may result in; ·
weakness turning head to contralateral side |
Jugular foramen |
|
XII (Hypoglossal) |
Tongue movement |
Tongue deviates towards side of lesion |
Hypoglossal canal |
Some
cranial nerves are motor, some sensory and some are both. The most useful
mnemonic is given below.
CN I
----------------------------------------------------------------------→XII
Some Say Marry Money But My Brother Says Big Brains Matter Most
S = Sensory, M = Motor, B = Both
|
|
|
|
Image
sourced from Wikipedia |
|

View from the inferior surface of the brain showing the
emergence of the cranial nerves
|
|
|
|
Image
sourced from Wikipedia |
|

Diagram showing the nuclei of the cranial nerves in the
brainstem
Cranial nerve
reflexes
|
Reflex |
Afferent limb |
Efferent limb |
|
Corneal |
Ophthalmic nerve (V1) |
Facial nerve (VII) |
|
Jaw jerk |
Mandibular nerve (V3) |
Mandibular nerve (V3) |
|
Gag |
Glossopharyngeal nerve (IX) |
Vagal nerve (X) |
|
Carotid sinus |
Glossopharyngeal nerve (IX) |
Vagal nerve (X) |
|
Pupillary light |
Optic nerve (II) |
Oculomotor nerve (III) |
|
Lacrimation |
Ophthalmic nerve (V1) |
Facial nerve (VII) |
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
19:52
Glasgow Coma Scale: adults
|
Modality |
Options |
|
Motor
response |
6. Obeys commands 5. Localises to pain 4. Withdraws from pain 3. Abnormal flexion to pain
(decorticate posture) 2. Extending to pain 1. None |
|
Verbal
response |
5. Orientated 4. Confused 3. Words 2. Sounds 1. None |
|
Eye
opening |
4. Spontaneous 3. To speech 2. To pain 1. None |
Glasgow coma scale (GCS) scores are
generally expressed in the following format 'GCS = 13, M5 V4 E4 at 21:30'.
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
20:16
Bell's palsy
Bell's palsy may be defined as an
acute, unilateral, idiopathic, facial nerve paralysis. The aetiology is unknown
although the role of the herpes simplex virus has been investigated previously.
The peak incidence is 20-40 years and the condition is more common in pregnant
women.
Features
·
lower motor neuron facial nerve palsy - forehead affected*
·
patients may also notice post-auricular pain (may precede
paralysis), altered taste, dry eyes, hyperacusis
Management
·
in the past a variety of treatment options have been proposed
including no treatment, prednisolone only and a combination of aciclovir and
prednisolone
·
following a National Institute for Health randomised controlled
trial it is now recommended that prednisolone 1mg/kg for 10 days should be
prescribed for patients within 72 hours of onset of Bell's palsy. Adding in
aciclovir gives no additional benefit
·
eye care is important - prescription of artificial tears and eye
lubricants should be considered
Prognosis
·
if untreated around 15% of patients have permanent moderate to
severe weakness
*upper motor neuron lesion 'spares'
upper face
From <https://www.passmedicine.com/question/questions.php?q=0#>
21 December 2020
21:51
Guillain-Barre syndrome: features
Guillain-Barre syndrome describes
an immune-mediated demyelination of the peripheral nervous system often
triggered by an infection (classically Campylobacter jejuni).
Initial symptoms
·
around 65% of patients experience back/leg
pain in the initial
stages of the illness
The characteristic features of
Guillain-Barre syndrome is progressive,
symmetrical weakness of all the limbs.
·
the weakness is classically ascending i.e. the legs are affected first
·
proximal muscles (e.g. hips/shoulders) are usually affected
before than the distal ones (e.g. feet/hands)
·
reflexes are reduced or absent
·
sensory symptoms tend to be mild (e.g. distal paraesthesia) with
very few sensory signs
Other features
·
there may be a history of gastroenteritis
·
respiratory muscle weakness
·
cranial nerve involvement
o diplopia
o bilateral facial nerve palsy
o oropharyngeal weakness is common
·
autonomic involvement
o urinary retention
o diarrhoea
Less common findings
·
papilloedema: thought to be secondary to reduced CSF resorption
Investigations
·
lumbar puncture
o rise in protein with a normal white
blood cell count (albuminocytologic dissociation) - found in 66%
·
nerve condution studies may be performed
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:51
DVLA: neurological disorders
The guidelines below relate to
car/motorcycle use unless specifically stated. For obvious reasons, the rules
relating to drivers of heavy goods vehicles tend to be much stricter
Epilepsy/seizures - all patient
must not drive and must inform the DVLA
·
first unprovoked/isolated seizure: 6
months off if there are
no relevant structural abnormalities on brain imaging and no definite
epileptiform activity on EEG. If these conditions are not met then this is
increased to 12 months
·
for patients with established epilepsy or those with multiple
unprovoked seizures:
·
→ may qualify for a driving licence if they have been free from
any seizure for 12 months
·
→ if there have been no seizures for 5 years (with medication if
necessary) a ’til 70 licence is usually restored
·
withdrawawl of epilepsy medication: should not drive whilst
anti-epilepsy medication is being withdrawn and for 6 months after the last
dose
Syncope
·
simple faint: no restriction
·
single episode, explained and treated: 4 weeks off
·
single episode, unexplained: 6 months off
·
two or more episodes: 12 months off
Other conditions
·
stroke or TIA: 1 month off driving, may not need to inform
DVLA if no residual neurological deficit
·
multiple TIAs over short period of times: 3 months off driving and inform DVLA
·
craniotomy e.g. For meningioma: 1 year off driving*
·
pituitary tumour: craniotomy: 6 months; trans-sphenoidal surgery
'can drive when there is no debarring residual impairment likely to affect safe
driving'
·
narcolepsy/cataplexy: cease driving on diagnosis, can restart
once 'satisfactory control of symptoms'
·
chronic neurological disorders e.g. multiple sclerosis, motor
neuron disease: DVLA should be informed, complete PK1 form (application for
driving licence holders state of health)
*if the tumour is a benign
meningioma and there is no seizure history, licence can be reconsidered 6
months after surgery if remains seizure free
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:51
Epilepsy: classification
The basic classification of
epilepsy has changed in recent years. The new basic seizure classification is
based on 3 key features:
·
1. Where seizures begin in the brain
·
2. Level of awareness during a seizure (important as can affect
safety during seizure)
·
3. Other features of seizures
Focal seizures
·
previously termed partial seizures
·
these start in a specific area, on one side of the brain
·
the level of awareness can vary in focal seizures. The
terms focal aware (previously termed 'simple partial'), focal impaired awareness (previously termed 'complex partial') and awareness
unknown are used to further describe focal seizures
·
further to this, focal seizures can be classified as being motor
(e.g. Jacksonian march), non-motor (e.g. déjà vu, jamais vu; ) or having other
features such as aura
Generalised
·
these engage or involve networks on both sides of the brain at
the onset
·
consciousness lost immediately. The level of awareness in the
above classification is therefore not needed, as all patients lose
consciousness
·
generalised seizures can be further subdivided into motor (e.g.
tonic-clonic) and non-motor (e.g. absence)
·
specific types include:
·
→ tonic-clonic (grand mal)
·
→ tonic
·
→ clonic
·
→ typical absence (petit mal)
·
→ atonic
Unknown onset
·
this termed is reserved for when the origin of the seizure is
unknown
Focal to bilateral seizure
·
starts on one side of the brain in a specific area before spreading
to both lobes
·
previously termed secondary generalized seizures
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:51
Epilepsy: treatment
Most neurologists now start
antiepileptics following a second epileptic seizure. NICE guidelines suggest
starting antiepileptics after the first seizure if any of the following are
present:
·
the patient has a neurological deficit
·
brain imaging shows a structural abnormality
·
the EEG shows unequivocal epileptic activity
·
the patient or their family or carers consider the risk of
having a further seizure unacceptable
It should be remembered that the following
are only general guidelines. For example, maternal use of sodium
valproate is associated with a significant risk of neurodevelopmental delay in
children. Guidance is now clear that sodium valproate should not
be used during pregnancy and in women of childbearing age unless clearly
necessary.
Sodium valproate is considered the
first line treatment for patients with generalised seizures with carbamazepine
used for focal seizures.
Generalised tonic-clonic seizures
·
sodium valproate
·
second line: lamotrigine, carbamazepine
Absence seizures* (Petit mal)
·
sodium valproate or ethosuximide
·
sodium valproate particularly effective if co-existent
tonic-clonic seizures in primary generalised epilepsy
Myoclonic seizures**
·
sodium valproate
·
second line: clonazepam, lamotrigine
Focal seizures
·
carbamazepine or lamotrigine
·
second line: levetiracetam, oxcarbazepine or sodium valproate
*carbamazepine may exacerbate absence
seizures
**carbamazepine may exacerbate myoclonic
seizures
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:52
Headache: red flags
Headache is one of the most common
presenting complaints seen in clinical practice. The vast majority of these
will be caused by common, benign conditions. There are however certain features
in a history which should prompt further action. In the 2012 guidelines NICE
suggest the following:
·
compromised immunity, caused, for example, by HIV or
immunosuppressive drugs
·
age under 20 years and a history of malignancy
·
a history of malignancy known to metastasis to the brain
·
vomiting without other obvious cause
·
worsening headache with fever
·
sudden-onset headache reaching maximum intensity within 5
minutes - 'thunderclap'
·
new-onset neurological deficit
·
new-onset cognitive dysfunction
·
change in personality
·
impaired level of consciousness
·
recent (typically within the past 3 months) head trauma
·
headache triggered by cough, valsalva (trying
to breathe out with nose and mouth blocked), sneeze or exercise
·
orthostatic headache (headache that changes with posture)
·
symptoms suggestive of giant cell arteritis or acute
narrow-angle glaucoma
·
a substantial change in the characteristics of their headache
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:52
Idiopathic intracranial hypertension
Idiopathic intracranial
hypertension (also known as pseudotumour cerebri and formerly benign
intracranial hypertension) is a condition classically seen in young, overweight
females.
Risk factors
·
obesity
·
female sex
·
pregnancy
·
drugs*: oral contraceptive pill, steroids, tetracycline, vitamin A, lithium
Features
·
headache
·
blurred vision
·
papilloedema (usually present)
·
enlarged blind spot
·
sixth nerve palsy may be present
Management
·
weight loss
·
diuretics e.g. acetazolamide
·
topiramate is also used, and has the added benefit of causing
weight loss in most patients
·
repeated lumbar puncture
·
surgery: optic nerve sheath decompression and fenestration may
be needed to prevent damage to the optic nerve. A lumboperitoneal or
ventriculoperitoneal shunt may also be performed to reduce intracranial
pressure
*if intracranial hypertension is
thought to occur secondary to a known causes (e.g. Medication) then it is of
course not idiopathic
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:52
Motor neuron disease: types
Motor neuron disease is a
neurological condition of unknown cause which can present with both upper and
lower motor neuron signs. It rarely presents before 40 years and various
patterns of disease are recognised including amyotrophic lateral sclerosis,
primary lateral sclerosis, progressive muscular atrophy and progressive bulbar
palsy. In some patients however, there is a combination of clinical patterns
Amyotrophic lateral sclerosis (50%
of patients)
·
typically LMN signs in arms and UMN signs in legs
·
in familial cases the gene responsible lies on chromosome 21 and
codes for superoxide dismutase
Primary lateral sclerosis
·
UMN signs only
Progressive muscular atrophy
·
LMN signs only
·
affects distal muscles before proximal
·
carries best prognosis
Progressive bulbar palsy
·
palsy of the tongue, muscles of chewing/swallowing and facial
muscles due to loss of function of brainstem motor nuclei
·
carries worst prognosis
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:52
Multiple sclerosis: features
Patient's with multiple sclerosis
(MS) may present with non-specific features, for example around 75% of patients have
significant lethargy.
Diagnosis can be made on the basis
of two or more relapses and either objective clinical evidence of two or more
lesions or objective clinical evidence of one lesion together with reasonable
historical evidence of a previous relapse.
Visual
·
optic neuritis: common presenting feature
·
optic atrophy
·
Uhthoff's phenomenon: worsening of vision following rise in body
temperature
·
internuclear ophthalmoplegia
Sensory
·
pins/needles
·
numbness
·
trigeminal neuralgia
·
Lhermitte's syndrome: paraesthesiae in limbs on neck flexion
Motor
·
spastic weakness: most commonly seen in the legs
Cerebellar
·
ataxia: more often seen during an acute relapse than as a
presenting symptom
·
tremor
Others
·
urinary incontinence
·
sexual dysfunction
·
intellectual deterioration
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
18:15
Ataxia
Cerebellar
hemisphere lesions cause peripheral ('finger-nose ataxia')
wide-based gait with loss of heel
to toe walking,
Cerebellar
vermis lesions cause gait ataxia
Ataxic
gaits are often caused by cerebellar lesions. The mnemonic 'PASTRIES' can be
used to remember the causes of an ataxic gait.
P
- paraneoplastic syndrome
A
- abscess/atrophy
S
- stroke/sclerosis (multiple sclerosis)
T
- trauma
R
- raised ICP
I
- infection
E
- ethanol and poisons
S
- spinocerebellar ataxia (progressive degenerative genetic disease)
Ataxic
gaits typically occur following cerebellar injury, the causes of which can be
remembered by the mnemonic 'pastries'
P
- Posterior fossa tumour
A
- Alcohol
S
- Multiple sclerosis
T
- Trauma
R
- Rare causes
I
- Inherited (e.g. Friedreich's ataxia)
E
- Epilepsy treatments
S
- Stroke
22 December 2020
19:07
Stroke: assessment
Whilst the diagnosis of stroke may
sometimes be obvious in many cases the presenting symptoms may be vague and
accurate assessment difficult.
The FAST screening tool
(Face/Arms/Speech/Time) is widely known by the general public following a
publicity campaign. It has a positive predictive value of 78%.
A variant of FAST called the ROSIER
score is useful for medical professionals. It is validated tool recommended by
the Royal College of Physicians.
ROSIER score
Exclude hypoglycaemia first, then
assess the following:
|
Assessment |
Scoring |
|
Loss of consciousness or syncope |
- 1 point |
|
Seizure activity |
- 1 point |
|
New, acute onset of: |
|
|
• asymmetric facial weakness |
+ 1 point |
|
• asymmetric arm weakness |
+ 1 point |
|
• asymmetric leg weakness |
+ 1 point |
|
• speech disturbance |
+ 1 point |
|
• visual field defect |
+ 1 point |
A stroke is likely if > 0.
Investigations
A non-contrast CT head scan is the first line radiological investigation for suspected
stroke
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
16:23
Essential tremor
Essential tremor (previously called
benign essential tremor) is an autosomal dominant condition which usually
affects both upper limbs
Features
·
postural tremor: worse if arms outstretched
·
improved by alcohol and rest
·
most common cause of titubation (head tremor)
Management
·
propranolol is first-line
·
primidone is sometimes used
From <https://www.passmedicine.com/question/questions.php?q=0>
Tuesday, 22 December 2020
22:45
Wernicke's encephalopathy
Wernicke's encephalopathy is a
neuropsychiatric disorder caused by thiamine deficiency which is most commonly
seen in alcoholics. Rarer causes include: persistent vomiting, stomach cancer,
dietary deficiency. A classic triad of ophthalmoplegia/nystagmus, ataxia and
confusion may occur. In Wernicke's encephalopathy petechial haemorrhages occur
in a variety of structures in the brain including the mamillary bodies and
ventricle walls.
Features
·
nystagmus (the most common ocular sign)
·
ophthalmoplegia
·
ataxia
·
confusion, altered GCS
·
peripheral sensory neuropathy
Investigations
·
decreased red cell transketolase
·
MRI
Treatment is with urgent
replacement of thiamine
Relationship with Korsakoff
syndrome
If not treated Korsakoff's syndrome
may develop as well. This is termed Wernicke-Korsakoff syndrome and is
characterised by the addition of antero- and retrograde amnesia and confabulation
in addition to the above symptoms.
|
|
|
|
A
useful mnemonic to remember the features of Wernicke's encephalopathy
is CAN
OPEN Confusion Ataxia Nystagmus Ophthamoplegia PEripheral Neuropathy Retrograde
amnesia and confabulation are features of Korsakoff's psychosis |
|
Wednesday, 23 December 2020
00:53
Cataplexy
Cataplexy describes the sudden
and transient loss of muscular tone caused by strong
emotion (e.g. laughter, being frightened). Around two-thirds of patients
with narcolepsy have cataplexy.
Features range from buckling knees
to collapse.
22 December 2020
20:39
Vestibular schwannoma (acoustic neuroma)
Vestibular schwannomas (sometimes
referred to as acoustic neuromas) account for approximately 5% of intracranial
tumours and 90% of cerebellopontine angle tumours.
The classical
history of vestibular schwannoma includes a combination of vertigo, hearing
loss, tinnitus and an absent corneal reflex. Features
can be predicted by the affected
cranial nerves:
·
cranial nerve VIII: vertigo, unilateral
sensorineural hearing loss, unilateral tinnitus
·
cranial nerve V: absent corneal reflex
·
cranial nerve VII: facial palsy
Bilateral vestibular schwannomas
are seen in neurofibromatosis type 2.
Patients with a suspected
vestibular schwannoma should be referred
urgently to ENT. It should be noted though that
the tumours are often slow growing, benign and often observed initially.
MRI of the cerebellopontine angle is the
investigation of choice. Audiometry is also important as only 5% of patients
will have a normal audiogram.
Management is with either surgery,
radiotherapy or observation.
From <https://www.passmedicine.com/question/questions.php?q=0#>
22 December 2020
20:47
Idiopathic intracranial
hypertension
Idiopathic intracranial
hypertension (also known as pseudotumour cerebri and formerly benign
intracranial hypertension) is a condition classically seen in young, overweight
females.
Risk factors
·
obesity
·
female sex
·
pregnancy
·
drugs*: oral contraceptive pill, steroids, tetracycline, vitamin A, lithium
Features
·
headache
·
blurred vision
·
papilloedema (usually present)
·
enlarged blind spot
·
sixth nerve palsy may be present
Management
·
weight loss
·
diuretics e.g. acetazolamide
·
topiramate is also used, and has the added benefit of causing
weight loss in most patients
·
repeated lumbar puncture
·
surgery: optic nerve sheath decompression and fenestration may
be needed to prevent damage to the optic nerve. A lumboperitoneal or
ventriculoperitoneal shunt may also be performed to reduce intracranial
pressure
*if intracranial hypertension is
thought to occur secondary to a known causes (e.g. Medication) then it is of
course not idiopathic
Next question
Save my notes
Search
Go
Google
search on "Idiopathic intracranial hypertension"
Links
|
statMed.org |
00 |
|
|
|
Patient.info |
21 |
|
|
Suggest linkReport broken link
From <https://www.passmedicine.com/question/questions.php?q=0#>
Comparing neurology
diseases
01 January 2021
18:29
progressive
polyneuropathy and hyporeflexia 3 weeks following a gastrointestinal infection
- this is very suggestive of Guillain-Barre syndrome.
Myasthenia
gravis typically presents with muscle fatigue particularly after exercise and
ocular manifestations - droop of the upper eyelids is typical with weakness of
external ocular muscles producing diplopia. In contrast to Guillain-Barre syndrome,
tone is normal, sensation is unimpaired and tendon reflexes are normal in
myasthenia gravis.
In
polymyositis, diffuse weakness in the proximal muscles develops. Distal muscles
are spared and weakness may vary from week to week or month to month. This is
in contrast to Stephen's progressive distal limb weakness.
Acute
transverse myelitis presents with an acute episode of weakness or paralysis of
both legs, with sensory loss and loss of control of bowels and bladder.
Commonly there is associated back or leg pain. This is a differential to
consider here, however no bladder or bowel dysfunction is mentioned and there
is also no mention of back pain in Stephen's history. Furthermore the history
of gastrointestinal infection 3 weeks ago points more towards a diagnosis of
Guillain-Barre syndrome.
Posterior
circulation ischaemic stroke may present with motor or sensory deficits,
however symptoms can often also include dizziness, diplopia, dysarthria,
dysphagia, disequilibrium, ataxia, or visual field deficits - Stephen does not
have any of these symptoms. Furthermore in a posterior circulation stroke, th
From <https://www.passmedicine.com/question/questions.php?q=0>
Hypotension with
compensatory tachycardia 4D's
01 January 2021
19:03
Of
all the other options, one would expect a compensatory tachycardia on standing.
The '4Ds' can be useful in remembering causes of postural hypotension with
compensatory tachycardia.
·
Deconditioning.
·
Dysfunctional heart:
aortic stenosis.
·
Dehydration: disease
(acute illness, adrenal insufficiency), dialysis, drugs (diuretics, narcotics).
·
Drugs: anti-anginals,
anti-parkinsonian medications (levodopa), antidepressants, antipsychotics,
anti–benign prostatic hyperplasia drugs (tamsulosin).
From <https://www.passmedicine.com/question/questions.php?q=0>
01 January 2021
20:51
Pontine haemorrhage
Is a life-threatening condition. It often occurs as a complication
secondary to chronic hypertension. Patients often present with reduces Glasgow
coma score, quadriplegia, miosis, and absent horizontal eye movements.
Hyperkinetic movement
05 January 2021
13:23
common types of
hyperkinetic movements:
|
Tremor |
An oscillatory, usually rhythmic (to-and-fro) movement of one or
more body parts, such as the neck, tongue, chin, or vocal cords or a limb.
The rate, location, amplitude, and constancy vary depending on the specific
type of tremor. |
|
Dystonia |
Both agonist and antagonist muscles of a body region contract simultaneously to produce a twisted posture of the limb, neck,
or trunk. In contrast to chorea, dystonic movements repeatedly involve
the same group of muscles. They do not necessarily flow or affect
different muscle groups randomly. |
|
Myoclonus |
Sudden, brief, shock like jerks are caused by muscular contraction
(positive myoclonus) or inhibition (negative myoclonus, such as asterixis). |
|
Chorea |
Involuntary, irregular, purposeless, nonrhythmic,
often abrupt, rapid, and unsustained movements seem to flow randomly from one
body part to another; they are unpredictable in timing, direction, and
distribution. |
|
Tics |
Abnormal, stereotypic, repetitive movements (motor tics) or
abnormal sounds (phonic tics) can be suppressed temporarily but may need to
be “released” at some point. The release provides internal “relief” to the
patient until the next “urge” is felt. |
From <https://mle.ncl.ac.uk/cases/page/17516/>
Action
tremors can occur on different types of movement
·
Postural
- occurs when limbs/body specifically postured
against gravity (see video at 0:40)
·
Kinetic
- occurs on goal-directed movement e.g. lifting
a glass to lips
The
most common action tremor is essential tremor, sometimes called benign
essential tremor. This is a slowly progressive neurological disease that can
significantly impact a patient's quality of life. It is often inherited in an
autosomal dominant pattern. Patients will often report that their tremor
improves with alcohol.
Treatment
approach includes
Conservative:
relaxation techniques, reduce caffeine
Medical:
propanolol, primidone
Surgical:
deep brain stimulation (only for very severe/refractory cases)
From <https://mle.ncl.ac.uk/cases/page/17513/>
Physiological
tremor
It is
normal to sometimes experience a physiological tremor, often an action/postural
tremor. Physiological tremor can be exacerbated by stress, anxiety and
fatigue. You have probably noticed this in yourself when nervous or after
intense exercise. This can also be exacerbated by beta agonists e.g. salbutamol.
It is
worth mentioning that tremors with a lower amplitude (amount of movement), tend
to have a high frequency (movements per second). A normal physiological
tremor demonstrates a high frequency (10Hz) but a low amplitude.
Functional
tremor
Functional
tremor is a tremor that is caused by the nervous system not working properly
but not due to an underlying neurological disease ( https://www.neurosymptoms.org/functional-tremor/4594357998).
Tremors that have a high amplitude AND frequency are more likely to be
functional in nature. Features that point towards a functional tremor diagnosis
are: abrupt onset, incongruous examination findings, variable, and changes or
reduces frequency/amplitude on distraction. These tremors may have a variable
frequency and can sometimes be 'entrained' (tremor frequency switches to match
exactly the frequency of a voluntary rhythmical movement performed by the
unaffected limb.) Functional tremors can be extremely disabling for patients.
Intention
tremor
Intention
tremors are tremors that are worsened during the endpoint of a directed
movement towards a target. It has low frequency and a high amplitude. We see
this when the cerebellar system is affected because the patient cannot
precisely co-ordinate their movement to the target. Notice how the below tremor
increases as the person tries to touch their nose.
From <https://mle.ncl.ac.uk/cases/page/17513/>
|
Type of tremor |
Description |
Examples |
|
Resting tremor |
Occurs when the affected extremity is at
complete rest and diminishes with movement |
Parkinson’s disease |
|
Postural tremor |
Occurs when the affected limb is held in
position against gravity. |
Essential tremor Medication induced tremor Physiological tremor |
|
Kinetic tremor |
Occurs during voluntary movement. |
Essential tremor |
|
Intention tremor |
Marked increase in tremor amplitude during
the terminal portion of a targeted movement |
Cerebellar tremor |
From <https://mle.ncl.ac.uk/cases/page/17513/>
Dystonias:
Dystonia
is caused by sustained or intermittent muscle contractions / spasms that often
lead the patient to hold abnormal postures or positions. This frequently causes
discomfort and pain for the patient. Dystonia can have a genetic cause or
be acquired from mechanisms such as trauma, stroke and drug toxicity. We will
look at drug induced hyperkinesia later in this tutorial.
·
Focal: one body part affected
·
Segmental: adjacent body parts affected
·
General: entire body affected
From <https://mle.ncl.ac.uk/cases/page/17517/>

Approach
to management:
·
Conservative: education, relaxation, massage
·
Medical: A small % of patients respond to dopaminergic
medication (e.g. levodopa). Benzodiazepines are also used.
·
Surgical: BoTox injection, especially useful in focal
dystonia. Deep brain stimulation may be used in severe cases.
Myoclonus:
You
will have experienced myoclonus in the form of hypnic jerks when you have been
falling asleep. These are the jolty / jerking limb movements that occur at the
point of sleep onset. This is a normal nocturnal motor phenomenon but is a form
of myoclonus. You can watch the video below to see an example of pathological
myoclonus.
When myoclonus is pathological it
is more often a feature of an underlying disease than a primary disorder. The
characteristics of the myoclonus can help to localise the area of pathology but
this is not something you need to know as a medical student.
Chorea:
Chorea is dervied from the
Ancient Greek word for dance and describes an involuntary movement that is
brief, irregular, nonrhythmic, non
purposeful and flows from one body part to another in a random fashion. The
movements typically last longer than myoclonus and are briefer than dystonia
(although dystonia may be combined with chorea in some patients).
It is usually present at rest and
may increase with distracting manoeuvres such as counting or performing mental arithmetic. The
movements may be partially suppressible or incorporated into voluntary movements
to make them less conspicuous. They usually disappear in sleep. Chorea can be
unilateral or bilateral. It can affect all body parts: face, trunk, and limbs.
There are various causes of
chorea that include drug-induced, stroke related and genetic causes. We will
focus on Huntington's disease as a cause of chorea in the next chapter.
Tics:
You will likely be familiar with
tics as a result of Tourette's syndrome (TS). A tic is an involuntary movement
or vocalization that is usually of sudden onset, brief, repetitive, and
stereotyped, but nonrhythmic. They are
different to other hyperkinetic movements in that they are suppressible but
irresistible.
A tic is usually associated with
a premonitory “buildup” sensation or feeling of discomfort that is often
localized to the affected area. Usually, the individual experiences a sensation
of relief once the tic has occurred. Unlike most movement disorders, tics can persist
during sleep.
They can be classified as motor,
phonic or vocal and as simple or complex based on the manifestation. TS is
thought to involve abnormalities in corticostriatothalamocortical circuitry.
The video below shows some patient experiences with TS.
Huntington's disease
05 January 2021
13:38

Huntington's
disease (HD) is the most frequent cause of a
hereditary neurodegenerative choreic syndrome. It is caused
by a faulty gene on chromosome 4, producing a
mutant form of a protein called Huntingtin,
which is thought to increase the rate of
neuronal death in the brain. It is relatively rare disorder and
affects about 8,000 people in the UK. HD is an autosomal disorder and therefore
each child of an affected parent has a 50% chance of developing the
disease (ref). We
will take a deeper look into the genetics after we have learnt a bit more about
the disease.
It is
important that you recognise that HD is not only a movement disorder but also
has marked cognitive and behavioural effects. In fact, the earliest signs of
the disease in a patient are often subtle cognitive or mood related changes.
Read the diagram below from https://hopes.stanford.edu/stages-of-huntingtons-disease/#46539 to
appreciate the complex nature of the disease. Patients symptoms are highly
variable and will present unique difficulties dependent on their particular
lifestyle.
Motor symptoms include chorea,
dystonia, and tics. Characteristically,
the first motor symptom exhibited is a chorea (hence HD is also known as
Hungtinton's chorea). The examination in the video below is very useful, in
terms of being able to see specific signs but also in helping you to develop a
general neurological impression of a patient
with established HD.
We learned earlier
that Hungtinton's disease has an autosomal dominant inheritance. The
huntingtin gene (on the short arm of chromosome 4) codes for the huntingtin
protein. The specific pathology of the disease is not completely
characterised but mutated huntingtin protein aggregates are found in the basal
ganglia, specifically the dorsal striatum (caudate and putamen), and these
areas show increased neuronal death rates. There is thought to be a toxic
gain-of-function in the mutant huntingtin protein.

A section of the
genetic code for this protein has something called a trinucleotide repeat
expansion. This is a repeating sequence of three nucleotides. In the case of
huntingtin, this is a CAG repeat (which encodes glutamine and hence is known as
a polyglutamine disease).

Patients with 40 or
more repeats will develop the disease (100% penetrance) but patients with 36-39
repeats show a reduced penetrance. 27-35 repeats are classified as in the
'intermediate CAG range' and less than this is normal. For example, if a patient has a repeat number of 40, they are certain to
develop the disease (assuming they survive until disease onset). A patient with
36 repeats may or may not develop HD and a patient with fewer repeats
than this will not.
|
Number
of CAG repeats |
Classification |
|
<27 |
Normal |
|
27-35 |
Intermediate
CAG range |
|
36-39 |
Reduced
penetrance |
|
>39 |
100%
penetrance |
The intermediate CAG
range refers to people who, despite not having the disease, are at risk of
passing on mutant alleles due to repeat expansion. This number of trinucleotide
repeats causes the sequence to be unstable during DNA replication. There is a
small risk that within one generation an error in replication can expand the
repeat number into the disease range. This occurs much more in sperm than ova generation and thus repeat
expansion mainly occurs in paternal alleles (ref). Further to this, expansion of repeats already
in the disease range leads to an earlier onset and faster progression of
symptoms. This phenomenon is known as anticipation. Each successive affected
generation has a chance of inheriting a greater number of repeats, again most
commonly from the father, and having an earlier disease onset.
Usually symptomatic onset is between the ages of 30 and 50, although
onset can range from childhood/adolescence to individuals older than 70
years of age. There is a juvenile form, also known as the Westphal
variant HD, due to a very large repeat count.
Other trinucleotide
repeat disorders you may come across include Friedreich's ataxia, fragile
X syndrome and types of myotonic dystrophy
and spinocerebellar ataxia (of these, only spinocerebellar ataxia is a
polyglutamine repeat).
From <https://mle.ncl.ac.uk/cases/page/17512/>
No disease modifying therapies
are currently available for HD on the NHS. HCurrent treatments include:
Conservative: Symptomatic /
supportive therapy to alleviate the symptoms
Medicine: Anti-choreic medication
– atypical antipsychotics, tetrabenazine
Surgical: Deep brain stimulation
for pharmacological resistant chorea with significant disability
Ultimately, there is no cure for
HD at present and treatment revolves around supportive care (such as
modifications in the patient's house by occupational therapists, physiotherapy,
speech and language therapy and additional carers) and symptomatic relief.
Tetrabenazine is approved for the treatment of chorea in HD. Antipsychotics can
be used to treat psychiatric symptoms, as well as often also helping with
chorea
Early symptoms
Motor:
Begin in extremities of body,
people experience involuntary twitches in their fingers, toes and face.
Onlookers generally don't notice these motions, or assume that they are just nerveous
twitches.
People in the early years of HD
also experience a subtle loss of coordination, and may have more trouble
performing complicated motions
Cognitive symptoms:
Cognitive symptoms also become
noticeable in the early stages of HD, as it become more difficult for people to
think through complicated tasks
Behavioral:
Can be fairly serious even when
motor and cognitive symptoms are quite minor. Depression, irritability, and
inhibition are common in the early stages, some patients experience
hypersexuality, which can cause problems in relationships

Mid-stage HD


Drug induced movement
disorder
05 January 2021
13:54
Drug-induced movement disorders
can be caused by a wide variety of drugs, including illicit substances (e.g.
cocaine and amphetamines). We will focus on some important examples in this
tutorial.
Tardive dyskinesia
The most common cause of
drug-induced movement disorders are dopamine receptor blocking agents.
Antipsychotics, metoclopramide and prochlorperazine are prevalent examples that
you will undoubtedly prescribe during your career. These medications can cause
various movement disorders including tremor, neuroleptic malignant syndrome
(covered in the next section), dystonia and parkinsonism.
One of these disorders is called
tardive dyskinesia. Classically, there are involuntary movements of the mouth,
tongue and jaw (oro-buccal-lingual). There are various other 'tardive
syndromes' that can affect the trunk and extremities, including causing
choreiform movements. You can see a more
classic example in the video below.
The exact pathophysiology of
tardive dyskinesia in unclear. A common theory is that there is a dopamine
hypersensitivity in the nigrostriatal pathway after chronic pharmacological
blockage .
Tardive dyskinesia can be
diagnosed if:
Patient had at least 3 months
exposure to a dopamine receptor blocking agent (1 month if patient >60yrs
old).
Symptoms present for at least 1
month after medication discontinued
Symptoms can emerge during or up
to 4 weeks after stopping the medication - hence the name tardive (late/delayed
appearance). You do not need to memorise these criteria but they are useful to
appreciate the delayed onset of the disorder .
Treatment can be difficult and
therefore prevention is crucial. Dopamine receptor blocking medications should
be used in the lowest dose for the shortest time possible. Treatment involves
withdrawing the offending agent and this may require an analysis of benefit vs.
harm (e.g. if the antipsychotic is treating schizophrenia). There is usually a
delay before improvement and changes can be irreversible. Tetrabenazine can be
effective in some people who have not responded to treatment withdrawal.
neuroleptic malignant syndrome (NMS)
Dopamine
receptor blocking drugs can cause a severe neurological emergency called
neuroleptic malignant syndrome (NMS). This can also be induced by sudden
cessation of dopaminergic medications e.g. levodopa.
NMS is
a clinical diagnosis, supported by the diagnostic criteria below. NMS is
characterised by high
temperatures, rigidity, autonomic dysfunction and altered
mental status (often agitated confusion). Patients may demonstrate
hyporeflexia.
|
Major (need all 3) |
Minor (at least 2) |
|
Exposure
to dopamine antagonist or
withdrawal of dopaminergic |
Diaphoresis
(sweating) |
|
Rigidity |
Dysphagia |
|
Hyperthermia |
Tremor |
|
|
Incontinence |
|
|
Altered
levels of consciousness |
|
|
Mutism |
|
|
Tachycardia |
|
|
Elevated
or labile BP |
|
|
Leukocytosis |
|
|
Elevated
CK |
Adapted
from Diagnostic and Statistical Manual of Mental Disorders, 5th Edition
A
common scenario for this to occur would be with a patient already on an
antipsychotic e.g. haloperidol (highest risk) who is then given a dopamine
blocking antiemetic such as metoclopramide. The high temperature and altered
mental state would make you think about infection but is important to take note
of the patient's medications. Rigidity,
a new tremor and a raised CK should make you think
about NMS.
The
pathophysiology of NMS is thought to be due to the abrupt loss of dopaminergic
activity in the nigrostriatal pathway and basal ganglia, with fever thought to
be due to dopamine blockade in the hypothalamus (which plays a role in
thermoregulation).
Treatment
approach:
·
Stop the dopamine
blocking medication
·
Supportive care: IV
fluids, correct metabolic abnormalities
·
Medications in severe
cases: bromocriptine (a dopamine agonist, to increase dopaminergic activity)
and dantrolene (muscle relaxant to reduce rigidity, acts by inhibiting
inhibiting calcium release from the sarcoplasmic reticulum in muscle
cells.)
(ref)
From <https://mle.ncl.ac.uk/cases/page/17522/>
Serotonin syndrome:
Serotonin syndrome is
another drug-induced syndrome that causes hyperthermia and neurological
changes. In patients with polypharmacy you may need to differentiate this from
NMS.
Serotonin syndrome
can be caused by prescription of multiple serotonergic drugs or medication
overdose. This essentially leads to serotonin toxicity and hyperstimulation in
the central nervous system. The video below is a good primer for the topic.
Serotonin
syndrome can be caused by multiple classes of drugs that affect signaling in
presynaptic and postsynaptic serotonergic neurons (in the raphe nuclei of the
brainstem). The picture below demonstrates a serotonin synapse and how
medications affect this.
·
MAO inhibitors: reduced
breakdown of serotonin
·
Illicit drugs: promote serotonin release into the synaptic cleft or
directly stimulate the postsynaptic cleft (amphetamines, ecstasy and cocaine)
·
Tricyclic
antidepressants: reduce
serotonin re-uptake into the presynaptic neurone (amitriptyline)
·
SSRIs and
SNRIs: reduce serotonin re-uptake into the presynaptic
neurone (fluoxetine, sertraline, duloxetine)
·
Synthetic
opioids: multiple effects on serotonergic
neurons (tramadol,
fentanyl)
(ref)
The table below shows
the diagnostic criteria for serotonin syndrome. As is characterised by the
acute onset of symptoms, commonly after a serotonergic medication
change/overdose.

Approach to
treatment:
·
Withdraw serotonergic agents
·
Supportive care: IV fluids, cooling
·
Medications in severe cases:
Benzodiazepines can be used to reduce agitation and myoclonus. Cyproheptadine
(a serotonin antagonist) is sometimes used but the evidence base for this is
not strongly established.
We can see that a lot
of symptoms overlap with NMS. Differentiating between the two conditions
clearly begins with checking the patient's medications and any recent changes.
If a patient is pharmacologically at risk of both, their neurological symptoms
are most helpful in distinguishing between the two.
|
|
Serotonin
Syndrome |
Neuroleptic
Malignant Syndrome |
|
Timing |
More
acute (<24hours) |
More
gradual (days-weeks) |
|
Drugs |
Serotonergic |
Dopaminergic |
|
Neurological
reactivity |
Increased:
hyperreflexia, clonus, tremor |
Decreased:
rigidity, hyporeflexia |
|
GI
Features |
Diarrhoea,
increased bowel sounds |
Usually
normal |
From <https://mle.ncl.ac.uk/cases/page/17514/>
Future treatments
05 January 2021
14:02
Spinal Muscular
Atrophy:
Recent advances in
genetic medicine have allowed for the development of new treatments for single
gene disorders. This is in the form of a new class of drugs called anti-sense
oligonucleotides (ASOs). These compounds bind to specific mRNAs and ultimately
affect protein expression in various desired ways, dependent on the disease we
are treating.
For neurological
disorders this has led to the development of treatments for Spinal Muscular
Atrophy (SMA), and emerging treatments for Huntington's disease and MND (single
gene variants).
The SMN protein is
particularly important in promoting the survival of alpha motor neurons, which
exit through the ventral roots of the spinal cord to directly innervate
skeletal muscle and initiate contraction. In SMA the SMN1 gene
is mutated or deleted homozygously in a way that ultimately results in
insufficient levels of SMN protein.
The SMN2 gene
is a pseudogene copy of SMN1, which
means that it is a mutated copy which produces little or no functional protein.
In this case very little functional protein is produced. This is because a
single nucleotide mutation in exon 7 of SMN2 leads
to it being removed in the majority of mRNAs. This resultant protein is
non-functional / rapidly degraded.
Nusinersen is an ASO
which binds to a complimentary sequence after exon 7 and causes mRNA processing
to include this exon. Thus, functional SMN protein is produced. For many
patients this leads to significant motor function and survival
benefits.
From <https://mle.ncl.ac.uk/cases/page/17569/>
Huntington's disease
The pathology of
Huntington's disease has been covered in
the 'Hyperkinesia' tutorial. You will recall that this is an autosomal dominant
condition in which a mutant copy of the huntingtin gene has an expansion of the
CAG triplet repeats. This leads to the production of a toxic gain-of-function
mutant huntingtin protein.
Lowering mutant huntingtin
protein levels in the brain has been shown to improve symptoms of the disease.
ASOs have therefore been developed to reduce the levels of this protein. In
this case, rather than ASO binding resulting in increased levels of a protein,
the ASO binding to mutant mRNA targets this mRNA for degradation
Motor neurone disease
The pathology and types of MND
have been covered in the 'Motor Neurone Disease' lecture from this week's
content. Amyotrophic lateral sclerosis (ALS) can be classified as either
sporadic or familial / inherited (5-10%) . The familial forms of ALS (FALS)
have a mutation in one of several genes known to cause ALS. These genes are
therefore being researched as targets for ASOs.
So far, the most promising
research has been undertaken with ASOs in patients with mutant SOD1 genes.
Multiple point mutations in this gene have been found to be associated with
FALS. However, the mechanism by which these mutations cause ALS is poorly
characterised. Despite this results have been promising.
At the time of writing there are
ongoing clinical trials for SOD1 ASOs. As with Huntington's, the purpose of the
ASO is to target mutant mRNA for degradation.
The SOD1 gene
is located on chromosome 21. If mutations in the SOD1 gene
cause a gain-of-function,
if
there is a gain of function from an allele, it is more likely that only one
copy of the gene will be required to cause the disease. Conversely, if there is
a loss-of-function in an allele, it is often the case that with wild type
(normal) allele will produce enough protein to compensate for this. Thus there
is a recessive pattern of inheritance. Again, this is not a hard and fast rule
and dominant loss-of-function mutations can also occur.
From <https://mle.ncl.ac.uk/cases/page/17569/>
05 January 2021
15:08
Progressive
Multifocal Leukoencephalopathy (PML)
This is
a rare condition, you don't need to know everything about it.
Just be
aware that PML is the big risk that neurologists think about when using DMTs,
especially Natalizumab. The strongest DMTs carry the greatest risk.
PML is
caused by reactivation of the JC virus in the CNS. Much of the general
population has already been exposed to the JC virus and carries it in an
inactive form. When the immune system is suppressed by DMTs, this virus can
reactivate in the brain and cause significant neurological problems and even
death. MS patients will have blood tests to assess the amount of JC virus
antibody in their blood. This can guide treatment decisions.
From <https://mle.ncl.ac.uk/cases/page/17721/>
Differentials diffuse
neuropathies
05 January 2021
15:34
·
Motor
neurone disease - A
mix of UMN and LMN signs. Motor only with absence of sensory
involvement. Fasiculation is more
prominent in MND.
·
Myasthenia
gravis - Neuromuscular junction
pathology. Muscle weakness that is fatiguable and varies over the day. Motor only with absence of sensory
involvement. Weakness is more proximal. Reflexes are normal. MG may manifest with
bulbar involvement, unlike peripheral neuropathy.
·
Spinal
cord syndrome - A spinal cord lesion
will cause UMN signs. Weakness/sensory loss below the level of
the lesion.
·
Cauda
Equina syndrome - Cauda
Equina syndrome can look like a peripheral neuropathy. Bladder and bowel
disturbance can also be present in autonomic neuropathy. Look for Cauda Equina red flag signs e.g. urinary retention, saddle anaesthesia,
loss of anal tone etc. Back pain may be present. Have a low threshold for MRI
spine if you suspect Cauda Equina syndrome.
·
Myopathies
- Motor only with no sensory
involvement. Weakness
is more proximal than distal (where larger muscle groups are.)
Reflexes are normal. Fasiculation is unlikely.
From <https://mle.ncl.ac.uk/cases/page/17594/>
Acute multi-focal
neuropathy
05 January 2021
15:36
Acute
multi-focal neuropathy
An
acute multi-focal neuropathy picture of random nerves being "picked
off" suddenly is an alarming condition for a neurologist. A hyper-acute
rapid onset suggests a vascular cause, fast action and urgent neurology
referral is required to save the nerve from irreversible damage. A vasculitic
neuropathy is rare, but worth being aware of due to the devastating
consequences of delayed treatment.
From <https://mle.ncl.ac.uk/cases/page/17650/>
05 January 2021
15:37
Chronic
inflammatory demyelinating polyneuropathy (CIDP):
A
demyelinating process, causing predominantly painless motor symptoms. Can be
seen on EMG studies. Treated with immune-modifying therapies e.g.
steroids/IVIG/plasma exchange. May have future relapses and require further
treatment.
From <https://mle.ncl.ac.uk/cases/page/17651/>
Sub-acute (weeks) are rare causes
of a diffuse peripheral neuropathy and will be mostly invested/managed by a
neurologist. Be aware of the basic principles.
05 January 2021
15:37
Paraneoplastic:
Cancer
can cause a paraneoplastic immune-mediated peripheral neuropathy, especially
small cell lung cancer and lymphoma. If suspected, investigations to look for
an underlying cancer (e.g. CT chest/abdo/pelvis) may be indicated. Remember,
some chemotherapy regimes may also cause a peripheral neuropathy.
Sub-acute (weeks) are rare causes
of a diffuse peripheral neuropathy and will be mostly invested/managed by a
neurologist. Be aware of the basic principles.
24 December 2020
12:23
Pulmonary embolism: investigation
We know from experience that few
patients (around 10%) present with the textbook triad of pleuritic chest pain,
dyspnoea and haemoptysis. Pulmonary embolism can be difficult to diagnose as it
can present with virtually any cardiorespiratory symptom/sign depending on its
location and size.
So which features make pulmonary
embolism more likely?
The PIOPED study1 in 2007
looked at the frequency of different symptoms and signs in patients who were
diagnosed with pulmonary embolism.
The relative frequency of common
clinical signs is shown below:
·
Tachypnea (respiratory rate >20/min) - 96%
·
Crackles - 58%
·
Tachycardia (heart rate >100/min) - 44%
·
Fever (temperature >37.8°C) - 43%
It is interesting to note that the
Well's criteria for diagnosing a PE use tachycardia rather than tachypnoea.
All patients with symptoms or signs
suggestive of a PE should have a history taken, examination performed and a
chest x-ray to exclude other pathology.
Pulmonary embolism rule-out
criteria (PERC)
NICE updated their guidelines on
the investigation and management of venous thromboembolism (VTE) in 2020. One
of the key changes was the use of the pulmonary embolism rule-out criteria (the PERC rule)
·
a copy of criteria can be found in the image below
·
all the criteria must be absent to have negative PERC result, i.e.
rule-out PE
·
this should be done when you think there is a low pre-test probability of PE, but want more reassurance that it isn't the diagnosis
o this low probability is defined as < 15%, although it is clearly difficult to quantify such judgements
·
a negative PERC reduces the probability of PE to < 2%
·
if your suspicion of PE is greater than this then you should
move straight to the 2-level PE Wells score, without doing a PERC
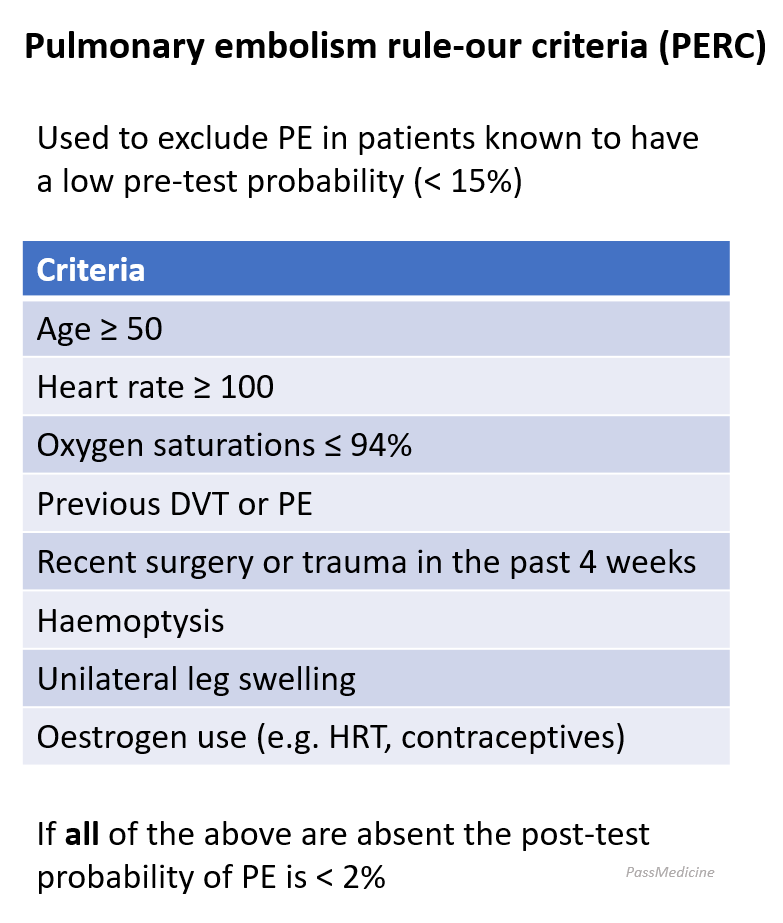
2-level PE Wells score
If a PE is suspected a 2-level PE Wells score should be performed:
|
Clinical
feature |
Points |
|
Clinical signs and symptoms of DVT
(minimum of leg swelling and pain with palpation of the deep veins) |
3 |
|
An alternative diagnosis is less likely
than PE |
3 |
|
Heart rate > 100 beats per minute |
1.5 |
|
Immobilisation for more than 3 days or
surgery in the previous 4 weeks |
1.5 |
|
Previous DVT/PE |
1.5 |
|
Haemoptysis |
1 |
|
Malignancy (on treatment, treated in
the last 6 months, or palliative) |
1 |
Clinical probability simplified
scores
·
PE likely - more than 4 points
·
PE unlikely - 4 points or less
If a PE is 'likely' (more than 4
points)
·
arrange an immediate computed tomography
pulmonary angiogram (CTPA)
·
If there is a delay in getting the CTPA then
interim therapeutic anticoagulation should be given until the scan is performed.
o interim therapeutic anticoagulation
used to mean giving low-molecular-weight heparin
o NICE updated their guidance in
2020. They now recommend using an anticoagulant that can be continued if the
result is positive.
o this means normally a direct oral
anticoagulant (DOAC) such as apixaban or rivaroxaban
- if the CTPA is positive then a PE
is diagnosed
·
if the CTPA is negative then consider a proximal
leg vein ultrasound scan if DVT is suspected
If a PE is 'unlikely' (4 points or
less)
·
arranged a D-dimer test
o if positive arrange an immediate
computed tomography pulmonary angiogram (CTPA). If there is a delay in getting
the CTPA then give interim therapeutic anticoagulation until the scan is performed
o if negative then PE is unlikely - stop anticoagulation and consider an alternative diagnosis
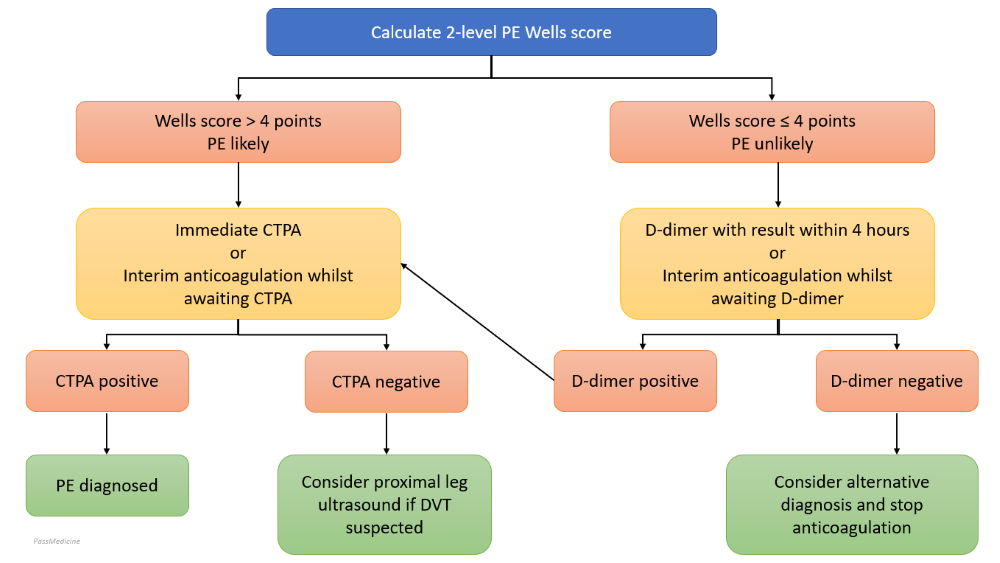

CTPA or V/Q scan?
The consensus view from the British
Thoracic Society and NICE guidelines is as follows:
·
CTPA is now the recommended initial lung-imaging modality for
non-massive PE. Advantages compared to V/Q scans include speed, easier to
perform out-of-hours, a reduced need for further imaging and the possibility of
providing an alternative diagnosis if PE is excluded
·
if the CTPA is negative then patients do not need further
investigations or treatment for PE
·
V/Q scanning may be used initially if appropriate facilities exist,
the chest x-ray is normal, and there is no significant symptomatic concurrent
cardiopulmonary disease. V/Q scanning is also the investigation of choice if
there is renal impairment (doesn't require the use of
contrast unlike CTPA)
Some other points
D-dimers
·
sensitivity = 95-98%, but poor specificity
·
age-adjusted D-dimer levels should be considered for patients
> 50 years
ECG
·
the classic ECG changes seen in PE are a large S wave in lead I,
a large Q wave in lead III and an inverted T wave in lead III - 'S1Q3T3'. However, this
change is seen in no more than 20% of patients
·
right bundle branch block and right axis deviation are also
associated with PE
·
sinus tachycardia may also be seen
Chest x-ray
·
a chest x-ray is recommended for all patients to exclude other pathology
·
however, it is typically normal in PE
·
possible findings include a wedge-shaped
opacification
V/Q scan
·
sensitivity of around 75% and specificity of 97%
·
other causes of mismatch in V/Q include old pulmonary embolisms,
AV malformations, vasculitis, previous radiotherapy
·
COPD gives matched defects
CTPA
·
peripheral emboli affecting subsegmental arteries may be missed
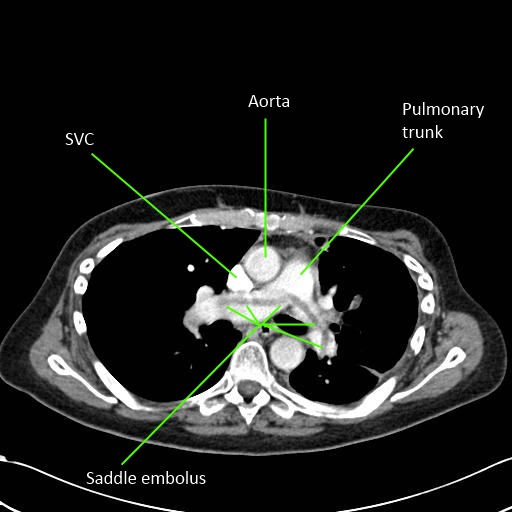

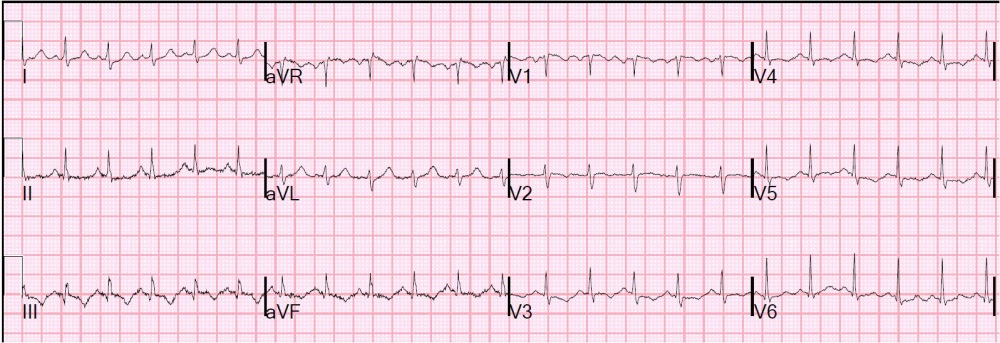
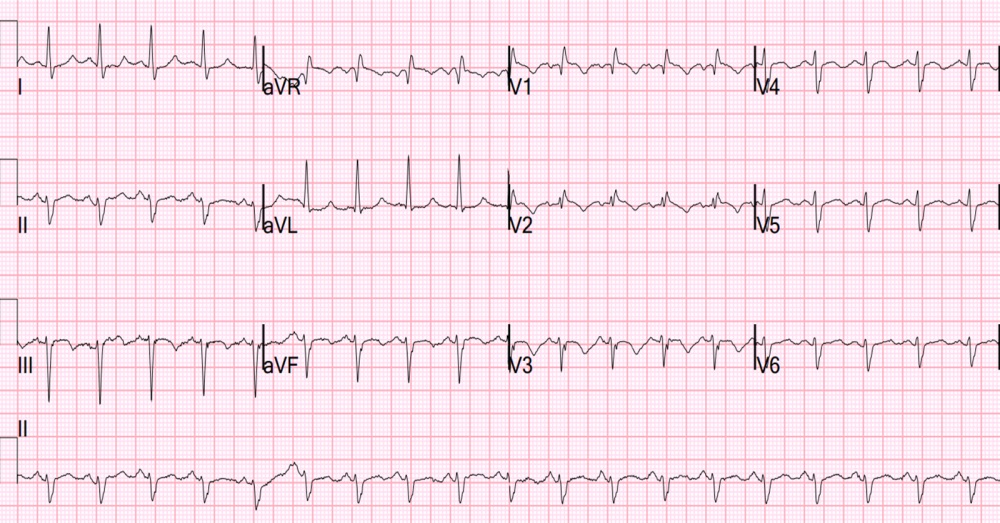
1. Clinical Characteristics of
Patients with Acute Pulmonary Embolism(Data from PIOPED II) Am J Med. Oct 2007;
120(10): 871879.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:23
Angina pectoris: drug management
The management of stable angina
comprises lifestyle changes, medication, percutaneous coronary intervention and
surgery. NICE produced guidelines in 2011 covering the management of stable
angina
Medication
·
all patients should receive aspirin and a statin in the absence
of any contraindication
·
sublingual glyceryl trinitrate to abort angina attacks
·
NICE recommend using either a beta-blocker or a calcium channel blocker first-line based
on 'comorbidities, contraindications and the person's preference'
·
if a calcium channel blocker is used as monotherapy a
rate-limiting one such as verapamil or diltiazem should be used. If used in
combination with a beta-blocker then use a long-acting dihydropyridine calcium-channel
blocker (e.g. modified-release nifedipine). Remember that beta-blockers should
not be prescribed concurrently with verapamil (risk of complete heart block)
·
if there is a poor response to initial treatment then medication
should be increased to the maximum tolerated
dose (e.g. for
atenolol 100mg od)
·
if a patient is still symptomatic after monotherapy with a
beta-blocker add a calcium channel blocker and vice versa
·
if a patient is on monotherapy and cannot tolerate the addition
of a calcium channel blocker or a beta-blocker then consider one of the
following drugs: a long-acting nitrate, ivabradine, nicorandil or ranolazine
·
if a patient is taking both a beta-blocker and a calcium-channel
blocker then only add a third drug whilst a patient is awaiting assessment for
PCI or CABG
Nitrate tolerance
·
many patients who take nitrates develop tolerance and experience
reduced efficacy
·
NICE advises that patients who take standard-release isosorbide
mononitrate should use an asymmetric dosing interval to maintain a daily nitrate-free
time of 10-14 hours to minimise the development of nitrate tolerance
·
this effect is not seen in patients who take once-daily
modified-release isosorbide mononitrate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:48
Acute pericarditis
Pericarditis is one of the
differentials of any patient presenting with chest pain.
Features
·
chest pain: may be pleuritic. Is
often relieved by sitting forwards
·
other symptoms include non-productive cough, dyspnoea and
flu-like symptoms
·
pericardial rub
·
tachypnoea
·
tachycardia
Causes
·
viral infections (Coxsackie)
·
tuberculosis
·
uraemia (causes 'fibrinous' pericarditis)
·
trauma
·
post-myocardial infarction, Dressler's syndrome
·
connective tissue disease
·
hypothyroidism
·
malignancy
Investigations
·
ECG changes
o the changes in pericarditis are
often global/widespread, as opposed to the 'territories'
seen in ischaemic events
o 'saddle-shaped' ST elevation
o PR depression: most specific ECG
marker for pericarditis
·
all patients with suspected acute pericarditis should have
transthoracic echocardiography
Management
·
treat the underlying cause
·
a combination of NSAIDs and colchicine is now generally used for
first-line for patients with acute idiopathic or viral pericarditis
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|

ECG showing pericarditis. Note the widespread nature of
the ST elevation and the PR depression
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:49
Long QT syndrome
Long QT syndrome (LQTS) is an
inherited condition associated with delayed repolarization of the ventricles.
It is important to recognise as it may lead to ventricular tachycardia/torsade de pointes and can therefore cause collapse/sudden death. The most common
variants of LQTS (LQT1 & LQT2) are caused by defects in the alpha subunit
of the slow delayed rectifier potassium
channel. A normal corrected QT interval is less than 430 ms in
males and 450 ms in females.
Causes of a prolonged QT interval:
|
Congenital |
Drugs* |
Other |
|
·
Jervell-Lange-Nielsen syndrome (includes deafness and is due to an
abnormal potassium channel) ·
Romano-Ward syndrome (no
deafness) |
·
amiodarone, sotalol, class 1a
antiarrhythmic drugs ·
tricyclic antidepressants, selective serotonin
reuptake inhibitors (especially citalopram) ·
methadone ·
chloroquine ·
terfenadine** ·
erythromycin ·
haloperidol ·
ondanestron |
·
electrolyte: hypocalcaemia, hypokalaemia, hypomagnesaemia ·
acute myocardial infarction ·
myocarditis ·
hypothermia ·
subarachnoid haemorrhage |
Features
·
may be picked up on routine ECG or following family screening
·
Long QT1 - usually associated with exertional syncope, often
swimming
·
Long QT2 - often associated with syncope occurring following
emotional stress, exercise or auditory stimuli
·
Long QT3 - events often occur at night or at rest
·
sudden cardiac death
Management
·
avoid drugs which prolong the QT interval and other precipitants
if appropriate (e.g. Strenuous exercise)
·
beta-blockers***
·
implantable cardioverter defibrillators in high risk cases
*the usual mechanism by which drugs
prolong the QT interval is blockage
of potassium channels. See the link for more details
**a non-sedating antihistamine and
classic cause of prolonged QT in a patient, especially if also taking P450
enzyme inhibitor, e.g. Patient with a cold takes terfenadine and erythromycin
at the same time
***note sotalol may exacerbate long
QT syndrome
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:50
Pulmonary embolism: management
NICE updated their guidelines on
the management of venous thromboembolism (VTE) in 2020. Some of the key changes
include recommending the following:
·
the use of direct oral anticoagulants (DOACs) as first-line
treatment for most people with VTE
·
the use of DOACs in patients with active cancer, as opposed to
low-molecular weight heparin as was the previous recommendation
·
outpatient treatment in low-risk pulmonary embolism (PE)
patients
·
routine cancer screening is no longer recommended following a
VTE diagnosis
Outpatient treatment in low-risk PE
patients
Deep vein thrombosis has for a long
time been treated on an outpatient condition. In contrast, patients with any
form of PE were typically admitted. However, in recent years patients with a
new diagnosis of PE who are deemed low-risk are now increasingly managed as
outpatients. NICE formally supported this approach in their latest guidance.
·
NICE recommends using a 'validated risk stratification tool' to
determine the suitability of outpatient treatment.
o no guidance is given as to what
tool should be used
o the 2018 British Society guidelines
support the use of the Pulmonary Embolism Severity Index
(PESI) score
·
key requirements would clearly be haemodynamic stability, lack
of comorbidities and support at home
Anticogulant therapy
The cornerstone of VTE management
is anticoagulant therapy. This was historically done with warfarin, often
preceded by heparin until the INR was stable. However, the development of
DOACs, and an evidence base supporting their efficacy, has changed modern management.
Choice of anticoagulant
·
the big change in the 2020 guidelines was the increased use of
DOACs
·
apixaban or rivaroxaban (both DOACs) should be offered
first-line following the diagnosis of a PE
o instead of using low-molecular
weight heparin (LMWH) until the diagnosis is confirmed, NICE now advocate using
a DOAC once a diagnosis is suspected, with this continued if the diagnosis is confirmed
o if neither apixaban or rivaroxaban
are suitable then either LMWH followed by dabigatran or edoxaban OR LMWH followed
by a vitamin K antagonist (VKA, i.e. warfarin)
·
if the patient has active cancer
o previously LMWH was recommended
o the new guidelines now recommend
using a DOAC, unless this is contraindicated
·
if renal impairment is severe (e.g. < 15/min) then LMWH, unfractionated
heparin or LMWH followed by a VKA
·
if the patient has antiphospholipid syndrome (specifically
'triple positive' in the guidance) then LMWH followed by a VKA should be used
Length of anticoagulation
·
all patients should have anticoagulation for at least 3 months
·
continuing anticoagulation after this period is partly
determined by whether the VTE was provoked or unprovoked
o a provoked VTE is due to an obvious
precipitating event e.g. immobilisation following major surgery. The
implication is that this event was transient and the patient is no longer at
increased risk
o an unprovoked VTE occurs in the
absence of an obvious precipitating event, i.e. there is a possibility that
there are unknown factors (e.g. mild thrombophilia) making the patient more at
risk from further clots
·
if the VTE was provoked the treatment is
typically stopped after the initial 3 months (3 to 6 months for people with active
cancer)
·
if the VTE was unprovoked then treatment is typically continued
for up to 3 further months (i.e. 6 months in total)
o NICE recommend that whether a
patient has a total of 3-6 months anticoagulant is based upon balancing a
person's risk of VTE recurrence and their risk of bleeding
o the HAS-BLED score can be used to
help assess the risk of bleeding
o NICE state: 'Explain to people with unprovoked DVT or PE and a low bleeding risk that
the benefits of continuing anticoagulation treatment are likely to outweigh the
risks. '. The implication of this is that in the absence of a bleeding
risk factors, patients are generally better off continuing anticoagulation for
a total of 6 months
PE with haemodynamic instability
Thrombolysis
·
thrombolysis is now recommended as the first-line treatment for
massive PE where there is circulatory failure (e.g. hypotension)
·
other invasive approaches should be considered where appropriate
facilities exist
Patients who have repeat pulmonary
embolisms, despite adequate anticoagulation, may be considered for inferior vena cava (IVC) filters. These work by stopping clots formed in the deep veins of the
leg from moving to the pulmonary arteries. IVC filter use is currently
supported by NICE but other studies suggest a weak evidence base - please see
the link for more details.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:50
Aortic stenosis
Clinical features of
symptomatic disease
·
chest pain
·
dyspnoea
·
syncope
·
murmur
o an ejection
systolic murmur (ESM) is classically seen in aortic stenosis
o classically radiates to the
carotids
o this is decreased following the Valsalva manoeuvre
Features of severe aortic stenosis
·
narrow pulse pressure
·
slow rising pulse
·
delayed ESM
·
soft/absent S2
·
S4
·
thrill
·
duration of murmur
·
left ventricular hypertrophy or failure
Causes of aortic stenosis
·
degenerative calcification (most common cause in older patients
> 65 years)
·
bicuspid aortic valve (most common cause in younger patients
< 65 years)
·
William's syndrome (supravalvular aortic stenosis)
·
post-rheumatic disease
·
subvalvular: HOCM
Management
·
if asymptomatic then observe the patient is general rule
·
if symptomatic then valve replacement
·
if asymptomatic but valvular gradient > 40 mmHg and with features such as left
ventricular systolic dysfunction then consider surgery
·
cardiovascular disease may coexist. For this reason an angiogram is often done prior to surgery so that the procedures can be
combined
·
balloon valvuloplasty is limited to patients with critical
aortic stenosis who are not fit for valve replacement
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:50
ECG: myocardial ischaemia
One of the main uses of the ECG is
to determine whether a patient is having a cardiac event in the context of
chest pain. A wide variety of changes can be seen depending on what type of
ischaemic event is happening, where it is happening and when it happened.
Acute myocardial infarction (MI)
·
hyperacute T waves are often the first sign of MI but often only
persists for a few minutes
·
ST elevation may then develop
·
the T waves typically become inverted within the first 24 hours.
The inversion of the T waves can last for days to months
·
pathological Q waves develop after several hours to days. This
change usually persists indefinitely
Definition of ST elevation
myocardial infarction (STEMI)
·
clinical symptoms consistent with ACS (generally of ≥ 20 minutes
duration) with persistent (> 20 minutes) ECG features in ≥ 2 contiguous
leads of:
o 2.5 mm (i.e ≥ 2.5 small squares) ST
elevation in leads V2-3 in men under 40 years, or ≥ 2.0 mm (i.e ≥ 2 small
squares) ST elevation in leads V2-3 in men over 40 years
o 1.5 mm ST elevation in V2-3 in
women
o 1 mm ST elevation in other leads
o new LBBB (LBBB should be considered
new unless there is evidence otherwise)
A posterior MI causes
ST depression not elevation on a 12-lead ECG.
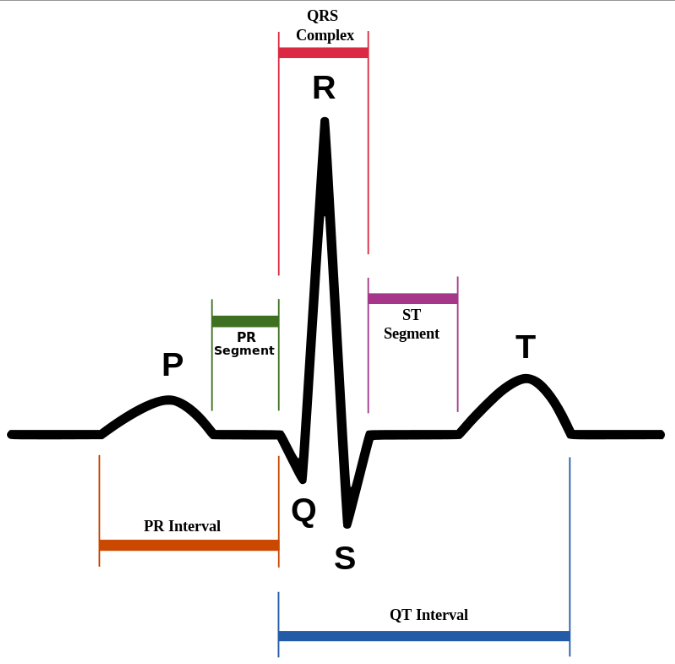
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:51
Warfarin
Warfarin is an oral anticoagulant
which inhibits
epoxide reductase preventing the reduction of vitamin
K to its active hydroquinone form, which in turn acts as a cofactor in the
carboxylation of clotting factor
II, VII, IX and X (mnemonic = 1972) and protein C.
Indications
·
venous thromboembolism: target INR = 2.5, if recurrent 3.5
·
atrial fibrillation, target INR = 2.5
·
mechanical heart valves, target INR depends on the valve type
and location. Mitral valves generally require a higher INR than aortic valves.
Patients on warfarin are monitored
using the INR (international normalised ration), the ratio of the prothrombin time for the
patient over the normal prothrombin time. Warfarin has a long half-life and
achieving a stable INR may take several days. There a variety of loading regimes
and computer software is now often used to alter the dose.
Factors that may potentiate
warfarin
·
liver disease
·
P450 enzyme inhibitors, e.g.: amiodarone, ciprofloxacin
·
cranberry juice
·
drugs which displace warfarin from plasma albumin, e.g. NSAIDs
·
inhibit platelet function: NSAIDs
Side-effects
·
haemorrhage
·
teratogenic, although can be used in
breastfeeding mothers
·
skin necrosis: when warfarin is first started biosynthesis of
protein C is reduced. This results in a temporary procoagulant state after
initially starting warfarin, normally avoided by concurrent heparin
administration. Thrombosis may occur in venules leading to skin necrosis
·
purple toes
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:51
Hypercalcaemia: features
Features
·
'bones, stones, groans and psychic moans'
·
corneal calcification
·
shortened QT interval on ECG
·
hypertension
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:51
Thiazide diuretics
Thiazide diuretics work by inhibiting sodium
reabsorption at the beginning of the distal convoluted tubule (DCT) by blocking
the thiazide-sensitive Na+-Cl− symporter. Potassium is lost as a result of more sodium reaching the
collecting ducts. Thiazide diuretics have a role in the treatment of mild heart
failure although loop diuretics are better for reducing overload. The main use
of bendroflumethiazide was in the management of hypertension but recent NICE
guidelines now recommend other thiazide-like diuretics such as indapamide and
chlortalidone.
Common adverse effects
·
dehydration
·
postural hypotension
·
hyponatraemia, hypokalaemia, hypercalcaemia*
·
gout
·
impaired glucose tolerance
·
impotence
Rare adverse effects
·
thrombocytopaenia
·
agranulocytosis
·
photosensitivity rash
·
pancreatitis
|
|
|
|
|
|
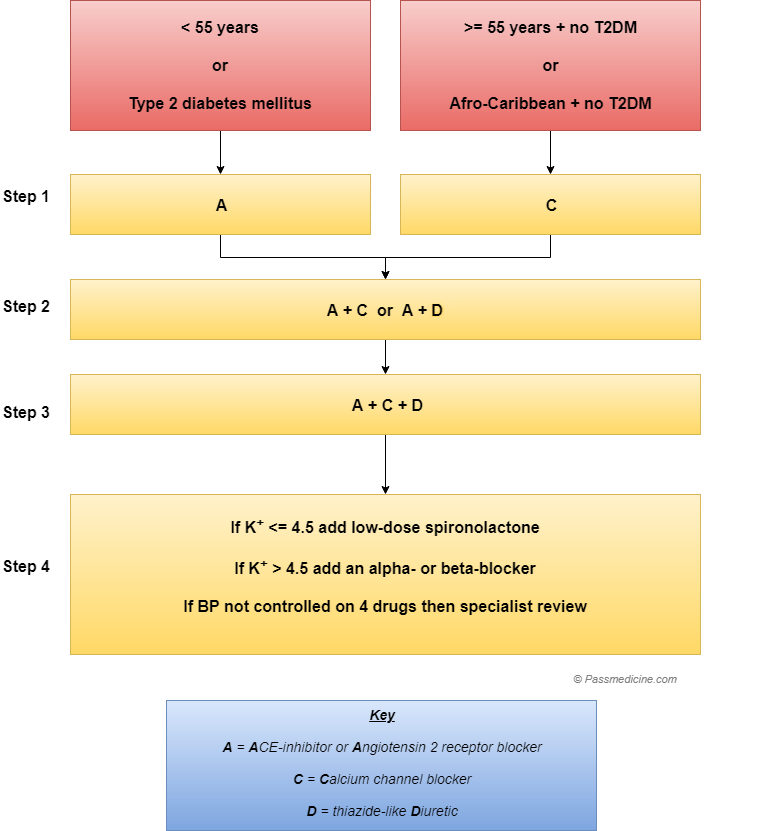
Flow chart showing the management of hypertension as per
current NICE guideliness
*the flip side of this is hypocalciuria, which may be useful in reducing the incidence of renal stones
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:52
Aortic dissection: management
Classification
Stanford classification
·
type A - ascending aorta, 2/3 of cases
·
type B - descending aorta, distal to left subclavian origin, 1/3
of cases
DeBakey classification
·
type I - originates in ascending aorta, propagates to at least
the aortic arch and possibly beyond it distally
·
type II - originates in and is confined to the ascending aorta
·
type III - originates in descending aorta, rarely extends
proximally but will extend distally
Management
Type A
·
surgical management, but blood pressure should be controlled to
a target systolic of 100-120 mmHg whilst awaiting intervention
Type B*
·
conservative management
·
bed rest
·
reduce blood pressure IV labetalol to prevent progression
Complications
Complications of backward tear
·
aortic incompetence/regurgitation
·
MI: inferior pattern often seen due to right coronary
involvement
Complications of forward tear
·
unequal arm pulses and BP
·
stroke
·
renal failure
|
|
|
|
©
Image used on license from Radiopaedia |
|

An intraluminal tear has formed a 'flap' that can be
clearly seen in the ascending aorta. This is a Stanford type A dissection
|
|
|
|
©
Image used on license from Radiopaedia |
|

Stanford type B dissection, seen in the descending aorta
*endovascular repair of type B
aortic dissection may have a role in the future
From <https://www.passmedicine.com/review/textbook.php?s=#>
Medical
management consists of decreasing heart rate, blood pressure and the shearing
forces of myocardial contractility in order to decrease the propagation
of the dissection.
Oral
verapamil is not suitable for precise BP control in the acute setting and IV
sodium nitroprusside does not slow down the heart rate.
Stanford
type A- ascending aorta dissection
·
control BP (IV
labetalol) + surgery
Stanford
type B - descending aortic dissection
·
control BP (IV
labetalol)
From <https://mle.ncl.ac.uk/cases/page/18128/>
24 December 2020
12:52
Atrial fibrillation: post-stroke
NICE issued guidelines on atrial
fibrillation (AF) in 2006. They included advice on the management of patients
with AF who develop a stroke or transient-ischaemic attack (TIA).
Recommendations include:
·
following a stroke or TIA, warfarin
or a direct thrombin or factor Xa inhibitor should be given as the anticoagulant of choice.
Antiplatelets should only be given if needed for the treatment of other
comorbidities
·
in acute stroke patients, in the absence of haemorrhage, anticoagulation
therapy should be commenced after 2 weeks. If imaging shows a very large cerebral infarction then the
initiation of anticoagulation should be delayed
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:52
Chest pain: assessment of patients with suspected
cardiac chest pain
NICE updated it's guidelines in
2016 on the 'Assessment and diagnosis of recent onset chest pain or discomfort
of suspected cardiac origin'.
Below is a brief summary of the key
points. Please see the link for more details.
Patients presenting with acute chest
pain
Immediate management of suspected
acute coronary syndrome (ACS)
·
glyceryl trinitrate
·
aspirin 300mg. NICE do not recommend giving other antiplatelet
agents (i.e. Clopidogrel) outside of hospital
·
do not routinely give oxygen, only give if sats < 94%*
·
perform an ECG as soon as possible but do not delay transfer to
hospital. A normal ECG does not exclude ACS
Referral
·
current chest pain or chest pain in the last 12 hours with an
abnormal ECG: emergency admission
·
chest pain 12-72 hours ago: refer to hospital the same-day for
assessment
·
chest pain > 72 hours ago: perform full assessment with ECG
and troponin measurement before deciding upon further action
*NICE suggest the following in
terms of oxygen therapy:
·
do not routinely administer oxygen, but monitor oxygen
saturation using pulse oximetry as soon as possible, ideally before hospital
admission. Only offer supplemental oxygen to:
·
people with oxygen saturation (SpO2) of less than 94% who are
not at risk of hypercapnic respiratory failure, aiming for SpO2 of 94-98%
·
people with chronic obstructive pulmonary disease who are at
risk of hypercapnic respiratory failure, to achieve a target SpO2 of 88-92%
until blood gas analysis is available.
Patients presenting with stable
chest pain
NICE define anginal pain as the
following:
·
1. constricting discomfort in the front of the chest, or in the
neck, shoulders, jaw or arms
·
2. precipitated by physical exertion
·
3. relieved by rest or GTN in about 5 minutes
·
patients with all 3 features have typical angina
·
patients with 2 of the above features have atypical angina
·
patients with 1 or none of the above features have non-anginal
chest pain
For patients in whom stable angina
cannot be excluded by clinical assessment alone NICE recommend the following
(e.g. symptoms consistent with typical/atypical angina OR ECG changes):
·
1st line: CT coronary angiography
·
2nd line: non-invasive functional imaging (looking for
reversible myocardial ischaemia)
·
3rd line: invasive coronary angiography
Examples of non-invasive functional
imaging:
·
myocardial perfusion scintigraphy with single photon emission
computed tomography (MPS with SPECT) or
·
stress echocardiography or
·
first-pass contrast-enhanced magnetic resonance (MR) perfusion
or
·
MR imaging for stress-induced wall motion abnormalities
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:52
Peri-arrest rhythms: bradycardia
The 2015 Resuscitation Council (UK)
guidelines emphasise that the management of bradycardia depends on:
·
1. identifying the presence of signs indicating haemodynamic
compromise - 'adverse signs'
·
2. identifying the potential risk of asystole
Adverse signs
The following factors indicate
haemodynamic compromise and hence the need for treatment:
·
shock: hypotension (systolic blood pressure < 90 mmHg),
pallor, sweating, cold, clammy extremities, confusion or impaired consciousness
·
syncope
·
myocardial ischaemia
·
heart failure
Atropine (500mcg IV) is the first
line treatment in this situation.
If there is an unsatisfactory
response the following interventions may be used:
·
atropine, up to maximum of 3mg
·
transcutaneous pacing
·
isoprenaline/adrenaline infusion titrated to response
Specialist help should be sought
for consideration of transvenous pacing if there is no response to the above
measures.
Potential risk of asystole
The following are risk factors for
asystole. Even if there is a satisfactory response to atropine specialist help
is indicated to consider the need for transvenous pacing:
·
complete heart block with broad complex QRS
·
recent asystole
·
Mobitz type II AV block
·
ventricular pause > 3 seconds
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:52
Thrombolysis
Thrombolytic drugs activate
plasminogen to form plasmin. This in turn degrades fibrin and help breaks up
thrombi. They in primarily used in patients who present with a ST elevation
myocardial infarction. Other indications include acute ischaemic stroke and
pulmonary embolism, although strict inclusion criteria apply.
Examples
·
alteplase
·
tenecteplase
·
streptokinase
Contraindications to thrombolysis
·
active internal bleeding
·
recent haemorrhage, trauma or surgery (including dental
extraction)
·
coagulation and bleeding disorders
·
intracranial neoplasm
·
stroke < 3 months
·
aortic dissection
·
recent head injury
·
severe hypertension
Side-effects
·
haemorrhage
·
hypotension - more common with streptokinase
·
allergic reactions may occur with streptokinase
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:53
Torsades de pointes
Torsades de pointes ('twisting of
the points') is a form of polymorphic ventricular tachycardia associated with a
long QT interval. It may deteriorate into ventricular fibrillation and hence
lead to sudden death.
Causes of long QT interval
·
congenital: Jervell-Lange-Nielsen syndrome, Romano-Ward syndrome
·
antiarrhythmics: amiodarone, sotalol, class 1a antiarrhythmic
drugs
·
tricyclic antidepressants
·
antipsychotics
·
chloroquine
·
terfenadine
·
erythromycin
·
electrolyte: hypocalcaemia, hypokalaemia, hypomagnesaemia
·
myocarditis
·
hypothermia
·
subarachnoid haemorrhage
Management
·
IV magnesium sulphate
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|
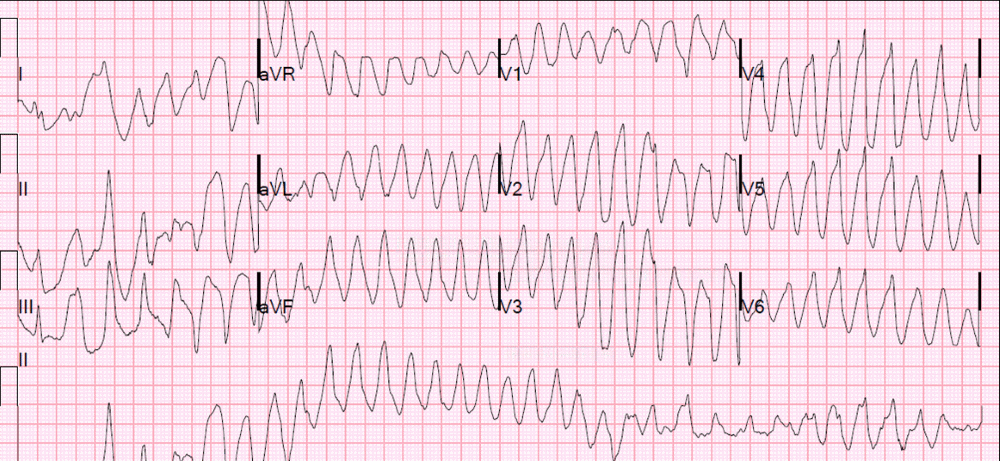
ECG showing torsades de pointes
From <https://www.passmedicine.com/review/textbook.php?s=#>
Pacing
is contraindicated in patients with torsades de pointes ventricular tachycardia
secondary to reversible causes.
From <https://mle.ncl.ac.uk/cases/page/18128/>
24 December 2020
12:53
Atrial fibrillation: a very basic introduction
Atrial fibrillation (AF) is the
most common sustained cardiac arrhythmia. It is very common, being present in
around 5% of patients over aged 70-75 years and 10% of patients aged 80-85
years. Whilst uncontrolled atrial fibrillation can result in symptomatic
palpitations and inefficient cardiac function probably the most important aspect
of managing patients with AF is reducing the increased risk of stroke which is
present in these patients.
Types of atrial fibrillation
AF may by classified as either
first detected episode, paroxysmal, persistent or permanent.
·
first detected episode (irrespective of whether it is
symptomatic or self-terminating)
·
recurrent episodes, when a patient has 2 or more episodes of AF.
If episodes of AF terminate spontaneously then the term paroxysmal
AF is used. Such
episodes last less than 7 days (typically < 24 hours). If the arrhythmia is
not self-terminating then the term persistent AF is used. Such episodes usually last
greater than 7 days
·
in permanent AF there is continuous atrial fibrillation which cannot be
cardioverted or if attempts to do so are deemed inappropriate. Treatment goals
are therefore rate control and anticoagulation if appropriate
Symptoms and signs
Symptoms
·
palpitations
·
dyspnoea
·
chest pain
Signs
·
an irregularly irregular pulse
Investigations
An ECG is essential to make the
diagnosis as other conditions can give an irregular pulse, such as ventricular
ectopics or sinus arrhythmia.
Management
There are two key parts of managing
patients with AF:
·
1. Rate/rhythm control
·
2. Reducing stroke risk
Rate vs. rhythm control
There are two main strategies
employed in dealing with the arrhythmia element of atrial fibrillation:
·
rate control: accept that the pulse will be irregular, but slow the rate
down to avoid negative effects on cardiac function
·
rhythm control: try to get the patient back into, and maintain, normal sinus
rhythm. This is termed cardioversion. Drugs (pharmacological cardioversion) and
synchronised DC electrical shocks (electrical cardioversion) may be used for
this purpose
For many years the predominant
approach was to try and maintain a patient in sinus rhythm. This approach
changed in the early 2000's and now the majority of patients are managed with a
rate control strategy. NICE advocate using a rate control strategy except in a
number of specific situations such as coexistent heart failure, first onset AF or where there is an obvious
reversible cause.
Rate control
A beta-blocker or a rate-limiting
calcium channel blocker (e.g. diltiazem) is used first-line
to control the rate in AF.
If one drug does not control the
rate adequately NICE recommend combination therapy with any 2 of the following:
·
a betablocker
·
diltiazem
·
digoxin
Rhythm control
As mentioned above there are a
subgroup of patients for whom a rhythm control strategy should be tried first.
Other patients may have had a rate control strategy initially but switch to
rhythm control if symptoms/heart rate fails to settle.
When considering cardioversion it
is very important to remember that the moment a patient switches from AF to
sinus rhythm presents the highest risk for embolism leading to stroke. Imagine
the thrombus formed in the fibrillating atrium suddenly being pushed out when
sinus rhythm is restored. For this reason patients must either have had a short
duration of symptoms (less than 48 hours) or be anticoagulated for a period of
time prior to attempting cardioversion.
Reducing stroke risk
Some patients with AF are at a very
low risk of stroke whilst others are at a very significant risk. Clinicians use
risk stratifying tools such as the CHA2DS2-VASc score to
determine the most appropriate anticoagulation strategy.
|
|
Risk factor |
Points |
|
C |
Congestive heart failure |
1 |
|
H |
Hypertension (or treated hypertension) |
1 |
|
A2 |
Age >= 75 years |
2 |
|
|
Age 65-74 years |
1 |
|
D |
Diabetes |
1 |
|
S2 |
Prior Stroke or TIA |
2 |
|
V |
Vascular disease (including ischaemic
heart disease and peripheral arterial disease) |
1 |
|
S |
Sex (female) |
1 |
The table below shows a suggested
anticoagulation strategy based on the score:
|
Score |
Anticoagulation |
|
0 |
No treatment |
|
1 |
Males: Consider anticoagulation Females: No treatment (this is because
their score of 1 is only reached due to their gender) |
|
2 or more |
Offer anticoagulation |
NICE recommend that we offer
patients a choice of anticoagulation, including warfarin and the novel oral
anticoagulants (NOACs).
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:53
ECG: hypokalaemia
ECG features of hypokalaemia
·
U waves
·
small or absent T waves (occasionally inversion)
·
prolong PR interval
·
ST depression
·
long QT
The ECG below shows typical U
waves. Note also the borderline PR interval.
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|
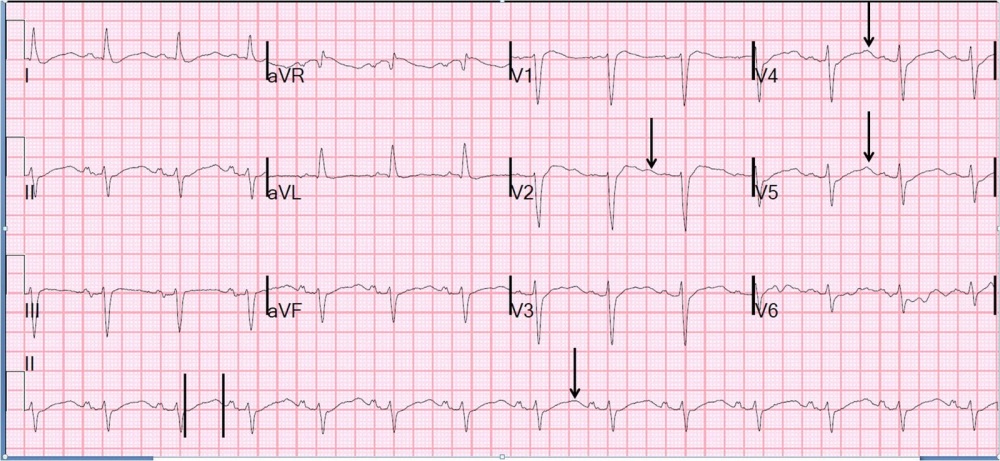
One registered user suggests the
following rhyme
·
In Hypokalaemia, U have no Pot and no T, but a long PR and a
long QT
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:53
ECG: normal variants
The following ECG changes are
considered normal variants in an athlete:
·
sinus bradycardia
·
junctional rhythm
·
first degree heart block
·
Wenckebach phenomenon
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:53
Loop diuretics
Furosemide and bumetanide are loop
diuretics that act by inhibiting
the Na-K-Cl cotransporter (NKCC) in the thick ascending limb of the loop of
Henle, reducing the absorption of NaCl. There are two variants of NKCC;
loop diuretics act on NKCC2, which is more prevalent in the kidneys.
Indications
·
heart failure: both acute (usually intravenously) and chronic
(usually orally)
·
resistant hypertension, particularly in patients with renal
impairment
Adverse effects
·
hypotension
·
hyponatraemia
·
hypokalaemia, hypomagnesaemia
·
hypochloraemic alkalosis
·
ototoxicity
·
hypocalcaemia
·
renal impairment (from dehydration + direct toxic effect)
·
hyperglycaemia (less common than with thiazides)
·
gout
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:54
Myocardial infarction: secondary prevention
NICE produced guidelines on the
management of patients following a myocardial infarction (MI) in 2013. Some key
points are listed below
All patients should be offered the
following drugs:
·
dual antiplatelet therapy (aspirin plus a second antiplatelet
agent)
·
ACE inhibitor
·
beta-blocker
·
statin
Some selected lifestyle points:
·
diet: advise a Mediterranean style diet, switch butter and
cheese for plant oil based products. Do not recommend omega-3 supplements or
eating oily fish
·
exercise: advise 20-30 mins a day until patients are 'slightly
breathless'
·
sexual activity may resume 4 weeks after an uncomplicated MI.
Reassure patients that sex does not increase their likelihood of a further MI.
PDE5 inhibitors (e.g, sildenafil) may be used 6 months after a MI. They should
however be avoided in patient prescribed either nitrates or nicorandil
Most patients who've had an acute
coronary syndrome are now given dual antiplatelet therapy (DAPT). Clopidogrel
was previously the second antiplatelet of choice. Now ticagrelor and prasugrel
(also ADP-receptor inhibitors) are more widely used. The NICE Clinical
Knowledge Summaries now recommend:
·
post acute coronary syndrome (medically managed): add ticagrelor
to aspirin, stop ticagrelor after 12 months
·
post percutaneous coronary intervention: add prasugrel or
ticagrelor to aspirin, stop the second antiplatelet after 12 months
·
this 12 month period may be altered for people at a high-risk of
bleeding or those who at high-risk of further ischaemic events
Aldosterone antagonists
·
patients who have had an acute MI and who have symptoms and/or
signs of heart failure and left ventricular systolic dysfunction, treatment
with an aldosterone antagonist licensed for post-MI treatment (e.g. eplerenone) should
be initiated within 3-14 days of the MI, preferably after ACE inhibitor therapy
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:54
Scoring systems
There are now numerous scoring
systems used in medicine. The table below lists some of the more common ones:
|
Scoring
system |
Notes |
|
CHA2DS2-VASc |
Used to determine the need to
anticoagulate a patient in atrial fibrillation |
|
ABCD2 |
Prognostic score for risk stratifying
patients who've had a suspected TIA |
|
NYHA |
Heart failure severity scale |
|
DAS28 |
Measure of disease activity in
rheumatoid arthritis |
|
Child-Pugh classification |
A scoring system used to assess the
severity of liver cirrhosis |
|
Wells score |
Helps estimate the risk of a patient
having a deep vein thrombosis |
|
MMSE |
Mini-mental state examination - used to
assess cognitive impairment |
|
HAD |
Hospital Anxiety and Depression (HAD)
scale - assesses severity of anxiety and depression symptoms |
|
PHQ-9 |
Patient Health Questionnaire - assesses
severity of depression symptoms |
|
GAD-7 |
Used as a screening tool and severity
measure for generalised anxiety disorder |
|
Edinburgh Postnatal Depression Score |
Used to screen for postnatal depression |
|
SCOFF |
Questionnaire used to detect eating
disorders and aid treatment |
|
AUDIT |
Alcohol screening tool |
|
CAGE |
Alcohol screening tool |
|
FAST* |
Alcohol screening tool |
|
CURB-65 |
Used to assess the prognosis of a
patient with pneumonia |
|
Epworth Sleepiness Scale |
Used in the assessment of suspected
obstructive sleep apnoea |
|
IPSS |
International prostate symptom score |
|
Gleason score |
Indicates prognosis in prostate cancer |
|
APGAR |
Assesses the health of a newborn
immediately after birth |
|
Bishop score |
Used to help assess the whether
induction of labour will be required |
|
Waterlow score |
Assesses the risk of a patient
developing a pressure sore |
|
FRAX |
Risk assessment tool developed by WHO
which calculates a patients 10-year risk of developing an osteoporosis
related fracture |
|
Ranson criteria |
Acute pancreatitis |
|
MUST |
Malnutrition |
*FAST is also mnemonic to help
patients/relatives identify the symptoms of a stroke
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Warfarin: interactions
Interactions of warfarin are
important both clinically and in terms of exams.
General factors that may potentiate
warfarin
·
liver disease
·
P450 enzyme inhibitors (see below)
·
cranberry juice
·
drugs which displace warfarin from plasma albumin, e.g. NSAIDs
·
inhibit platelet function: NSAIDs
Drugs which either inhibit or
induce the P450 system may affect the metabolism of warfarin and hence the INR:
|
Inducers
of the P450 system include - INR will decrease |
Inhibitors of the P450 system include -
INR will increase |
|
·
antiepileptics: phenytoin, carbamazepine ·
barbiturates: phenobarbitone ·
rifampicin ·
St John's Wort ·
chronic alcohol intake ·
griseofulvin ·
smoking (affects CYP1A2,
reason why smokers require more aminophylline) |
·
antibiotics: ciprofloxacin, clarithromycine/erythromycin ·
isoniazid ·
cimetidine,omeprazole ·
amiodarone ·
allopurinol ·
imidazoles: ketoconazole, fluconazole ·
SSRIs: fluoxetine, sertraline ·
ritonavir ·
sodium valproate ·
acute alcohol intake ·
quinupristin |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Adenosine
Adenosine is most commonly used to
terminate supraventricular
tachycardias. The effects of adenosine are enhanced by dipyridamole (antiplatelet agent) and blocked by theophyllines. It should be avoided
in asthmatics due to possible bronchospasm.
Mechanism of action
·
causes transient heart block in the AV node
·
agonist of the A1 receptor in the atrioventricular node, which
inhibits adenylyl cyclase thus reducing cAMP and causing hyperpolarization by
increasing outward potassium flux
·
adenosine has a very short half-life of about 8-10
seconds
Adenosine should ideally be infused
via a large-calibre
cannula due to it's short half-life,
Adverse effects
·
chest pain
·
bronchospasm
·
transient flushing
·
can enhance conduction down accessory pathways, resulting in
increased ventricular rate (e.g. WPW syndrome)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Amiodarone
Amiodarone is a class III
antiarrhythmic agent used in the treatment of atrial, nodal and ventricular
tachycardias. The main mechanism of action is by blocking potassium channels which inhibits repolarisation and hence prolongs the action
potential. Amiodarone also has other actions such as blocking sodium channels
(a class I effect)
The use of amiodarone is limited by
a number of factors
·
very long half-life (20-100 days). For this reason, loading
doses are frequently used
·
should ideally be given into central veins (causes thrombophlebitis)
·
has proarrhythmic effects due to lengthening of the QT interval
·
interacts with drugs commonly used concurrently (p450 inhibitor) e.g. Decreases metabolism of warfarin
·
numerous long-term adverse effects (see below)
Monitoring of patients taking
amiodarone
·
TFT, LFT, U&E, CXR prior to treatment
·
TFT, LFT every 6 months
Adverse effects of amiodarone use
·
thyroid dysfunction: both hypothyroidism and hyper-thyroidism
·
corneal deposits
·
pulmonary fibrosis/pneumonitis
·
liver fibrosis/hepatitis
·
peripheral neuropathy, myopathy
·
photosensitivity
·
'slate-grey' appearance
·
thrombophlebitis and injection site reactions
·
bradycardia
·
lengths QT interval
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Aortic regurgitation
Features
·
early diastolic murmur: intensity of the murmur is increased by
the handgrip manoeuvre
·
collapsing pulse
·
wide pulse pressure
·
Quincke's sign (nailbed pulsation)
·
De Musset's sign (head bobbing)
·
mid-diastolic Austin-Flint murmur in severe AR - due to partial
closure of the anterior mitral valve cusps caused by the regurgitation streams
Causes (due to valve disease)
·
rheumatic fever
·
infective endocarditis
·
connective tissue diseases e.g. RA/SLE
·
bicuspid aortic valve
Causes (due to aortic root disease)
·
aortic dissection
·
spondylarthropathies (e.g. ankylosing spondylitis)
·
hypertension
·
syphilis
·
Marfan's, Ehler-Danlos syndrome
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Chest pain
The table below gives
characteristic exam question features for conditions causing chest pain
|
Condition |
Characteristic exam feature |
|
Myocardial infarction |
Cardiac-sounding pain ·
heavy, central chest pain they may radiate to the
neck and left arm ·
nausea, sweating ·
elderly patients and diabetics may experience no
pain Risk factors for cardiovascular disease |
|
Pneumothorax |
History of asthma, Marfan's etc Sudden dyspnoea and pleuritic chest
pain |
|
Pulmonary embolism |
Sudden dyspnoea and pleuritic chest
pain Calf pain/swelling Current combined pill user, malignancy |
|
Pericarditis |
Sharp pain relieved by sitting forwards May be pleuritic in nature |
|
Dissecting aortic aneurysm |
'Tearing' chest pain radiating through
to the back Unequal upper limb blood pressure |
|
Gastro-oesophageal reflux disease |
Burning retrosternal pain Other possible symptoms include
regurgitation and dysphagia |
|
Musculoskeletal chest pain |
One of the most common diagnoses made
in the Emergency Department. The pain is often worse on movement or palpation. May be precipitated by trauma or
coughing |
|
Shingles |
Pain often precedes the rash |
Further notes:
Aortic dissection
·
This occurs when there is a flap or filling defect within the
aortic intima. Blood tracks into the medial layer and splits the tissues with
the subsequent creation of a false lumen. It most commonly occurs in the
ascending aorta or just distal to the left subclavian artery (less common). It
is most common in Afro-carribean males aged 50-70 years.
·
Patients usually present with a tearing intrascapular pain,
which may be similar to the pain of a myocardial infarct.
·
The dissection may spread either proximally or distally with
subsequent disruption to the arterial branches that are encountered.
·
In the Stanford classification system the disease is classified
into lesions with a proximal origin (Type A) and those that commence distal to
the left subclavian (Type B).
·
Diagnosis may be suggested by a chest x-ray showing a widened
mediastinum. Confirmation of the diagnosis is usually made by use of CT
angiography
·
Proximal (Type A) lesions are usually treated surgically, type B
lesions are usually managed non operatively.
Pulmonary embolism
·
Typically sudden onset of chest pain, haemoptysis, hypoxia and
small pleural effusions may be present.
·
Most patients will have an underlying deep vein thrombosis
·
Diagnosis may be suggested by various ECG findings including S
waves in lead I, Q waves in lead III and inverted T waves in lead III.
Confirmation of the diagnosis is usually made through use of CT pulmonary
angiography.
·
Treatment is with anticoagulation, in those patients who develop
a cardiac arrest or severe compromise from their PE, consideration may be given
to thrombolysis.
Myocardial infarction
·
Traditionally described as sudden onset of central, crushing
chest pain. It may radiate into the neck and down the left arm. Signs of
autonomic dysfunction may be present. The presenting features may be atypical
in the elderly and those with diabetes.
·
Diagnosis is made through identification of new and usually
dynamic ECG changes (and cardiac enzyme changes). Inferior and anterior
infarcts may be distinguished by the presence of specific ECG changes (usually
II, III and aVF for inferior, leads V1-V5 for anterior).
·
Treatment is with oral antiplatelet agents, primary coronary
angioplasty and/ or thrombolysis.
Perforated peptic ulcer
·
Patients usually develop sudden onset of epigastric abdominal
pain, it may be soon followed by generalised abdominal pain.
·
There may be features of antecendant abdominal discomfort, the
pain of gastric ulcer is typically worse immediately after eating.
·
Diagnosis may be made by erect chest x-ray which may show a
small amount of free intra-abdominal air (very large amounts of air are more
typically associated with colonic perforation).
·
Treatment is usually with a laparotomy, small defects may be
excised and overlaid with an omental patch, larger defects are best managed
with a partial gastrectomy.
Boerhaaves syndrome
·
Spontaneous rupture of the oesophagus that occurs as a result of
repeated episodes of vomiting.
·
The rupture is usually distally sited and on the left side.
·
Patients usually give a history of sudden onset of severe chest
pain that may complicate severe vomiting.
·
Severe sepsis occurs secondary to mediastinitis.
·
Diagnosis is CT contrast swallow.
·
Treatment is with thoracotomy and lavage, if less than 12 hours
after onset then primary repair is usually feasible, surgery delayed beyond 12
hours is best managed by insertion of a T tube to create a controlled fistula
between oesophagus and skin.
·
Delays beyond 24 hours are associated with a very high mortality
rate.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Complete heart block
Features
·
syncope
·
heart failure
·
regular bradycardia (30-50 bpm)
·
wide pulse pressure
·
JVP: cannon waves in neck
·
variable intensity of S1
Types of heart block
First degree heart block
·
PR interval > 0.2 seconds
Second degree heart block
·
type 1 (Mobitz I, Wenckebach): progressive prolongation of the
PR interval until a dropped beat occurs
·
type 2 (Mobitz II): PR interval is constant but the P wave is
often not followed by a QRS complex
Third degree (complete) heart block
·
there is no association between the P waves and QRS complexes
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|

ECG showing third degree (complete) heart block
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:55
Constrictive pericarditis
Causes
·
any cause of pericarditis
·
particularly TB
Features
·
dyspnoea
·
right heart failure: elevated JVP, ascites, oedema, hepatomegaly
·
JVP shows prominent x and y descent
·
pericardial knock - loud S3
·
Kussmaul's sign is positive
CXR
·
pericardial calcification
The key differences between
constrictive pericarditis and cardiac tamponade are summarized in the table
below:
|
|
Cardiac tamponade |
Constrictive pericarditis |
|
JVP |
Absent Y descent |
X + Y present |
|
Pulsus paradoxus |
Present |
Absent |
|
Kussmaul's sign* |
Rare |
Present |
|
Characteristic features |
|
Pericardial calcification on CXR |
A commonly used mnemonic to
remember the absent Y descent in cardiac tamponade is TAMponade = TAMpaX
*a paradoxical rise in JVP during
inspiration
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:58
Dabigatran
Dabigatran is an oral anticoagulant
that works by being a direct
thrombin inhibitor. It is one of the drugs developed
over the past 20 years as an alternative to warfarin, with the advantage that
it does not require regular monitoring.
What is dabigatran used for?
Dabigatran is currently used for
two main indications.
Firstly it is an option in the
prophylaxis of venous thromboembolism following hip or knee replacement
surgery.
Secondly, it is also licensed in
the UK for prevention of stroke in patients with non-valvular atrial
fibrillation who have one or more of the following risk factors present:
·
previous stroke, transient ischaemic attack or systemic embolism
·
left ventricular ejection fraction below 40%
·
symptomatic heart failure of New York Heart Association (NYHA)
class 2 or above
·
age 75 years or older
·
age 65 years or older with one of the following: diabetes
mellitus, coronary artery disease or hypertension
What are the known side-effects of
dabigatran?
Unsurprisingly haemorrhage is the
major adverse effect.
Doses should be reduced in chronic
kidney disease and dabigatran should not be prescribed if the creatinine
clearance is < 30 ml/min.
Reversing the effects
Idarucizumab can be used
for rapid reversal of the anticoagulant effects of dabigatran.
Drug Safety Update 2013
The RE-ALIGN study showed
significantly higher
bleeding and thrombotic events in patients with recent mechanical heart
valve replacement using dabigatran compared with warfarin.
Previously there had been no
guidance to support the use of dabigatran in patients with prosthetic heart
valves but the advice has now changed to dabigatran being contraindicated in
such patients.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:58
ECG: bi/tri-fascicular block
Bifascicular block
·
combination of RBBB with left anterior or posterior hemiblock
·
e.g. RBBB with left axis deviation
Trifascicular block
·
features of bifascicular block as above + 1st-degree heart block
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|
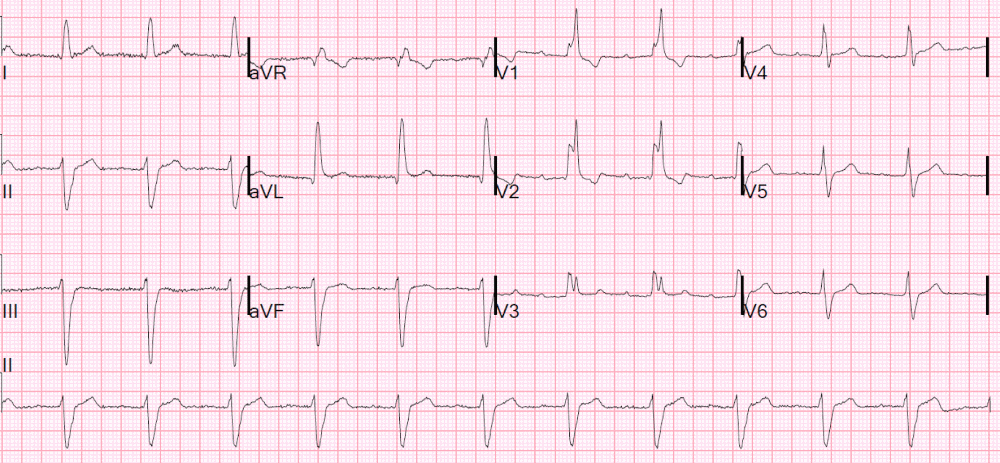
ECG showing trifascicular block: RBBB + left anterior
hemiblock + 1st-degree heart block
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:59
ECG: hypothermia
The following ECG changes may be
seen in hypothermia
·
bradycardia
·
'J' wave - small hump at the end of the QRS complex
·
first degree heart block
·
long QT interval
·
atrial and ventricular arrhythmias
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:59
Heart failure: NYHA classification
The New York Heart Association
(NYHA) classification is widely used to classify the severity of heart failure:
NYHA Class I
·
no symptoms
·
no limitation: ordinary physical exercise does not cause undue
fatigue, dyspnoea or palpitations
NYHA Class II
·
mild symptoms
·
slight limitation of physical activity: comfortable at rest but
ordinary activity results in fatigue, palpitations or dyspnoea
NYHA Class III
·
moderate symptoms
·
marked limitation of physical activity: comfortable at rest but
less than ordinary activity results in symptoms
NYHA Class IV
·
severe symptoms
·
unable to carry out any physical activity without discomfort:
symptoms of heart failure are present even at rest with increased discomfort
with any physical activity
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:59
Pulses
Pulsus paradoxus
·
greater than the normal (10 mmHg) fall in systolic blood
pressure during inspiration → faint or absent pulse in inspiration
·
severe asthma, cardiac
tamponade
Slow-rising/plateau
·
aortic stenosis
Collapsing
·
aortic regurgitation
·
patent ductus arteriosus
·
hyperkinetic states (anaemia, thyrotoxic, fever,
exercise/pregnancy)
Pulsus alternans
·
regular alternation of the force of the arterial pulse
·
severe LVF
Bisferiens pulse
·
'double pulse' - two systolic peaks
·
mixed aortic valve disease
'Jerky' pulse
·
hypertrophic obstructive cardiomyopathy*
*HOCM may occasionally
be associated with a bisferiens pulse
From <https://www.passmedicine.com/review/textbook.php?s=#>
|
Bounding |
CO2 retention, liver failure, sepsis |
|
Bisferiens |
mixed aortic stenosis and regurgitation |
|
Anacrotic |
Aortic stenosis |
|
Collapsing |
Aortic regurgitation |
From <https://mle.ncl.ac.uk/cases/page/18128/>
Jerky- HOCM
24 December 2020
12:59
Rheumatic fever
Rheumatic fever develops following
an immunological reaction to recent (2-6 weeks ago) Streptococcus pyogenes infection.
Pathogenesis
·
Streptococcus pyogenes infection → activation of the
innate immune system leading to antigen presentation to T cells
·
B and T cells produce IgG and IgM antibodies and CD4+ T cells
are activated
·
there is then a cross-reactive immune response (a form of type
II hypersensitivity) thought to be mediated by molecular
mimicry
·
the cell wall of Streptococcus pyogenes includes M protein, a virulence
factor that is highly antigenic. It is thought that the antibodies against M
protein cross-react with myosin and the smooth muscle of arteries
·
this response leads to the clinical features of rheumatic fever
·
Aschoff bodies describes the granulomatous nodules found in rheumatic
heart fever
Diagnosis is based on evidence of
recent streptococcal infection accompanied by:
·
2 major criteria
·
1 major with 2 minor criteria
Evidence of recent streptococcal
infection
·
raised or rising streptococci antibodies,
·
positive throat swab
·
positive rapid group A streptococcal antigen test
Major criteria
·
erythema marginatum
·
Sydenham's chorea: this is often a late
feature
·
polyarthritis
·
carditis and valvulitis (eg, pancarditis)*
·
subcutaneous nodules
Minor criteria
·
raised ESR or CRP
·
pyrexia
·
arthralgia (not if arthritis a major criteria)
·
prolonged PR interval
|
|
|
|
©
Image used on license from DermNet NZ |
|

Erythema marginatum is seen in around 10% of children
with rheumatic fever. It is rare in adults
*The latest iteration of the Jones
criteria (published in 2015) state that rheumatic carditis cannot be based on
pericarditis or myocarditis alone and that there must be evidence of
endocarditis (the clinical correlate of which is valvulitis which manifests as
a regurgitant murmur).
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:59
Ventricular tachycardia
Ventricular tachycardia (VT) is
broad-complex tachycardia originating from a ventricular ectopic focus. It has
the potential to precipitate ventricular fibrillation and hence requires urgent
treatment.
There are two main types of VT:
·
monomorphic VT: most commonly caused by myocardial infarction
·
polymorphic VT: A subtype of polymorphic VT is torsades de
pointes which is precipitated by prolongation of the QT interval. The causes of
a long QT interval are listed below
Causes of a prolonged QT interval
|
Congenital |
Drugs |
Other |
|
·
Jervell-Lange-Nielsen syndrome (includes deafness
and is due to an abnormal potassium channel) ·
Romano-Ward syndrome (no deafness) |
·
amiodarone, sotalol, class 1a antiarrhythmic drugs ·
tricyclic antidepressants, fluoxetine ·
chloroquine ·
terfenadine ·
erythromycin |
·
electrolyte: hypocalcaemia, hypokalaemia,
hypomagnesaemia ·
acute myocardial infarction ·
myocarditis ·
hypothermia ·
subarachnoid haemorrhage |
Management
If the patient has adverse signs
(systolic BP < 90 mmHg, chest pain, heart failure) then immediate
cardioversion is indicated. In the absence of such signs antiarrhythmics may be
used. If these fail, then electrical cardioversion may be needed with
synchronised DC shocks
Drug therapy
·
amiodarone: ideally administered through a central line
·
lidocaine: use with caution in severe left ventricular
impairment
·
procainamide
Verapamil should NOT be used in VT
If drug therapy fails
·
electrophysiological study (EPS)
·
implant able cardioverter-defibrillator (ICD) - this is
particularly indicated in patients with significantly impaired LV function
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:59
Acute coronary syndrome: a very basic introduction
Acute coronary syndrome (ACS) is an
umbrella term covering a number of acute presentations of ischaemic heart
disease.
It covers a number of
presentations, including
·
ST elevation myocardial infarction (STEMI)
·
non-ST elevation myocardial infarction (NSTEMI)
·
unstable angina
Before we go into more detail into
these presentations it's useful to take a step back and consider how such
conditions develop.
ACS generally develops in patients
who have ischaemic heart disease, either known or previously undetected.
Ischaemic heart disease is a term synonymous with coronary heart disease and
coronary artery disease. It describes the gradually build up of fatty plaques
within the walls of the coronary arteries. This leads to two main problems:
·
1. Gradual narrowing, resulting in less blood and therefore
oxygen reaching the myocardium at times of increased demand. This results in
angina, i.e. chest pain due to insufficient oxygen reaching the myocardium
during exertion
·
2. The risk of sudden plaque rupture. The fatty plaques which
have built up in the endothelium may rupture leading to sudden occlusion of the
artery. This can result in no blood/oxygen reaching the area of myocardium.
Remember that there are a large
number of factors which can increase the chance of a patient developing
ischaemic heart disease:
|
Unmodifiable
risk factors |
Modifiable risk factors |
|
Increasing age Male gender Family history |
Smoking Diabetes mellitus Hypertension Hypercholesterolaemia Obesity |
Pathophysiology
Ischaemic heart disease is a
complex process which develops over a number of years. A number of changes can
be seen:
·
initial endothelial dysfunction is triggered by a number of
factors such as smoking, hypertension and hyperglycaemia
·
this results in a number of changes to the endothelium including
pro-inflammatory, pro-oxidant, proliferative and reduced nitric oxide
bioavailability
·
fatty infiltration of the subendothelial space by low-density
lipoprotein (LDL) particles
·
monocytes migrate from the blood and differentiate into
macrophages. These macrophages then phagocytose oxidized LDL, slowly turning
into large 'foam cells'. As these macrophages die the result can further
propagate the inflammatory process.
·
smooth muscle proliferation and migration from the tunica media
into the intima results in formation of a fibrous capsule covering the fatty
plaque.
|
|
|
|
Image
sourced from Wikipedia |
|
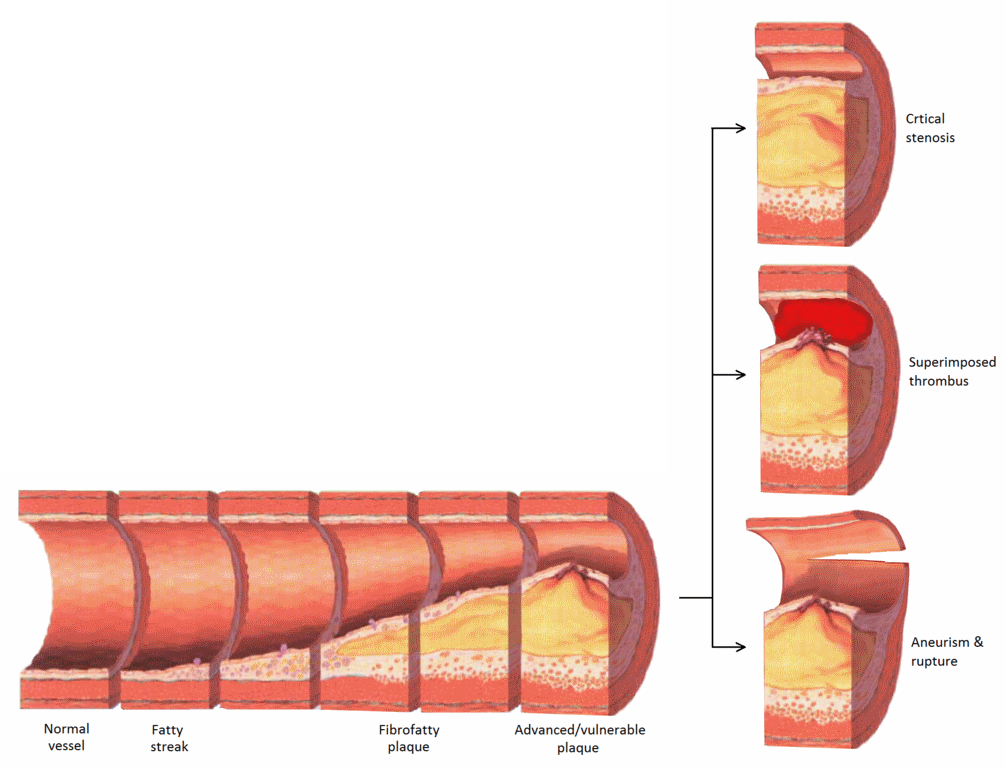
Diagram showing the progression of atherosclerosis in
the coronary arteries with associated complications on the right.
|
|
|
|
Image
sourced from Wikipedia |
|
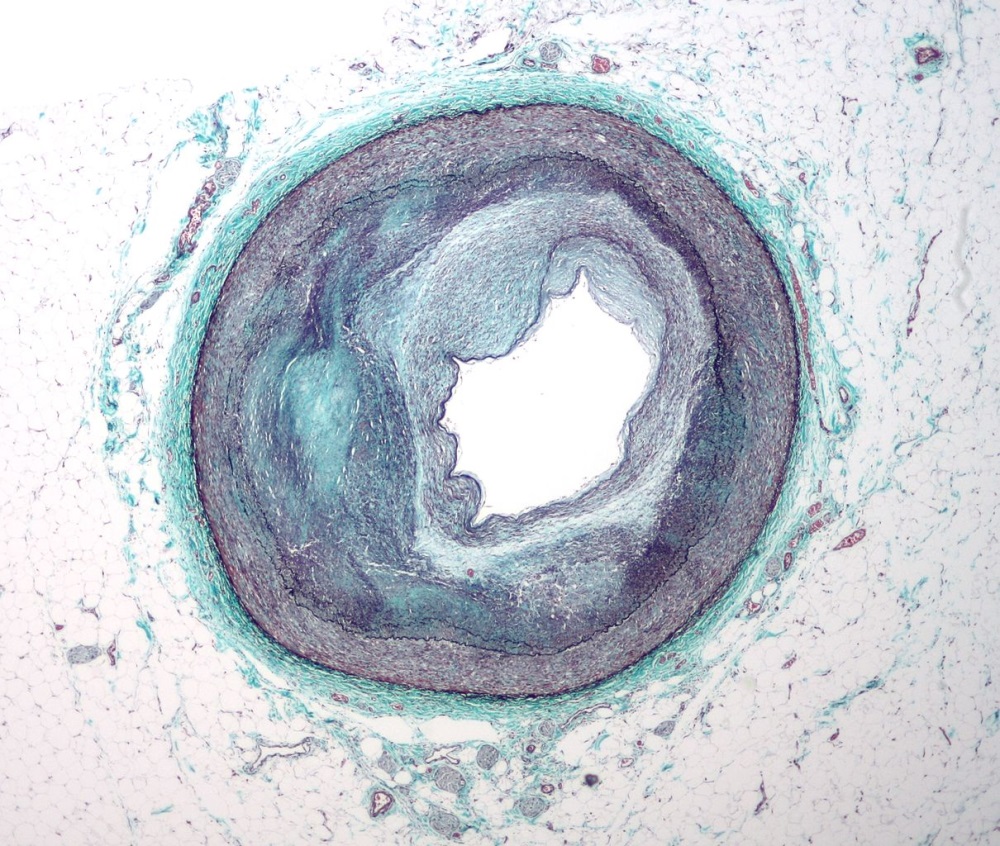
Slide showing a markedly narrowed coronary artery
secondary to atherosclerosis. Stained with Masson's trichrome.
Complications of atherosclerosis
Once a plaque has formed a number
of complications can develop:
·
the plaque forms a physical blockage in the lumen of the
coronary artery. This may cause reduced blood flow and hence oxygen to the
myocardium, particularly at times of increased demand, resulting clinically in
angina
·
the plaque may rupture, potentially causing a complete occlusion
of the coronary artery. This may result in a myocardial infarction
|
|
|
|
©
Image used on license from PathoPic |
|
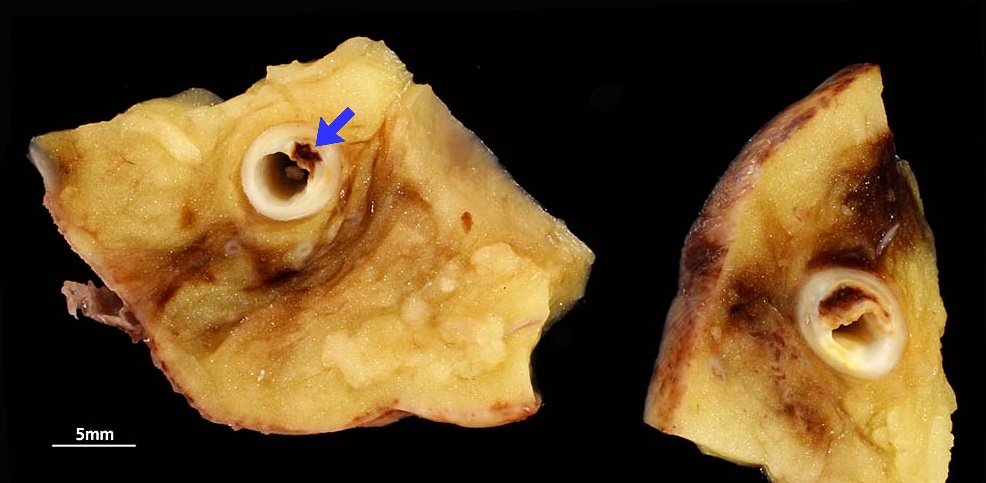
Ruptured coronary artery plaque resulting in thrombosis
and associated myocardial infarction.
|
|
|
|
©
Image used on license from PathoPic |
|

Pathological specimen showing infarction of the
anteroseptal and lateral wall of the left ventricle. There is a background of
biventricular myocardial hypertrophy.
Symptoms and signs
The classic and most common feature
of ACS is chest pain.
·
typically central/left-sided
·
may radiate to the jaw or the left arm
·
often described as 'heavy' or constricting, 'like an elephant on
my chest'
·
it should be noted however in real clinical practice patients
present with a wide variety of types of chest pain and patients/doctors may
confuse ischaemic pain for other causes such as dyspepsia
·
certain patients e.g. diabetics/elderly may not experience any
chest pain
Other symptoms in ACS include
·
dyspnoea
·
sweating
·
nausea and vomiting
Patients presenting with ACS often
have very few physical signs to ellicit:
·
pulse, blood pressure, temperature and oxygen saturations are
often normal or only mildly altered e.g. tachycardia
·
if complications of the ACS have developed e.g. cardiac failure
then clearly there may a number of findings
·
the patient may appear pale and clammy
Investigations
The two most important
investigations when assessing a patient with chest pain are:
·
ECG
·
cardiac markers e.g. troponin

ECG showing a ST elevation myocardial infarction
(STEMI). Note by how looking at which leads are affected (in this case II, III
and aVF) we are able to tell which coronary arteries are blocked (the right
coronary artery in this case). A blockage of the left anterior descending (LAD)
artery would cause elevation of V1-V4, what is often termed an 'anterior'
myocardial infarction.
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|
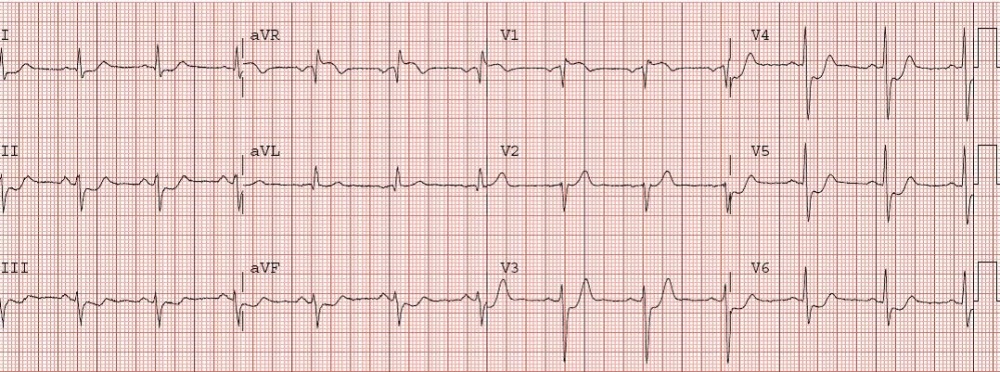
ECG showing a non-ST elevation myocardial infarction
(NSTEMI). On the ECG there is deep ST depression in I-III, aVF, and V3-V6. aVR
also has ST elevation. Deep and widespread ST depression is associated with
very high mortality because it signifies severe ischemia usually of LAD or left
main stem.
The table below shows a simplified
correlation between ECG changes and coronary territories:
|
|
ECG changes |
Coronary artery |
|
Anterior |
V1-V4 |
Left anterior descending |
|
Inferior |
II, III, aVF |
Right coronary |
|
Lateral |
I, V5-6 |
Left circumflex |
|
|
|
|
|
|
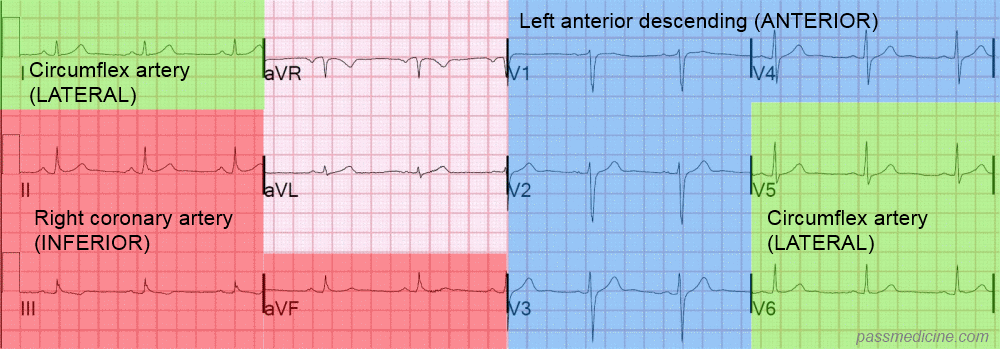
Diagram showing the correlation between ECG changes and
coronary territories in acute coronary syndrome
Management
Once a diagnosis of ACS has been
made there are a number of elements to treatment:
·
prevent worsening of presentation (i.e. further occlusion of
coronary vessel)
·
revascularise (i.e. 'unblock') the vessel if occluded (patients
presenting with a STEMI)
·
treat pain
A commonly taught mnemonic for the
treatment of ACS is MONA:
·
Morphine
·
Oxygen
·
Nitrates
·
Aspirin
Whilst useful it should be remember
that not all patients require oxygen therapy. British Thoracic Society
guidelines are now widely adopted and oxygen should only be given if the oxygen
saturations are < 94%.
For patients who've had a STEMI (i.e. one of the coronary arteries has become occluded) the
priority of management is to reopen, or revascularise, the blocked vessel.
·
a second antiplatelet drug should be given in addition to
aspirin. Options include clopidogrel, prasugrel and ticagrelor
·
for many years the treatment of choice was thrombolysis. This
involved the intravenous administration of a thrombolytic or 'clot-busting'
drug to breakdown the thrombus blocking the coronary artery
·
since the early 2000's thrombolysis has been superseded by
percutaneous coronary intervention (PCI). In this procedure the blocked
arteries are opened up using a balloon (angioplasty) following which a stent
may be deployed to prevent the artery occluding again in the future. This is
done via a catheter inserted into either the radial or femoral artery
If a patient presents with an NSTEMI then a risk stratification too (such as GRACE) is used to decide
upon further management. If a patient is considered high-risk or is clinically
unstable then coronary angiography will be performed during the admission. Lower
risk patients may have a coronary angiogram at a later date.
Secondary prevention
Patients who've had an ACS require
lifelong drug therapy to help reduce the risk of a further event. Standard
therapy comprises the following as a minimum:
·
aspirin
·
a second antiplatelet if appropriate (e.g. clopidogrel)
·
a beta-blocker
·
an ACE inhibitor
·
a statin
Further images
The following images show the
progress of coronary artery atherosclerosis:
|
|
|
|
©
Image used on license from PathoPic |
|

Normal coronary artery with blood in the lumen.
|
|
|
|
©
Image used on license from PathoPic |
|
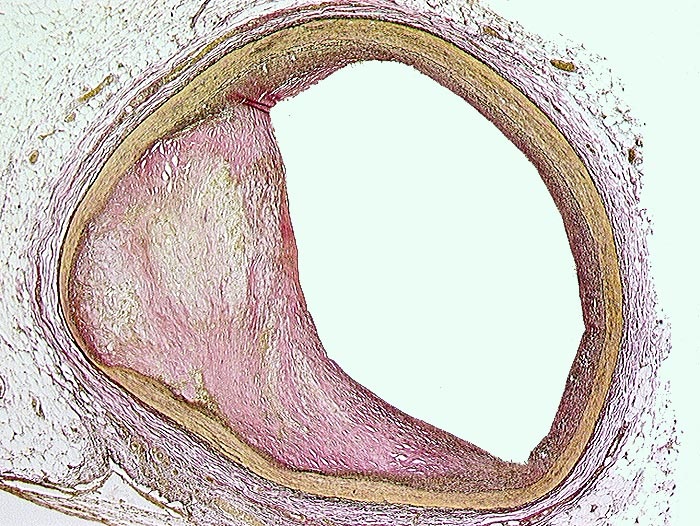
Slightly stenosed coronary artery
|
|
|
|
©
Image used on license from PathoPic |
|

Moderately stenosed coronary artery, beetween 50-75%
|
|
|
|
©
Image used on license from PathoPic |
|
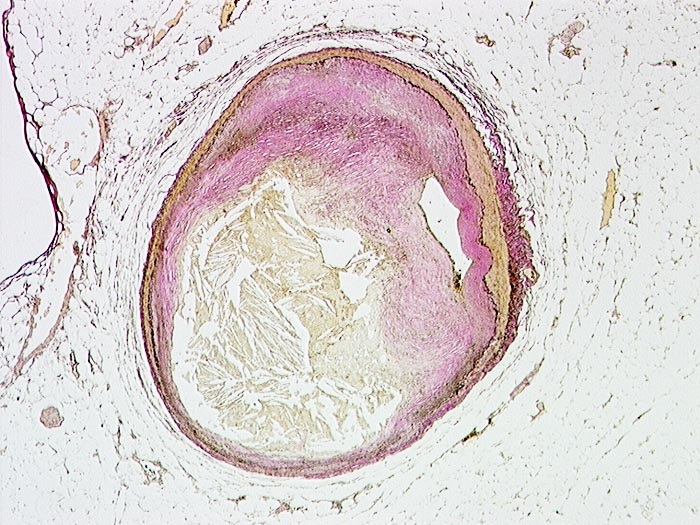
Severely stenosed coronary artery
|
|
|
|
©
Image used on license from PathoPic |
|
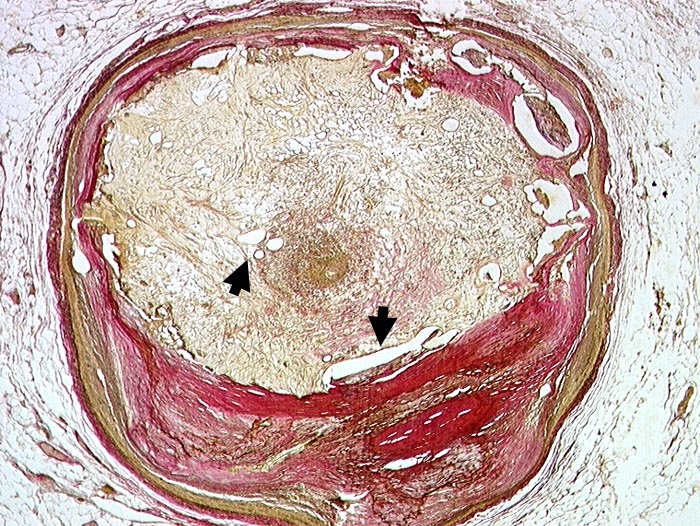
Recanalised old atherothrombotic occlusion of a coronary
artery. Numerous small neolumina recanalising the organised occluding thrombus
(indicated with arrows)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
12:59
Acute coronary syndrome: prognostic factors
The 2006 Global Registry of Acute
Coronary Events (GRACE) study has been used to derive regression models to
predict death in hospital and death after discharge in patients with acute
coronary syndrome
Poor prognostic factors
·
age
·
development (or history) of heart failure
·
peripheral vascular disease
·
reduced systolic blood pressure
·
Killip class*
·
initial serum creatinine concentration
·
elevated initial cardiac markers
·
cardiac arrest on admission
·
ST segment deviation
*Killip class - system used
to stratify risk post myocardial infarction
|
Killip
class |
Features |
30 day mortality |
|
I |
No clinical signs heart failure |
6% |
|
II |
Lung crackles, S3 |
17% |
|
III |
Frank pulmonary oedema |
38% |
|
IV |
Cardiogenic shock |
81% |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:00
Atrial fibrillation: pharmacological cardioversion
NICE published guidelines on the
management of atrial fibrillation (AF) in 2014. The following is also based on
the joint American Heart Association (AHA), American College of Cardiology
(ACC) and European Society of Cardiology (ESC) 2016 guidelines
Agents with proven efficacy in the
pharmacological cardioversion of atrial fibrillation
·
amiodarone
·
flecainide (if no structural heart disease)
·
others (less commonly used in UK): quinidine, dofetilide,
ibutilide, propafenone
Less effective agents
·
beta-blockers (including sotalol)
·
calcium channel blockers
·
digoxin
·
disopyramide
·
procainamide
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:00
Atrial septal defects
Atrial septal defects (ASDs) are
the most likely congenital heart defect to be found in adulthood. They carry a
significant mortality, with 50% of patients being dead at 50 years. Two types
of ASDs are recognised, ostium secundum and ostium primum. Ostium secundum are
the most common
Features
·
ejection systolic murmur, fixed splitting of S2
·
embolism may pass from venous system to left side of heart
causing a stroke
Ostium secundum (70% of ASDs)
·
associated with Holt-Oram syndrome (tri-phalangeal thumbs)
·
ECG: RBBB with RAD
Ostium primum
·
present earlier than ostium secundum defects
·
associated with abnormal AV valves
·
ECG: RBBB with LAD, prolonged PR interval
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:01
B-type natriuretic peptide
B-type natriuretic peptide (BNP) is
a hormone produced mainly by the left ventricular myocardium in response to strain.
Whilst heart failure is the most
obvious cause of raised BNP levels any cause of left ventricular dysfunction
such as myocardial ischaemia or valvular disease may raise levels. Raised
levels may also be seen due to reduced excretion in patients with chronic kidney disease. Factors which reduce BNP levels include treatment with ACE
inhibitors, angiotensin-2 receptor blockers and diuretics.
Effects of BNP
·
vasodilator
·
diuretic and natriuretic
·
suppresses both sympathetic tone and the
renin-angiotensin-aldosterone system
Clinical uses of BNP
Diagnosing patients with acute
dyspnoea
·
a low concentration of BNP(< 100pg/ml) makes a diagnosis of
heart failure unlikely, but raised levels should prompt further investigation
to confirm the diagnosis
·
NICE currently recommends BNP as a helpful test to rule out a
diagnosis of heart failure
Prognosis in patients with chronic
heart failure
·
initial evidence suggests BNP is an extremely useful marker of
prognosis
Guiding treatment in patients with
chronic heart failure
·
effective treatment lowers BNP levels
Screening for cardiac dysfunction
·
not currently recommended for population screening
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:01
Cardiac enzymes and protein markers
Interpretation of the various
cardiac enzymes has now largely been superceded by the introduction of troponin
T and I. Questions still however commonly appear in exams.
Key points for the exam
·
myoglobin is the first to rise
·
CK-MB is useful to look for reinfarction as it returns to
normal after 2-3 days (troponin T remains elevated for up to 10 days)
|
|
Begins to rise |
Peak value |
Returns to normal |
|
Myoglobin |
1-2 hours |
6-8 hours |
1-2 days |
|
CK-MB |
2-6 hours |
16-20 hours |
2-3 days |
|
CK |
4-8 hours |
16-24 hours |
3-4 days |
|
Trop T |
4-6 hours |
12-24 hours |
7-10 days |
|
AST |
12-24 hours |
36-48 hours |
3-4 days |
|
LDH |
24-48 hours |
72 hours |
8-10 days |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:01
Chronic heart failure: diagnosis
NICE issued updated guidelines on
diagnosis and management in 2018. Previously the first-line investigation was
determined by whether the patient has previously had a myocardial infarction or
not this is no longer the case - all patients should have an N-terminal
pro-B-type natriuretic peptide (NT‑proBNP) blood test first-line.
Interpreting the test
·
if levels are 'high' arrange specialist assessment (including
transthoracic echocardiography) within 2 weeks
·
if levels are 'raised' arrange specialist assessment (including
transthoracic echocardiography) echocardiogram within 6 weeks
Serum natriuretic peptides
B-type natriuretic peptide (BNP) is
a hormone produced mainly by the left ventricular myocardium in response to
strain. Very high levels are associated with a poor prognosis.
|
|
BNP |
NTproBNP |
|
High levels |
> 400 pg/ml (116 pmol/litre) |
> 2000 pg/ml (236 pmol/litre) |
|
Raised levels |
100-400 pg/ml (29-116 pmol/litre) |
400-2000 pg/ml (47-236 pmol/litre) |
|
Normal levels |
< 100 pg/ml (29 pmol/litre) |
< 400 pg/ml (47 pmol/litre) |
Factors which alter the BNP level:
|
Increase
BNP levels |
Decrease BNP levels |
|
Left ventricular hypertrophy Ischaemia Tachycardia Right ventricular overload Hypoxaemia (including pulmonary
embolism) GFR < 60 ml/min Sepsis COPD Diabetes Age > 70 Liver cirrhosis |
Obesity Diuretics ACE inhibitors Beta-blockers Angiotensin 2 receptor blockers Aldosterone antagonists |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:01
DVLA: cardiovascular disorders
The guidelines below relate to
car/motorcycle use unless specifically stated. For obvious reasons, the rules
relating to drivers of heavy goods vehicles tend to be much stricter
Specific rules
·
hypertension
o can drive unless treatment causes
unacceptable side effects, no need to notify DVLA
o if Group 2 Entitlement the
disqualifies from driving if resting BP consistently 180 mmHg systolic or more
and/or 100 mm Hg diastolic or more
·
angioplasty (elective) - 1 week off driving
·
CABG - 4 weeks off driving
·
acute coronary syndrome- 4 weeks off driving
o 1 week if successfully treated by
angioplasty
·
angina - driving must cease if symptoms occur at rest/at the
wheel
·
pacemaker insertion - 1 week off driving
·
implantable cardioverter-defibrillator (ICD)
o if implanted for sustained
ventricular arrhythmia: cease driving for 6 months
o if implanted prophylactically then
cease driving for 1 month. Having an ICD results in a permanent
bar for Group 2 drivers
·
successful catheter ablation for an arrhythmia- 2 days off
driving
·
aortic aneurysm of 6cm or more - notify DVLA. Licensing will be
permitted subject to annual review.
o an aortic diameter of 6.5 cm or
more disqualifies patients from driving
·
heart transplant: do not drive for 6 weeks, no need to notify
DVLA
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:09
Eisenmenger's syndrome
Eisenmenger's syndrome describes
the reversal of a left-to-right shunt in a congenital heart defect due to
pulmonary hypertension. This occurs when an uncorrected left-to-right leads to
remodeling of the pulmonary microvasculature, eventually causing obstruction to
pulmonary blood and pulmonary hypertension.
Associated with
·
ventricular septal defect
·
atrial septal defect
·
patent ductus arteriosus
Features
·
original murmur may disappear
·
cyanosis
·
clubbing
·
right ventricular failure
·
haemoptysis, embolism
Management
·
heart-lung transplantation is required
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:09
Heart failure: acute management
Management options in acute heart
failure include:
·
oxygen
·
IV loop diuretics
·
opiates
·
vasodilators
·
inotropic agents
·
CPAP
·
ultrafiltration
·
mechanical circulatory assistance: e.g. intra-aortic balloon
counterpulsation or ventricular assist devices
Consideration should be given to
discontinuing beta-blockers in the short-term.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:09
Heart sounds
The first heart sound (S1) is
caused by closure of the mitral and tricuspid valves whilst the second heart
sound (S2) is due to aortic and pulmonary valve closure
S1
·
closure of mitral and tricuspid valves
·
soft if long PR or mitral regurgitation
·
loud in mitral stenosis
S2
·
closure of aortic and pulmonary valves
·
soft in aortic stenosis
·
splitting during inspiration is normal
S3 (third heart sound)
·
caused by diastolic filling of the ventricle
·
considered normal if < 30 years old (may persist in women up to 50
years old)
·
heard in left ventricular failure (e.g. dilated cardiomyopathy), constrictive pericarditis (called a pericardial knock) and mitral regurgitation
S4 (fourth heart sound)
·
may be heard in aortic stenosis, HOCM, hypertension
·
caused by atrial contraction against a stiff
ventricle
o therefore coincides with the P wave on ECG
·
in HOCM a double apical impulse may be felt as a result of a
palpable S4
Sites of auscultation
|
Valve |
Site |
|
Pulmonary valve |
Left second intercostal space, at the
upper sternal border |
|
Aortic valve |
Right second intercostal space, at the
upper sternal border |
|
Mitral valve |
Left fifth intercostal space, just
medial to mid clavicular line |
|
Tricuspid valve |
Left fourth intercostal space, at the
lower left sternal border |
The diagram below demonstrates
where the various cardiac valves are best heard.
|
|
|
|
Image
sourced from Wikipedia |
|
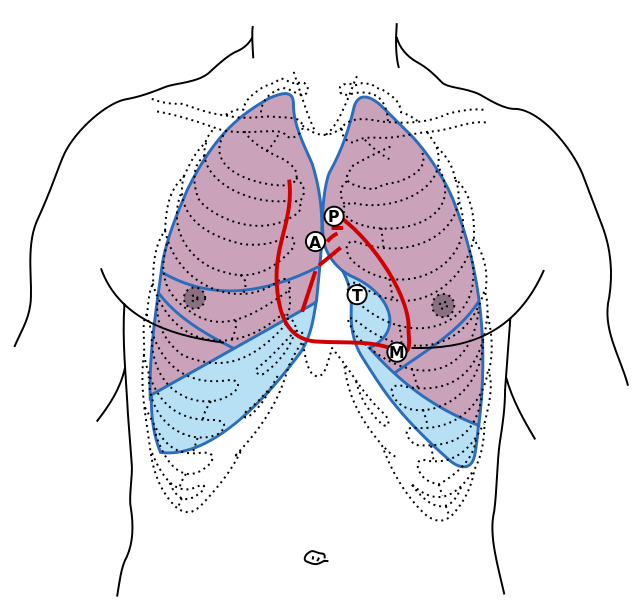
From <https://www.passmedicine.com/review/textbook.php?s=#>
Left
ventricular volume overload causes a third heart sound.

Cannon
waves occur when the atrium contracts against a closing tricuspid valve.
Cannon
waves happen only when P waves fall within QT intervals in ECG. P wave
represents atrial systolic contraction and QT represents ventricular
systole. When the atrium contracts against a closed tricuspid valve
during a ventricular contraction, a cannon wave projecting into the neck is
seen.
From <https://mle.ncl.ac.uk/cases/page/18128/>
24 December 2020
13:09
Hypothermia
Hypothermia is an unintentional
reduction of core body temperature below the normal physiological limits. In
initial stages, thermoreceptors in the skin and subcutaneous tissues sense the
low temperature and cause a regional vasoconstriction. This causes the hypothalamus
to stimulate the release of TSH and ACTH. It also stimulates heat production by
promoting shivering.
Definitions:
·
Mild hypothermia: 32-35°C
·
Moderate or severe hypothermia: < 32°C
Epidemiology:
·
The incidence of hypothermia varies globally. In the UK, the
estimated annual number of hypothermia-related deaths is 300/year, whereas in
Canada, it is 8000/year.
·
Hypothermia is most common during the winter, and the elderly
are particularly susceptible (see further risk factors below). Many cases of
hypothermia also occur indoors, due to poor heating facilities.
Causes can include:
·
Exposure to cold in the environment is the major cause
·
Inadequate insulation in the operating room
·
Cardiopulmonary bypass
·
Newborn babies.
Risk factors:
·
General anaesthesia
·
Substance abuse
·
Hypothyroidism
·
Impaired mental status
·
Homelessness
·
Extremes of age
Signs of hypothermia include:
·
shivering
·
cold and pale skin. Frostbite occurs when the skin and
subcutaneous tissue freeze, causing damage to cells.
·
slurred speech
·
tachypnoea, tachycardia and hypertension (if mild)
·
respiratory depression, bradycardia and hypothermia (if
moderate)
·
confusion/ impaired mental state
Babies with hypothermia can look
healthy. However, they may be limp, unusually quiet and refuse to feed. Heat
loss in newborns is extremely common, hence a hat and clothing/ blankets will
be applied soon after birth.
Investigations:
·
Temperature. Special low-reading rectal thermometers or
thermistor probes are preferred for measuring core body temperature. The
patient's temperature should be tracked over time, to check for improvement.
·
12 lead ECG. As the core temperature approaches 32°C to 33°C,
acute ST-elevation and J waves or Osborn waves may appear
·
FBC, serum electrolytes. Haemoglobin and haematocrit can be
elevated (due to haemoconcentration). Platelets and WBCs are low due to
sequestration in the spleen. Monitoring potassium is advised as hypothermic
patients can be hypokalaemic due to a shift of potassium into the intracellular
space.
·
Blood glucose. Stress hormones are increased, and the body can
have more peripheral resistance to insulin.
·
Arterial blood gas
·
Coagulation factors
·
Chest X-ray
Initial management includes:
·
Removing the patient from the cold environment and removing any
wet/cold clothing,
·
Warming the body with blankets
·
Securing the airway and monitoring breathing,
·
If the patient is not responding well to passive warming, you
may consider maintaining circulation using warm IV fluids or applying forced
warm air directly to the patient's body
+ rapid re-warming can lead to
peripheral vasodilation and shock
·
In severe cases, be prepared to conduct CPR. IV drugs should be
avoided if possible, as the patient is more likely to have a drastic response
to the drug.
For reference, the NHS also
provides advice to the public for what NOT to do when a person has hypothermia
(due to the risk of cardiac arrest):
·
Don't put the person into a hot bath.
·
Don't massage their limbs.
·
Don't use heating lamps.
·
Don't give them alcohol to drink.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:09
Infective endocarditis: features
Modified Duke criteria
Infective endocarditis diagnosed if
·
pathological criteria positive, or
·
2 major criteria, or
·
1 major and 3 minor criteria, or
·
5 minor criteria
Pathological criteria
Positive histology or microbiology
of pathological material obtained at autopsy or cardiac surgery (valve tissue,
vegetations, embolic fragments or intracardiac abscess content)
Major criteria
Positive blood cultures
·
two positive blood cultures showing typical organisms consistent
with infective endocarditis, such as Streptococcus viridans and the HACEK group, or
·
persistent bacteraemia from two blood cultures taken > 12
hours apart or three or more positive blood cultures where the pathogen is less
specific such as Staph aureus and Staph
epidermidis, or
·
positive serology for Coxiella burnetii, Bartonella species or Chlamydia
psittaci, or
·
positive molecular assays for specific gene targets
Evidence of endocardial involvement
·
positive echocardiogram (oscillating structures, abscess
formation, new valvular regurgitation or dehiscence of prosthetic valves), or
·
new valvular regurgitation
Minor criteria
·
predisposing heart condition or intravenous drug use
·
microbiological evidence does not meet major criteria
·
fever > 38ºC
·
vascular phenomena: major emboli, splenomegaly, clubbing,
splinter haemorrhages, Janeway lesions, petechiae or purpura
·
immunological phenomena: glomerulonephritis, Osler's nodes, Roth
spots
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:10
Infective endocarditis: prophylaxis
The 2008 guidelines from NICE have
radically changed the list of procedures for which antibiotic prophylaxis is
recommended
NICE recommends the following
procedures do not require prophylaxis:
·
dental procedures
·
upper and lower gastrointestinal tract procedures
·
genitourinary tract; this includes urological, gynaecological
and obstetric procedures and childbirth
·
upper and lower respiratory tract; this includes ear, nose and
throat procedures and bronchoscopy
The guidelines do however suggest:
·
any episodes of infection in people at risk of infective
endocarditis should be investigated and treated promptly to reduce the risk of
endocarditis developing
·
if a person at risk of infective endocarditis is receiving
antimicrobial therapy because they are undergoing a gastrointestinal or
genitourinary procedure at a site where there is a suspected infection they
should be given an antibiotic that covers organisms that cause infective
endocarditis
It is important to note that these
recommendations are not in keeping with the American Heart Association/European
Society of Cardiology guidelines which still advocate antibiotic prophylaxis
for high-risk patients who are undergoing dental procedures.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:10
Postural hypotension
Postural hypotension may be defined
as a fall of systolic blood pressure > 20 mmHg on standing.
Causes
·
hypovolaemia
·
autonomic dysfunction: diabetes, Parkinson's
·
drugs: diuretics, antihypertensives, L-dopa, phenothiazines,
antidepressants, sedatives
·
alcohol
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:10
Pulmonary embolism
Potential features of pulmonary
embolism include:
·
chest pain
o typically pleuritic
·
dyspnoea
·
haemoptysis
·
tachycardia
·
tachypnoea
·
respiratory examination
o classically the chest will be clear
o however, in real-world clinical
practice findings are often found (see below for more details)
We know from experience that few
patients (around 10%) present with the medical student textbook triad of pleuritic
chest pain, dyspnoea and haemoptysis. Pulmonary embolism can be difficult to
diagnose as it can present with virtually any cardiorespiratory symptom/sign
depending on it's location and size.
So which features make pulmonary
embolism more likely?
The PIOPED study1 in 2007
looked at the frequency of different symptoms and signs in patients who were
diagnosed with pulmonary embolism.
The relative frequency of common
clinical signs is shown below:
·
Tachypnea (respiratory rate >16/min) - 96%
·
Crackles - 58%
·
Tachycardia (heart rate >100/min) - 44%
·
Fever (temperature >37.8°C) - 43%
It is interesting to note that the
Well's criteria for diagnosing a PE use tachycardia rather than tachypnoea.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:10
Takayasu's arteritis
pulseless disease of Asian young females
Takayasu's arteritis is a large
vessel vasculitis. It typically causes occlusion of the aorta and questions
commonly refer to an absent limb pulse. It is more common in females and Asian
people
Features
·
systemic features of a vasculitis e.g. malaise, headache
·
unequal blood pressure in the upper limbs
·
carotid bruit
·
intermittent claudication
·
aortic regurgitation (around 20%)
Investigation:
magnetic resonance angiography.
|
|
|
|
|
|

Angiography showing multiple stenoses in the branches of
the aorta secondary to Takayasu's arteritis
Associations
·
renal artery stenosis
Management
·
steroids
From <https://www.passmedicine.com/review/textbook.php?s=#>

24 December 2020
13:10
Ventricular septal defect
Ventricular septal defects (VSD)
are the most common cause of congenital heart disease. They close spontaneously
in around 50% of cases. Congenital VSDs are associated with chromosomal
disorders (e.g. Down's syndrome, Edward's syndrome, Patau syndrome) and single
gene disorders such as Non-congenital causes include post myocardial infarction
Features
·
classically a pan-systolic murmur which is louder in smaller
defects
Complications
·
aortic regurgitation*
·
infective endocarditis
·
Eisenmenger's complex
·
right heart failure
·
pulmonary hypertension: pregnancy is contraindicated in women
with pulmonary hypertension as it carries a 30-50% risk of mortality
*aortic regurgitation is due to a
poorly supported right coronary cusp resulting in cusp prolapse
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:10
Abdominal aorta aneurysm
- Abdominal aortic aneurysms are a
common problem in vascular surgery.
·
They may occur as either true or false aneurysm. With the former
all 3 layers of the arterial wall are involved, in the latter only a single
layer of fibrous tissue forms the aneurysm wall.
·
True abdominal aortic aneurysms have an approximate incidence of
0.06 per 1000 people. They are commonest in elderly men and for this reason the
UK is now introducing the aneurysm screening program with the aim of performing
an abdominal aortic ultrasound measurement in all men aged 65 years.
Causes
·
Several different groups of patients suffer from aneurysmal
disease.
·
The commonest group is those who suffer from standard arterial
disease, i.e. Those who are hypertensive, have diabetes and have been or are smokers.
·
Other patients such as those suffering from connective tissue diseases such as Marfan's may also develop aneurysms.
In patients with abdominal aortic aneurysms the extracellular matrix becomes
disrupted with a change in the balance of collagen and elastic fibres.
Management
·
Most abdominal aortic aneurysms are an incidental finding.
·
Symptoms most often relate to rupture or impending rupture.
·
20% rupture anteriorly into the peritoneal cavity. Very poor
prognosis.
·
80% rupture posteriorly into the retroperitoneal space
·
The risk of rupture is related to aneurysm size, only 2% of
aneurysms measuring less than 4cm in diameter will rupture over a 5 year
period. This contrasts with 75% of aneurysms measuring over 7cm in diameter.
·
This is well explained by Laplaces' law which relates size to
transmural pressure.
·
For this reason most vascular surgeons will subject patients
with an aneurysm size of 5cm or greater to CT scanning of the chest, abdomen
and pelvis with the aim of delineating anatomy and planning treatment.
Depending upon co-morbidities, surgery is generally offered once the aneurysm
is between 5.5cm and 6cm.
A CT reconstruction showing an
infrarenal abdominal aortic aneurysm. The walls of the sac are calcified which
may facilitate identification on plain x-rays
|
|
|
|
Image
sourced from Wikipedia |
|

Indications for surgery
·
Symptomatic aneurysms (80% annual mortality if untreated)
·
Increasing size above 5.5cm if asymptomatic
·
Rupture (100% mortality without surgery)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:10
Acute coronary syndrome: clincial features
Features of acute coronary syndrome
(ACS) include:
·
chest pain: classically on the left side of the chest. May
radiate to the left arm or neck. This may not be present in elderly or diabetic
patients
·
dyspnoea
·
nausea and vomiting
·
sweating
·
palpitations
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:11
Antiplatelets: summary of latest guidance
The table below summarises the most
recent guidelines regarding antiplatelets:
|
Diagnosis |
1st line |
2nd line |
|
Acute coronary syndrome (medically
treated) |
Aspirin (lifelong) & ticagrelor (12
months) |
If aspirin contraindicated, clopidogrel
(lifelong) |
|
Percutaneous coronary intervention |
Aspirin (lifelong) & prasurgrel or
ticagrelor (12 months) |
If aspirin contraindicated, clopidogrel
(lifelong) |
|
TIA |
Clopidogrel (lifelong) |
Aspirin (lifelong)
& dipyridamole (lifelong) |
|
Ischaemic stroke |
Clopidogrel
(lifelong) |
Aspirin (lifelong) & dipyridamole
(lifelong) |
|
Peripheral arterial disease |
Clopidogrel (lifelong) |
Asprin (lifelong) |
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:11
Atrial myxoma
Atrial myxoma is the most common primary cardiac tumour.
Overview
·
75% occur in left atrium, most commonly attached to the fossa ovalis
·
more common in females
Features
·
systemic: dyspnoea, fatigue, weight loss, pyrexia of unknown origin, clubbing
·
emboli
·
atrial fibrillation
·
mid-diastolic murmur, 'tumour plop'
·
echo: pedunculated heterogeneous mass typically attached to the fossa
ovalis region of the interatrial septum
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:11
Atrioventricular block
In atrioventricular (AV) block, or
heart block, there is impaired electrical conduction between the atria and
ventricles. There are three types:
First-degree heart block
·
PR interval > 0.2 seconds
·
asymptomatic first-degree heart block is relatively common and does not need treatment
Second-degree heart block
·
type 1 (Mobitz I, Wenckebach): progressive
prolongation of the PR interval until a dropped beat occurs
·
type 2 (Mobitz II): PR interval is constant
but the P wave is often not followed by a QRS complex
Third-degree (complete) heart block
·
there is no association between the P waves and QRS complexes
|
|
|
|
|
|
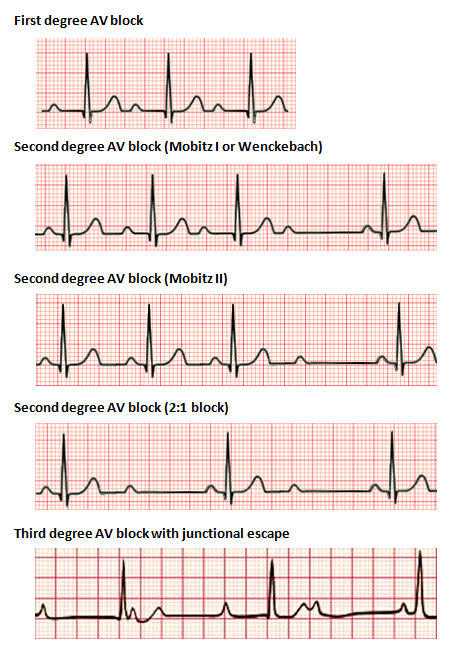
ECG showing types of heart block
|
|
|
|
|
|
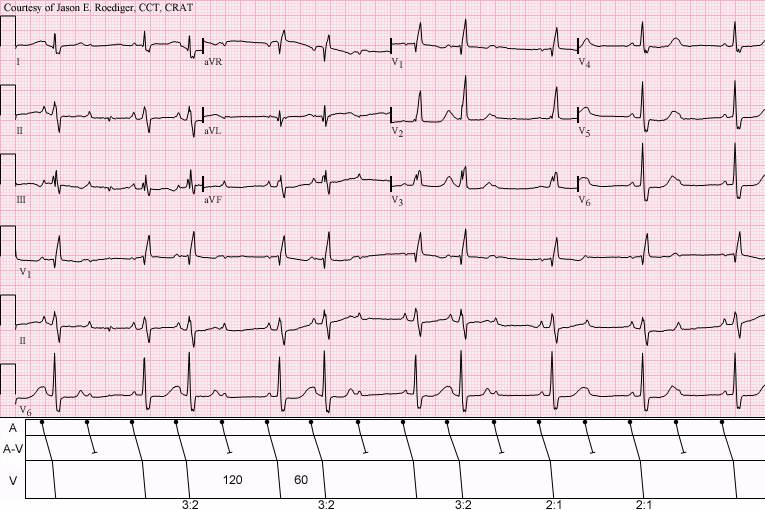
Type 1 (Wenckebach)
|
|
|
|
|
|
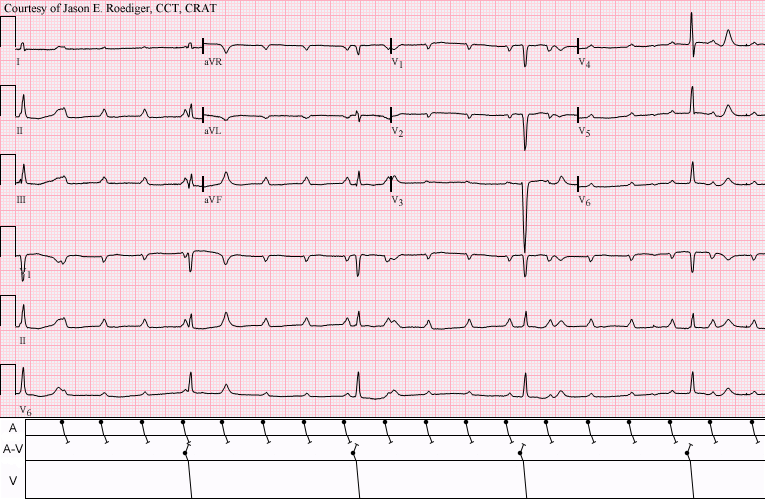
Sinus tachycardia with complete AV block and resulting
junctional escape
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:11
Cardiac imaging: non-invasive techniques excluding
echocardiography
The ability to image the heart
using non-invasive techniques such as MRI, CT and radionuclides has evolved
rapidly over recent years.
Nuclear imaging
These techniques use radiotracers
which are extracted by normal myocardium. Examples include:
·
thallium
·
technetium (99mTc) sestamibi: a coordination complex of the
radioisotope technetium-99m with the ligand methoxyisobutyl isonitrile (MIBI),
used in 'MIBI' or cardiac Single Photon Emission Computed Tomography (SPECT)
scans
·
fluorodeoxyglucose (FDG): used in Positron Emission Tomography
(PET) scans
The primary role of SPECT is to
assess myocardial perfusion and myocardial viability. Two sets of images are
usually acquired. First the myocardium at rest followed by images of the
myocardium during stress (either exercise or following adenosine /
dipyridamole). By comparing the rest with stress images any areas of ischaemia
can classified as reversible or fixed (e.g. Following a myocardial infarction).
Cardiac PET is predominately a research tool at the current time
MUGA
·
Multi Gated Acquisition Scan, also known as radionuclide
angiography
·
radionuclide (technetium-99m) is injected intravenously
·
the patient is placed under a gamma camera
·
may be performed as a stress test
·
can accurately measure left ventricular ejection fraction.
Typically used before and after cardiotoxic drugs are used
Cardiac Computed Tomography (CT)
Cardiac CT is useful for assessing
suspected ischaemic heart disease, using two main methods:
·
calcium score: there is known to be a correlation between the
amount of atherosclerotic plaque calcium and the risk of future ischaemic
events. Cardiac CT can quantify the amount of calcium producing a 'calcium
score'
·
contrast enhanced CT: allows visualisation of the coronary
artery lumen
If these two techniques are
combined cardiac CT has a very high negative predictive value for ischaemic
heart disease.
Cardiac MRI
Cardiac MRI (commonly termed CMR)
has become the gold standard for providing structural images of the heart. It
is particularly useful when assessing congenital heart disease, determining
right and left ventricular mass and differentiating forms of cardiomyopathy.
Myocardial perfusion can also be assessed following the administration of
gadolinium. Currently CMR provides limited data on the extent of coronary
artery disease.
Please also see the British Heart
Foundation link for an excellent summary.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Choking
Partial or complete airway
obstruction is a life-threatening emergency. Episodes often occur whilst eating
and patients will often clutch their neck. The first step is to ask the patient
'Are you choking?'
Features of airway obstruction
(taken from the Resus Council)
|
Mild
airway obstruction |
Severe airway obstruction |
|
Response to question 'Are you choking?' ·
victim speaks and answers yes Other signs ·
victim is able to speak, cough, and breathe |
Response to question 'Are you choking?' ·
victim unable to speak ·
victim may respond by nodding Other signs ·
victim unable to breathe ·
breathing sounds wheezy ·
attempts at coughing are silent ·
victim may be unconscious |
If mild airway obstruction
·
encourage the patient to cough
If severe airway obstruction and is
conscious:
·
give up to 5 back-blows
·
if unsuccessful give up to 5 abdominal thrusts
·
if unsuccessful continue the above cycle
If unconscious
·
call for an ambulance
·
start cardiopulmonary resuscitation (CPR)
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Combination antiplatelet and anticoagulant therapy
With the increase in comorbidity,
it is now common to find that a patient has an indication for both an
antiplatelet (e.g. established cardiovascular disease) and an anticoagulant
(e.g. atrial fibrillation, venous thromboembolism or valvular heart disease).
However, combination therapy increases the risk of bleeding and may not be
needed in all cases. How should this be managed?
Whilst there are not guidelines to
cover every scenario a recent review in the BMJ offered an expert opinion
outlining the approach in common scenarios.
Secondary prevention of stable
cardiovascular disease with an indication for an anticoagulant
·
normally in this situation, all patients are recommended to be
prescribed an antiplatelet
·
if an indication for anticoagulant exists (for example atrial
fibrillation) it is indicated that anticoagulant monotherapy is given without the addition of antiplatelets
Post-acute coronary
syndrome/percutaneous coronary intervention
·
in these patients, there is a much stronger indication for
antiplatelet therapy
·
generally patients are given triple therapy (2 antiplatelets + 1 anticoagulant) for 4 weeks-6 months after the
event and dual therapy (1 antiplatelet + 1 anticoagulant) to complete 12 months
·
there is variation from patient to patient however given that
the stroke risk in atrial fibrillation varies according to risk factors.
Venous thromboembolism (VTE)
·
if a patient on antiplatelets develops a VTE they are likely to
be prescribed anticoagulants for 3-6 months
·
a HAS-BLED score should be calculated. Those with a low risk of
bleeding may continue antiplatelets. In patients with an intermediate or high
risk of bleeding consideration should be given to stopping the antiplatelets
For more information please see BMJ
2017;358:j3782
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Dilated cardiomyopathy
Dilated cardiomyopathy (DCM) is the most common form of cardiomyopathy, accounting for 90% of cases.
Causes:
·
idiopathic: the most common cause
·
myocarditis: e.g. Coxsackie B, HIV, diphtheria, Chagas disease
·
ischaemic heart disease
·
peripartum
·
hypertension
·
iatrogenic: e.g. doxorubicin
·
substance abuse: e.g. alcohol, cocaine
·
inherited: either a familial genetic predisposition to DCM or a
specific syndrome e.g. Duchenne muscular dystrophy
o around a third of patients with DCM
are thought to have a genetic predisposition
o a large number of heterogeneous
defects have been identified
o the majority of defects are
inherited in an autosomal dominant fashion although other patterns of
inheritance are seen
·
infiltrative e.g. haemochromatosis, sarcoidosis
+ these causes may also lead to
restrictive cardiomyopathy
·
nutritional e.g. wet beriberi (thiamine deficiency)
Pathophysiology
·
dilated heart leading to predominately
systolic dysfunction
·
all 4 chambers are dilated, but the left ventricle more so than
right ventricle
·
eccentric hypertrophy (sarcomeres added in series) is seen
Features
·
classic findings of heart failure
·
systolic murmur: stretching of the valves may result in mitral
and tricuspid regurgitation
·
S3
·
'balloon' appearance of the heart on the chest x-ray
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
ECG: digoxin
ECG features
·
down-sloping ST depression ('reverse tick', 'scooped out')
·
flattened/inverted T waves
·
short QT interval
·
arrhythmias e.g. AV block, bradycardia
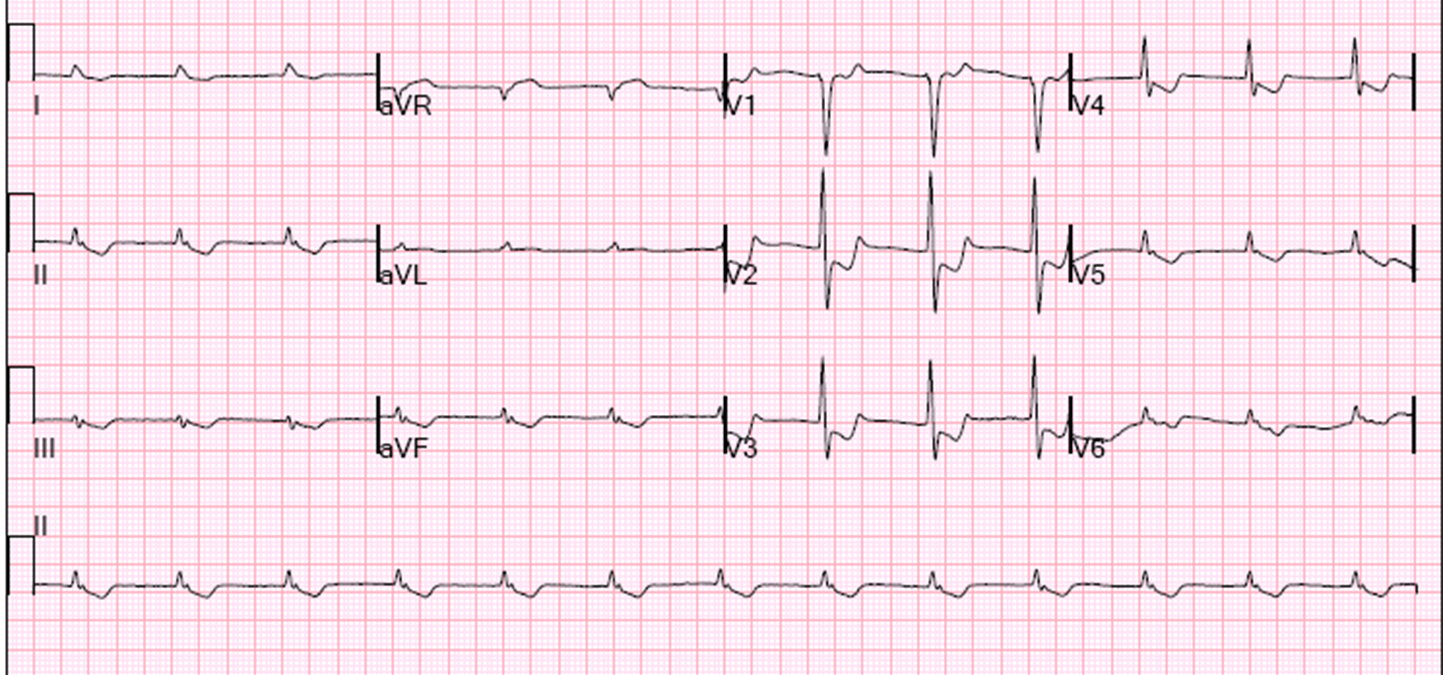
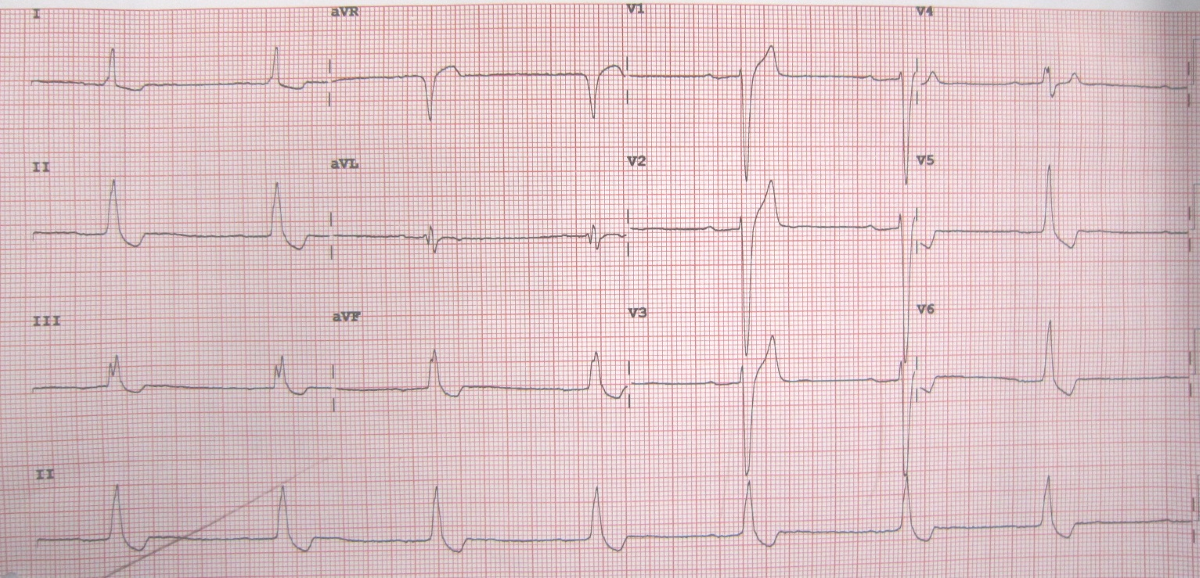
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
ECG: right bundle branch block
Right bundle branch block is a
common feature seen on ECGs.

One of the most common ways to
remember the difference between LBBB and RBBB is WiLLiaM MaRRoW
·
in LBBB there is a 'W' in V1 and a 'M' in V6
·
in RBBB there is a 'M' in V1 and a 'W' in V6
Causes of RBBB
·
normal variant - more common with increasing age
·
right ventricular hypertrophy
·
chronically increased right ventricular pressure - e.g. cor
pulmonale
·
pulmonary embolism
·
myocardial infarction
·
atrial septal defect (ostium secundum)
·
cardiomyopathy or myocarditis
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Glycoprotein IIb/IIIa receptor antagonists
Examples include;
·
abciximab
·
eptifibatide
·
tirofiban
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Heart failure (acute): features
Acute heart failure (AHF) is
life-threatening emergency. AHF is a term used to describe the sudden onset or
worsening of the symptoms of heart failure. Thus it may present with or without
a background history of pre-existing heart failure. AHF without a past history
of heart failure is called de-novo AHF. Decompensated AHF is more common
(66-75%) and presents with a background history of HF.
It usually presents after the age
of 65-years and is a major cause for unplanned hospital admission in such
patients.
AHF is usually caused by a reduced
cardiac output that results from a functional or structural abnormality.
De-novo heart failure is caused by
and increased cardiac filling pressures and myocardial dysfunction usually as a
result of ischaemia. This causes reduced cardiac output and therefore hypoperfusion. This,
in turn can cause pulmonary oedema. Other less common causes of de-novo AHF
are:
·
Viral myopathy
·
Toxins
·
Valve dysfunction
Decompensated heart failure
accounts for most cases of AHF. The most common precipitating causes of acute
AHF are:
·
Acute coronary syndrome
·
Hypertensive crisis
·
Acute arrhythmia
·
Valvular disease
There is generally a history of
pre-existing cardiomyopathy. It usually presents with signs of fluid
congestion, weight gain, orthopnoea and breathlessness.
Patient with heart failure are
broadly characterised into 1 of 4 groups based on whether they present:
·
With or without hypoperfusion
·
With or without fluid congestion
Classifying patients into one of
these 4 groups is clinically useful as it determines the therapeutic approach.
Generally speaking, the signs and
symptoms of AHF are as follows:
|
Symptoms |
Signs |
|
Breathlessness |
Cyanosis |
|
Reduced exercise tolerance |
Tachycardia |
|
Oedema |
Elevated jugular venous pressure |
|
Faitgue |
Displaced apex beat |
|
|
Chest signs: classically bibasal
crackles but may also cause a wheeze |
|
|
S3-heart sound |
Sometimes the presentation will be
that of the underlying cause (e.g: chest pain, viral infection)
Over 90% of patients with AHF have
a normal or increased blood pressure (mmHg).
The diagnostic workup for patients
with AHF includes:
·
Blood tests – this is to look for any underlying abnormality
such as anaemia, abnormal electrolytes or infection.
·
Chest X-ray – findings include pulmonary venous congestion,
interstitial oedema and cardiomegaly
·
Echocardiogram – this will identify pericardial effusion and
cardiac tamponade
·
B-type natriuretic peptide – raised levels (>100mg/litre)
indicate myocardial damage and are supportive of the diagnosis.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Heart failure (chronic): features
Features:
·
dyspnoea
·
cough: may be worse at night and associated with pink/frothy
sputum
·
orthopnoea
·
paroxysmal nocturnal dyspnoea
·
wheeze ('cardiac wheeze')
·
weight loss ('cardiac cachexia'): occurs in up to 15% of
patients. Remember this may be hidden by weight gained secondary to oedema
·
bibasal crackles on examination
·
signs of right-sided heart failure: raised JVP, ankle oedema and
hepatomegaly
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Heart sounds: S2
S2 is caused by the closure of the
aortic valve (A2) closely followed by that of the pulmonary valve (P2)
|
|
|
|
|
|

Causes of a loud S2
·
hypertension: systemic (loud A2) or pulmonary (loud P2)
·
hyperdynamic states
·
atrial septal defect without pulmonary
hypertension
Causes of a soft S2
·
aortic stenosis
Causes of fixed split S2
·
atrial septal defect
Causes of a widely split S2
·
deep inspiration
·
RBBB
·
pulmonary stenosis
·
severe mitral regurgitation
Causes of a reversed (paradoxical)
split S2 (P2 occurs before A2)
·
LBBB
·
severe aortic stenosis
·
right ventricular pacing
·
WPW type B (causes early P2)
·
patent ductus arteriosus
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:49
Hyperlipidaemia: xanthomata
Characteristic xanthomata seen in
hyperlipidaemia:
Palmar xanthoma
·
remnant hyperlipidaemia
·
may less commonly be seen in familial hypercholesterolaemia
Eruptive xanthoma are due to high
triglyceride levels and present as multiple red/yellow vesicles on the extensor
surfaces (e.g. elbows, knees)
Causes of eruptive xanthoma
·
familial hypertriglyceridaemia
·
lipoprotein lipase deficiency
Tendon xanthoma, tuberous xanthoma,
xanthelasma
·
familial hypercholesterolaemia
·
remnant hyperlipidaemia
Xanthelasma are also seen without
lipid abnormalities
Management of xanthelasma, options
include:
·
surgical excision
·
topical trichloroacetic acid
·
laser therapy
·
electrodesiccation
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Hypertension: a very basic introduction
Hypertension is one of the most
common medical conditions encountered in the developed world. Whilst there is a
degree of normal variation in blood pressure according to the time of day and
whether we are exerting ourselves hypertension describes a chronically raised
blood pressure. The main relevance of hypertension lies in the fact that it is
an important risk factor for the development of cardiovascular disease such as
ischaemic heart disease and stroke. Unless the blood pressure is very high it
is unusual for patients to experience any symptoms.
What is a 'normal' blood pressure?
Normal blood pressure can vary
widely according to age, gender and individual physiology. Most healthy people
have a blood pressure between 90/60 mmHg and 140/90 mmHg.
NICE define hypertension as
follows:
·
a clinic reading persistently above >= 140/90 mmHg, or:
·
a 24 hour blood pressure average reading >= 135/85 mmHg
Why do some patients have an
elevated blood pressure?
Patients with hypertension may be
divided into two categories. The vast majority (around 90-95%) have primary, or
essential, hypertension. This is where there is no single disease causing the
rise in blood pressure but rather a series of complex physiological changes
which occur as we get older.
Secondary hypertension may be
caused by a wide variety of endocrine, renal and other causes. The table below
lists some of the conditions that may cause secondary hypertension
|
Renal
disease |
Endocrine disorders |
Other causes |
|
• Glomerulonephritis • Chronic pyelonephritis • Adult polycystic kidney disease • Renal artery stenosis |
• Primary hyperaldosteronism • Phaeochromocytoma • Cushing's syndrome • Liddle's syndrome • Congenital adrenal hyperplasia
(11-beta hydroxylase deficiency) • Acromegaly |
• Glucocorticoids • NSAIDs • Pregnancy • Coarctation of the aorta • Combined oral contraceptive pill |
Symptoms and signs
As mentioned earlier, hypertension does not typically
cause symptoms unless it is very high, for example
> 200/120 mmHg. If very raised patients may experience:
·
headaches
·
visual disturbance
·
seizures
In terms of signs hypertension is
obviously usually detected when checking someones blood pressure. For
diagnosing longstanding blood pressure there has been a move in recent years to
using 24 hour blood pressure monitors. These avoid cases of so called 'white
coat' hypertension where a patients blood pressure rises when they are in a
clinical setting, for example a GP surgery. Studies have shown that readings
from 24 hour blood pressure monitors correlate better with clinical outcomes
and hence should be used to guide decisions about treatment.
It also also important when
assessing a patient with newly diagnosed hypertension to ensure they do not
have any end-organ damage:
·
fundoscopy: to check for hypertensive retinopathy
·
urine dipstick: to check for renal disease, either as a cause or
consequence of hypertension
·
ECG: to check for left ventricular hypertrophy or ischaemic heart
disease
Investigations
As mentioned previously 24 hour
blood pressure is now recommend for the diagnosis of hypertension. If 24 hour
blood pressure monitoring is not available then home readings using an
automated sphygmomanometer are useful.
Following diagnosis patients
typically have the following tests:
·
urea and electrolytes: check for renal disease, either as a
cause or consequence of hypertension
·
HbA1c: check for co-existing diabetes mellitus, another
important risk factor for cardiovascular disease
·
lipids: check for hyperlipidaemia, again another important risk
factor for cardiovascular disease
·
ECG
·
urine dipstick
Management
The management of patients with
hypertension involves several aspects:
·
drug therapy using antihypertensives
·
modification of other risk factors to reduce the overall risk of
cardiovascular disease
·
monitoring the patient for the development of complications of
hypertension
The table below shows the common
drugs used to treat hypertension:
|
Drug |
Mechanism of action |
Common side-effects |
Notes |
|
Angiotensin-converting enzyme (ACE)
inhibitors |
Inhibit the conversion angiotensin I to
angiotensin II |
Cough Angioedema Hyperkalaemia |
First-line treatment in younger
patients (< 55 years old) Less effective in Afro-Caribbean
patients Must be avoided in pregnant women Renal function must be check 2-3 weeks
after starting due to the risk of worsening renal function in patients with
renovascular disease Drug names end in '-pril' |
|
Calcium channel blockers |
Block voltage-gated calcium channels
relaxing vascular smooth muscle and force of myocardial contraction |
Flushing Ankle swelling Headache |
First-line treatment in older patients
(>= 55 years old) |
|
Thiazide type diuretics |
Inhibit sodium absorption at the
beginning of the distal convoluted tubule |
Hyponatraemia Hypokalaemia Dehydration |
Although technically a diuretic,
thiazides have a very weak diuretic action |
|
Angiotensin II receptor blockers (A2RB) |
Block effects of angiotensin II at the
AT1 receptor |
Hyperkalaemia |
Angiotensin II receptor blockers are
generally used in situations where patients have not tolerated an ACE
inhibitor, usually due to the development of a cough Drug names end in '-sartan' |
Drug therapy is decided by well
established NICE guidelines, which advocate a step-wise approach:
|
|
|
|
|
|
Flow chart showing the management of hypertension as per
current NICE guideliness
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Hypertension: secondary causes
It is thought that between 5-10% of
patients diagnosed with hypertension have primary hyperaldosteronism, including Conn's syndrome. This makes it the single most
common cause of secondary hypertension.
Renal disease accounts for a large
percentage of the other cases of secondary hypertension. Conditions which may
increase the blood pressure include:
·
glomerulonephritis
·
pyelonephritis
·
adult polycystic kidney disease
·
renal artery stenosis
Endocrine disorders (other than
primary hyperaldosteronism) may also result in increased blood pressure:
·
phaeochromocytoma
·
Cushing's syndrome
·
Liddle's syndrome
·
congenital adrenal hyperplasia (11-beta hydroxylase deficiency)
·
acromegaly
Drug causes:
·
steroids
·
monoamine oxidase inhibitors
·
the combined oral contraceptive pill
·
NSAIDs
·
leflunomide
Other causes include:
·
pregnancy
·
coarctation of the aorta
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Hypertrophic obstructive cardiomyopathy: management
Hypertrophic obstructive
cardiomyopathy (HOCM) is an autosomal dominant disorder of muscle tissue caused
by defects in the genes encoding contractile proteins. The estimated prevalence
is 1 in 500.
Management
·
Amiodarone
·
Beta-blockers or verapamil for symptoms
·
Cardioverter defibrillator
·
Dual chamber pacemaker
·
Endocarditis prophylaxis*
Maintain
fluid at all times
Drugs to avoid
·
nitrates
·
ACE-inhibitors
·
inotropes
*although see the 2008 NICE
guidelines on infective endocarditis prophylaxis
From <https://www.passmedicine.com/review/textbook.php?s=#>
MR SAM ASH
insertion
of an implantable cardioverter defibrillator to lower the risk of sudden
cardiac death
From <https://mle.ncl.ac.uk/cases/page/18128/>
HOCM is the most common cause of
sudden cardiac death in young people.
Surgery:
Surgical myectomy
Alcohol septal ablation
24 December 2020
13:50
Infective endocarditis: prognosis and management
Poor prognostic factors
·
Staphylococcus aureus infection (see below)
·
prosthetic valve (especially 'early', acquired during surgery)
·
culture negative endocarditis
·
low complement levels
Mortality according to organism
·
staphylococci - 30%
·
bowel organisms - 15%
·
streptococci - 5%
Current antibiotic guidelines
(source: British National Formulary)
|
Scenario |
Suggested antibiotic therapy |
|
Initial blind therapy |
Native valve ·
amoxicillin, consider adding low-dose gentamicin If penicillin allergic, MRSA or severe
sepsis ·
vancomycin + low-dose gentamicin If prosthetic valve ·
vancomycin + rifampicin + low-dose gentamicin |
|
Native valve endocarditis caused by
staphylococci |
Flucloxacillin If penicillin allergic or MRSA ·
vancomycin + rifampicin |
|
Prosthetic valve endocarditis caused by
staphylococci |
Flucloxacillin + rifampicin + low-dose
gentamicin If penicillin allergic or MRSA ·
vancomycin + rifampicin + low-dose gentamicin |
|
Endocarditis caused by fully-sensitive
streptococci (e.g. viridans) |
Benzylpenicillin If penicillin allergic ·
vancomycin + low-dose gentamicin |
|
Endocarditis caused by less sensitive
streptococci |
Benzylpenicillin + low-dose gentamicin If penicillin allergic ·
vancomycin + low-dose gentamicin |
Indications for surgery
·
severe valvular incompetence
·
aortic abscess (often indicated by a lengthening PR interval)
·
infections resistant to antibiotics/fungal infections
·
cardiac failure refractory to standard medical treatment
·
recurrent emboli after antibiotic therapy
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Inhaled foreign body
This typically occurs in younger
children. Whilst the presentation if often acute it can sometimes go unnoticed,
with up to a third of cases being diagnosed after a few days.
Features
·
cough
·
stridor
·
dyspnoea
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Investigating palpitations
Palpitations are a common
presenting symptom.
Possible causes include
·
arrhythmias
·
stress
·
increased awareness of normal heart beat / extrasystoles
First-line investigations include:
·
12-lead ECG: this will only capture the heart rhythm for a few
seconds and hence is likely to miss episodic arrhythmias. However, other
abnormalities linked to the underlying arrhythmia (for example a prolonged QT
interval or PR interval, or changes suggesting recent myocardial ischaemia) may
be seen.
·
thyroid function tests: thyrotoxicosis may precipitate atrial
fibrillation and other arrhythmias
·
urea and electrolytes: looking for disturbances such as a low
potassium
·
full blood count
Capturing episodic arrhythmias
First-line investigations are often
normal in patients complaining of palpitations. The next step is to exclude an
episode arrhythmia.
The most common investigation is
Holter monitoring
·
portable battery operated device
·
continuously records ECG from 2-3 leads
·
usually done for 24 hours but may be used for longer if symptoms
are less than daily
·
patients are asked to keep a diary to record any symptomatic
palpitations. This can later be compared to the rhythm strip at the time of the
symptoms
·
at the end of the monitoring a report is generated summarising a
number of parameters including heart rate, arrhythmias and changes in ECG
waveform
If no abnormality is found on the
Holter monitor, and symptoms continue, other options include:
·
external loop recorder
·
implantable loop recorder
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Isolated systolic hypertension
Isolated systolic hypertension
(ISH) is common in the elderly, affecting around 50% of people older than 70
years old. The Systolic Hypertension in the Elderly Program (SHEP) back in 1991
established that treating ISH reduced both strokes and ischaemic heart disease.
Drugs such as thiazides were recommended as first line agents. This approach is
contradicated by the 2011 NICE guidelines which recommends treating ISH in the
same stepwise fashion as standard hypertension.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Ivabradine
Ivabradine is a class of
anti-anginal drug which works by reducing the heart rate. It acts on the If ('funny') ion current which is highly expressed in the sinoatrial node, reducing
cardiac pacemaker activity.
Adverse effects
·
visual effects, particular luminous
phenomena, are common
·
headache
·
bradycardia, heart block
There is no evidence currently of
superiority over existing treatments of stable angina.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Mitral regurgitation
Also known as mitral insufficiency,
mitral regurgitation (MR) occurs when blood leaks back through the mitral valve
on systole. It is the second most common valve disease after aortic stenosis.
The mitral valve is located between the left atrium and ventricle, and
regurgitation leads to a less efficient heart as less blood is pumped through
the body with each contraction. This said, MR is common in otherwise healthy
patients to a trivial degree and does not need treatment.
As the degree of regurgitation
becomes more severe, the body’s oxygen demands may exceed what the heart can
supply and as a result, the myocardium can thicken over time. While this may be
benign initially, patients may find themselves increasingly fatigued as a
thicker myometrium becomes less efficient, and eventually go into irreversible
heart failure.
Risk factors
·
Female sex
·
Lower body mass
·
Age
·
Renal dysfunction
·
Prior myocardial infarction
·
Prior mitral stenosis or valve prolapse
·
Collagen disorders e.g. Marfan's Syndrome and
Ehlers-Danlos syndrome
Causes
·
Following coronary artery disease or post-MI: if the papillary
muscles or chordae tendinae are affected by a cardiac insult, mitral valve
disease may ensue as a result of damage to its supporting structures.
·
Mitral valve prolapse: Occurs when the leaflets of the mitral
valve is deformed so the valve does not close properly and allows for backflow.
Most patients with this have a trivial degree of mitral regurgitation.
·
Infective endocarditis: When vegetations from the organisms
colonising the heart grow on the mitral valve, it is prevented from closing
properly. Patients with abnormal valves are more likely to develop endocarditis
as opposed to their peers.
·
Rheumatic fever: While this is uncommon in developed countries,
rheumatic fever can cause inflammation of the valves and therefore result in
mitral regurgitation.
·
Congenital
Symptoms
·
Most patients with MR are asymptomatic, and patients suffering
from mild to moderate MR may stay largely asymptomatic indefinitely. Symptoms
tend to be due to failure of the left ventricle, arrhythmias or pulmonary
hypertension. This may present as fatigue, shortness of breath and oedema.
Signs
·
The murmur heard on auscultation of the chest is typically a
pansystolic murmur described as “blowing”. It is heard best at the apex and
radiating into the axilla. S1 may be quiet as a result of incomplete closure of
the valve. Severe MR may cause a widely split S2
Investigations
·
ECG may show a broad P wave, indicative of atrial enlargement
·
Cardiomegaly may be seen on chest x-ray, with an enlarged left
atrium and ventricle
·
Echocardiography is crucial to diagnosis and to assess severity
Treatment options
·
Medical management in acute cases involves nitrates, diuretics,
positive inotropes and an intra-aortic balloon pump to increase cardiac output
·
If patients are in heart failure, ACE inhibitors may be
considered along with beta-blockers and spironolactone
·
In acute, severe regurgitation, surgery is indicated
·
The evidence for repair over replacement is strong in
degenerative regurgitation, and is demonstrated through lower mortality and
higher survival rates
·
When this is not possible, valve replacement with either an
artificial valve or a pig valve is considered
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Mitral valve prolapse
Mitral valve prolapse is common,
occurring in around 5-10 % of the population. It is usually idiopathic but may
be associated with a wide variety of cardiovascular disease and other
conditions
Associations
·
congenital heart disease: PDA, ASD
·
cardiomyopathy
·
Turner's syndrome
·
Marfan's syndrome, Fragile X
·
osteogenesis imperfecta
·
pseudoxanthoma elasticum
·
Wolff-Parkinson White syndrome
·
long-QT syndrome
·
Ehlers-Danlos Syndrome
·
polycystic kidney disease
Features
·
patients may complain of atypical chest pain or palpitations
·
mid-systolic click (occurs later if patient squatting)
·
late systolic murmur (longer if patient standing)
·
complications: mitral regurgitation, arrhythmias (including long
QT), emboli, sudden death
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:50
Myocarditis
Myocarditis describes inflammation
of the myocardium. There are a wide range of underlying causes. It should be
particularly considered in younger patients who present with chest pain.
Causes
·
viral: coxsackie B, HIV
·
bacteria: diphtheria, clostridia
·
spirochaetes: Lyme disease
·
protozoa: Chagas' disease, toxoplasmosis
·
autoimmune
·
drugs: doxorubicin
Presentation
·
usually young patient with an acute history
·
chest pain
·
dyspnoea
·
arrhythmias
Investigations
·
bloods
o ↑ inflammatory markers in 99%
o ↑ cardiac enzymes
o ↑ BNP
·
ECG
o tachycardia
o arrhythmias
o ST/T wave changes including
ST-segment elevation and T wave inversion
Management
·
treatment of underlying cause e.g. antibiotics if bacterial
cause
·
supportive treatment e.g. of heart failure or arrhythmias
Complications
·
heart failure
·
arrhythmia, possibly leading to sudden death
·
dilated cardiomyopathy: usually a late complication
From <https://www.passmedicine.com/review/textbook.php?s=#>
Cyclophosphamide
is known to be associated with haemorrhagic myocarditis
From <https://mle.ncl.ac.uk/cases/page/18128/>
24 December 2020
13:51
Nitrates
Nitrates are a group of drugs which
have vasodilating effects. The main indications for their use is in the
management of angina and the acute treatment of heart failure. Sublingual
glyceryl trinitrate is the most common drug used in patients with ischaemic
heart disease to relieve angina attacks.
Mechanism of action
·
nitrates cause the release of nitric oxide in smooth muscle,
activating guanylate cyclase which then converts GTP to cGMP, which in turn
leads to a fall in intracellular calcium
levels
·
in angina they both dilate the coronary arteries and also reduce
venous return which in turn reduces left ventricular work, reducing myocardial
oxygen demand
Side-effects
·
hypotension
·
tachycardia
·
headaches
·
flushing
Nitrate tolerance
·
many patients who take nitrates develop tolerance and experience
reduced efficacy
·
the BNF advises that patients who develop tolerance should take
the second dose of isosorbide mononitrate after 8 hours, rather than after 12
hours. This allows blood-nitrate levels to fall for 4 hours and maintains
effectiveness
·
this effect is not seen in patients who take modified release
isosorbide mononitrate
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Orthostatic hypotension
Orthostatic hypotension is more
common in older people and patients who have neurodegenerative disease (e.g.
Parkinson's) diabetes, or hypertension
Iatrogenic causes include alpha-blockers (e.g. for benign prostatic hyperplasia).
Features
·
a drop in BP (usually >20/10 mm Hg) within three minutes of
standing
·
presyncope
·
syncope
Management
·
treatment options include midodrine
and fludrocortisone
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Parenteral anticoagulation
Parenteral anticoagulants are used
for the prevention of venous thromboembolism and in the management of acute
coronary syndrome.
Unfractionated heparin and low molecular weight heparin are discussed in detail so this note will focus on fondaparinux
and direct thrombin inhibitors.
Fondaparinux
Activates antithrombin III, which
in turn potentiates the inhibition of coagulation factors Xa. It is given
subcutaneously.
Direct thrombin inhibitors
Examples include bivalirudin. These
are generally given intravenously.
Dabigatran is a type of direct
thrombin inhibitor that is taken orally. It is often grouped alongside the
direct oral anticoagulants (DOACs).
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Pulmonary artery occlusion pressure monitoring
The pulmonary artery occlusion
pressure is an indirect measure of left atrial pressure, and thus filling
pressure of the left heart. The low resistance within the pulmonary venous
system allows this useful measurement to be made. The most accurate trace is
made by inflating the balloon at the catheter tip and 'floating' it so that it
occludes the vessel. If it is not possible to occlude the vessel in this way
then the measurement gained will be the pulmonary artery end diastolic
pressure.
Interpretation of PAOP
|
PAOP |
mmHg |
Scenario |
|
Normal |
8-12 |
|
|
Low |
<5 |
Hypovolaemia |
|
Low
with pulmonary oedema |
<5 |
ARDS |
|
High |
>18 |
Overload |
When combined with measurements of
systemic vascular resistance and cardiac output it is possible to accurately
classify patients.
Systemic vascular resistance
Derived from aortic pressure, right
atrial pressure and cardiac output.
SVR=80(mean aortic pressure-mean
right atrial pressure)/cardiac output
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Saphenous vein
Long saphenous vein
This vein may be harvested for
bypass surgery, or removed as treatment for varicose veins with saphenofemoral
junction incompetence.
·
Originates at the 1st digit where the dorsal vein merges with
the dorsal venous arch of the foot
·
Passes anterior to the medial malleolus and runs up the medial side of the
leg
·
At the knee, it runs over the posterior border of the medial
epicondyle of the femur bone
·
Then passes laterally to lie on the anterior surface of the
thigh before entering an opening in the fascia lata called the saphenous
opening
·
It joins with the femoral vein in the region of the femoral
triangle at the saphenofemoral junction
Tributaries
·
Medial marginal
·
Superficial epigastric
·
Superficial iliac circumflex
·
Superficial external pudendal veins
Short saphenous vein
·
Originates at the 5th digit where the dorsal vein merges with
the dorsal venous arch of the foot, which attaches to the great saphenous vein.
·
It passes around the lateral aspect of the foot (inferior and posterior to the lateral malleolus) and runs along the posterior aspect of the leg (with
the sural nerve)
·
Passes between the heads of the gastrocnemius muscle, and drains
into the popliteal vein, approximately at or above the level of the knee joint.
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Subclavian artery
Path
·
The left subclavian comes directly off the arch of aorta
·
The right subclavian arises from the brachiocephalic artery
(trunk) when it bifurcates into the subclavian and the right common carotid
artery.
·
From its origin, the subclavian artery travels laterally,
passing between anterior and middle scalene muscles, deep to scalenus anterior
and anterior to scalenus medius. As the subclavian artery crosses the lateral
border of the first rib, it becomes the axillary artery. At this point it is
superficial and within the subclavian triangle.
|
|
|
|
Image
sourced from Wikipedia |
|
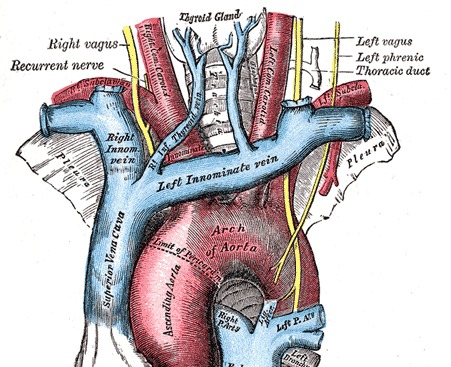
Branches
·
Vertebral artery
·
Internal thoracic artery
·
Thyrocervical trunk
·
Costocervical trunk
·
Dorsal scapular artery
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Takotsubo cardiomyopathy
Takotsubo cardiomyopathy is a type
of non-ischaemic cardiomyopathy associated with a transient, apical ballooning of the
myocardium. It may be triggered by stress.
Pathophysiology
·
Takotsubo is a Japanese word that describes an octopus trap
·
the apical ballooning appearance occurs due to severe
hypokinesis of the mid and apical segments with preservation of activity of the
basal segments. In simple terms, the bottom of the heart (the apex) does not
contract and therefore appears to balloon out. However, the area closer to the
top (the base) continues to contract (creating the neck of the octopus trap)
Features
·
chest pain
·
features of heart failure
·
ECG: ST-elevation
·
normal coronary angiogram
Treatment is supportive.
Prognosis
·
the majority of patients improve with supportive treatment
From <https://www.passmedicine.com/review/textbook.php?s=#>
24 December 2020
13:51
Travel-related thrombosis
It is not uncommon for us to be
asked by patients whether they should take aspirin prior to a long haul flight.
So called 'economy class syndrome' as a concept has increased in the public's
mind over the past 10 years or so. It is certainly true that long-haul air
travel is associated with an increased risk of VTE. A 2001 study in the New
England Journal of Medicine1 showed the following risk of pulmonary embolism:
·
0.01 cases per million for travel under 5,000 km
·
1.5 cases per million for travel between 5,000 - 10,000 km
·
4.8 cases per million for travel over 10,000 km
The Civil Aviation Authority do not
give specific guidance relating to venous thromboembolism. The British
Committee for Standards in Haematology did however produce guidelines in 2005
as did SIGN in 2010 and Clinical Knowledge Summaries (CKS) in 2013.
Unfortunately, there is no universal agreement on what to advise patients.
The most recent CKS guidelines
advise that we take a risk based approach. For example, a patient with no major
risk factors for VTE (i.e. the average person) then no special measures are
needed.
Patients with major risk factors
should consider wearing anti-embolism stockings. These can either be bought by
the patient or prescribed (class I). Clearly if the risk is very high (e.g. a
long-haul flight following recent major surgery) then consideration should be
given to delaying the flight or specialist advice sought regarding the use of
low-molecular weight heparin.
All guidelines agree there is no
role for aspirin in low, medium or high risk patients.
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
16:11
Hypertension: management
NICE published updated guidelines
for the management of hypertension in 2019. Some of the key changes include:
·
lowering the threshold for treating stage 1 hypertension in
patients < 80 years from 20% to 10%
·
angiotensin receptor blockers can be used instead of
ACE-inhibitors where indicated
·
if a patient is already taking an ACE-inhibitor or angiotensin
receptor blocker, then a calcium channel blocker OR a thiazide-like diuretic
can be used. Previously only a calcium channel blocker was recommended
Blood pressure classification
This becomes relevant later in some
of the management decisions that NICE advocate.
|
Stage |
Criteria |
|
Stage 1 hypertension |
Clinic BP >= 140/90 mmHg and subsequent ABPM daytime average or HBPM average
BP >= 135/85
mmHg |
|
Stage 2 hypertension |
Clinic BP >= 160/100 mmHg and subsequent ABPM daytime average or HBPM average
BP >= 150/95
mmHg |
|
Severe hypertension |
Clinic systolic BP >= 180 mmHg, or
clinic diastolic BP >= 110 mmHg |
|
|
|
|
|
|

Flow chart showing simplified schematic for diagnosis
hypertension following NICE guidelines
Managing hypertension
Lifestyle advice should not be
forgotten and is frequently tested in exams:
·
a low salt diet is recommended, aiming for less than 6g/day, ideally
3g/day. The average adult in the UK consumes around 8-12g/day of salt. A recent
BMJ paper* showed that lowering salt intake can have a significant effect on
blood pressure. For example, reducing salt intake by 6g/day can lower systolic
blood pressure by 10mmHg
·
caffeine intake should be reduced
·
the other general bits of advice remain: stop smoking, drink
less alcohol, eat a balanced diet rich in fruit and vegetables, exercise more,
lose weight
ABPM/HBPM >= 135/85 mmHg (i.e. stage 1 hypertension)
·
treat if < 80 years of age AND any of the following apply;
target organ damage, established cardiovascular disease, renal disease,
diabetes or a 10-year cardiovascular risk equivalent to 10% or greater
·
in 2019, NICE made a further recommendation, suggesting that we
should 'consider antihypertensive drug
treatment in addition to lifestyle advice for adults aged under 60 with stage 1
hypertension and an estimated 10-year risk below 10%. '. This seems to be due to evidence
that QRISK may underestimate the lifetime probability of developing
cardiovascular disease
ABPM/HBPM >= 150/95 mmHg (i.e. stage 2 hypertension)
·
offer drug treatment regardless of age
For patients < 40 years consider
specialist referral to exclude secondary causes.
|
|
|
|
|
|
Flow chart showing the management of hypertension as per
current NICE guideliness
Step 1 treatment
·
patients < 55-years-old or a background of type 2 diabetes mellitus: ACE inhibitor or a Angiotensin receptor blocker (ACE-i or ARB): (A)
o angiotensin
receptor blockers should be used where ACE inhibitors are not tolerated (e.g.
due to a cough)
·
patients >= 55-years-old or of black
African or African–Caribbean origin: Calcium channel blocker (C)
o ACE inhibitors have reduced
efficacy in patients of black African or African–Caribbean origin are therefore
not used first-line
Step 2 treatment
·
if already taking an ACE-i or ARB add a Calcium channel blocker or a thiazide-like Diuretic
·
if already taking a Calcium channel blocker add an ACE-i or ARB
o for patients of black African or
African–Caribbean origin taking a calcium channel blocker for hypertension, if
they require a second agent consider an angiotensin receptor blocker in
preference to an ACE inhibitor
·
(A + C) or (A + D)
Step 3 treatment
·
add a third drug to make, i.e.:
o if already taking an (A + C) then add a D
o if already (A
+ D) then add a C
·
(A + C + D)
Step 4 treatment
·
NICE define step 4 as resistant hypertension and suggest either
adding a 4th drug (as below) or seeking
specialist advice
·
first, check for:
o confirm elevated clinic BP with
ABPM or HBPM
o assess for postural hypotension.
o discuss adherence
·
if potassium < 4.5 mmol/l add low-dose
spironolactone
·
if potassium > 4.5 mmol/l add an alpha- or
beta-blocker
Patients who fail to respond to
step 4 measures should be referred to a specialist. NICE recommend:
If blood pressure remains uncontrolled with the optimal
or maximum tolerated doses of four drugs, seek expert advice if it has not yet
been obtained.
Blood pressure targets
|
|
Clinic BP |
ABPM / HBPM |
|
Age < 80 years |
140/90 mmHg |
135/85 mmHg |
|
Age > 80 years |
150/90 mmHg |
145/85 mmHg |
New drugs
Direct renin inhibitors
·
e.g. Aliskiren (branded as Rasilez)
·
by inhibiting renin blocks the conversion of angiotensinogen to
angiotensin I
·
no trials have looked at mortality data yet. Trials have only
investigated fall in blood pressure. Initial trials suggest aliskiren reduces
blood pressure to a similar extent as angiotensin converting enzyme (ACE)
inhibitors or angiotensin-II receptor antagonists
·
adverse effects were uncommon in trials although diarrhoea was
occasionally seen
·
only current role would seem to be in patients who are
intolerant of more established antihypertensive drugs
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:47
Heart failure: drug management
NICE issued updated guidelines on
management in 2018, key points are summarised here
Whilst loop diuretics play an
important role in managing fluid overload it should be remembered that no
long-term reduction in mortality has been demonstrated for loop diuretics such as
furosemide.
The first-line treatment for all
patients is both an ACE-inhibitor and
a beta-blocker
·
generally, one drug should be started at a
time. NICE advise
that clinical judgement is used when determining which one to start first
·
beta-blockers licensed to treat heart failure in the UK include bisoprolol, carvedilol, and nebivolol.
·
ACE-inhibitors and beta-blockers have no effect on mortality in
heart failure with preserved ejection fraction
Second-line treatment is an aldosterone antagonist
·
these are sometimes referred to as mineralocorticoid receptor
antagonists. Examples include spironolactone and eplerenone
·
it should be remember that both ACE inhibitors (which the
patient is likely to already be on) and aldosterone antagonists both cause
hyperkalaemia - therefore potassium should be monitored
Third-line treatment should be
initiated by a specialist. Options include ivabradine, sacubitril-valsartan,
hydralazine in combination with nitrate, digoxin and cardiac resynchronisation
therapy
·
ivabradine
o criteria: sinus
rhythm > 75/min and a left ventricular fraction < 35%
·
sacubitril-valsartan
o criteria: left ventricular fraction
< 35%
o is considered in heart failure with
reduced ejection fraction who are symptomatic on ACE inhibitors or ARBs
o should be initiated following ACEi
or ARB wash-out period
·
digoxin
o digoxin has also not been proven to
reduce mortality in patients with heart failure. It may however improve
symptoms due to its inotropic properties
o it is strongly indicated if there
is coexistent atrial fibrillation
·
hydralazine in combination with nitrate
o this may be particularly indicated
in Afro-Caribbean patients
·
cardiac resynchronisation therapy
o indications include a widened QRS (e.g. left bundle branch block) complex on ECG
Other treatments
·
offer annual influenza vaccine
·
offer one-off pneumococcal vaccine
o adults usually require just one
dose but those with asplenia, splenic dysfunction or chronic kidney disease
need a booster every 5 years
From <https://www.passmedicine.com/review/textbook.php?s=#>
In
acute decompensated heart failure, the negative inotropic effects of beta
blockers can worsen stroke volume and therefore aggravate heart failure.
Chronic
beta-blocker use in stable heart failure is associated with significantly
improved survival in patients but should be deferred until patient is no
longer congested after treatment with appropriate diuresis and post-load
reduction.
From <https://mle.ncl.ac.uk/cases/page/18128/>
Haemodynamic
profile is that of wet decompensated heart failure. Intravenous loop diuretic
is more effective than oral diuretic in clearing the congestion.
Beta-blocker
is not advisable in patients with acute decompensated heart failure.
From <https://mle.ncl.ac.uk/cases/page/18128/>
N-type
pro B-type natriuretic peptide
·
>2000ng/L refer for
specialist assessment urgently, transthoracic echo within 2 weeks
·
400-2000ng/L refer for
specialist assessment within 6 weeks
·
<400ng/L, diagnosis
of heart failure less likely
Reduced
levels in obese, African-Caribbean, patients on diuretics, ACEi, beta-blockers
Need to
rule out other causes (>70 years old, LVH, ischaemia, pulmonary embolism) in
patients with high natriuretic peptide levels
From <https://mle.ncl.ac.uk/cases/page/17993/>
21 December 2020
22:11
Statins
Statins inhibit the action of HMG-CoA
reductase, the rate-limiting enzyme in hepatic cholesterol synthesis.
Adverse effects
·
myopathy: includes myalgia, myositis, rhabdomyolysis and
asymptomatic raised creatine kinase. Risks factors for myopathy include
advanced age, female sex, low body mass index and presence of multisystem
disease such as diabetes mellitus. Myopathy is more common in lipophilic statins
(simvastatin, atorvastatin) than relatively hydrophilic statins (rosuvastatin,
pravastatin, fluvastatin)
·
liver impairment: the 2014 NICE guidelines recommend checking
LFTs at baseline, 3 months and 12 months. Treatment should be discontinued if
serum transaminase concentrations rise to and persist at 3 times the upper
limit of the reference range
·
there is some evidence that statins may increase the risk of
intracerebral haemorrhage in patients who've previously had a stroke. This
effect is not seen in primary prevention. For this reason the Royal College of
Physicians recommend avoiding statins in patients with a history of
intracerebral haemorrhage
Contraindications
·
macrolides (e.g. erythromycin,
clarithromycin) are an important interaction. Statins should be stopped until
patients complete the course
·
pregnancy
Who should receive a statin?
·
all people with established cardiovascular disease (stroke, TIA,
ischaemic heart disease, peripheral arterial disease)
·
following the 2014 update, NICE
recommend anyone with a 10-year cardiovascular risk >= 10%
·
patients with type 2 diabetes mellitus should now be assessed
using QRISK2 like other patients are, to determine whether they should be
started on statins
·
patients with type 1 diabetes mellitus who were diagnosed more
than 10 years ago OR are aged over 40 OR have established nephropathy
Statins should be taken at night as
this is when the majority of cholesterol synthesis takes place. This is
especially true for simvastatin which has a shorter half-life than other statins.
NICE currently recommends the
following for the prevention of cardiovascular disease::
·
atorvastatin 20mg for primary prevention
o increase the dose if non-HDL has
not reduced for >= 40%
·
atorvastatin 80mg for secondary prevention
|
|
|
|
|
|
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:54
Warfarin: management of high INR
The following is based on the BNF
guidelines, which in turn take into account the British Committee for Standards
in Haematology (BCSH) guidelines.
|
Situation |
Management |
|
Major bleeding |
Stop warfarin Give intravenous vitamin K 5mg Prothrombin complex concentrate - if
not available then FFP* |
|
INR > 8.0 Minor bleeding |
Stop warfarin Give intravenous vitamin K 1-3mg Repeat dose of vitamin K if INR still
too high after 24 hours Restart warfarin when INR < 5.0 |
|
INR > 8.0 No bleeding |
Stop warfarin Give vitamin K 1-5mg by mouth, using
the intravenous preparation orally Repeat dose of vitamin K if INR still
too high after 24 hours Restart when INR < 5.0 |
|
INR 5.0-8.0 Minor bleeding |
Stop warfarin Give intravenous vitamin K 1-3mg Restart when INR < 5.0 |
|
INR 5.0-8.0 No bleeding |
Withhold 1 or 2 doses of warfarin Reduce subsequent maintenance dose |
*as FFP can take time to defrost
prothrombin complex concentrate should be considered in cases of intracranial
haemorrhage
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
17:56
ECG: coronary territories
The table below shows the
correlation between ECG changes and coronary territories:
|
|
ECG changes |
Coronary artery |
|
Anteroseptal |
V1-V4 |
Left anterior descending |
|
Inferior |
II, III, aVF |
Right coronary |
|
Anterolateral |
V4-6, I, aVL |
Left anterior descending or left
circumflex |
|
Lateral |
I, aVL +/- V5-6 |
Left circumflex |
|
Posterior |
Tall R waves V1-2 |
Usually left circumflex, also right
coronary |
It should be remembered that a new left bundle
branch block (LBBB) may point towards a diagnosis of acute coronary syndrome.
|
|
|
|
|
|
Diagram showing the correlation between ECG changes and
coronary territories in acute coronary syndrome
Next question
Save my notes
Search
Go
Google search
on "ECG: coronary territories"
Links
|
University
of Massachusetts Medical School |
21 |
|
|
|
Postgraduate
Medical Journal |
32 |
|
|
Suggest linkReport broken link
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:54
Atrial fibrillation: rate control and maintenance of sinus
rhythm
The Royal College of Physicians and
NICE published guidelines on the management of atrial fibrillation (AF) in
2006. The following is also based on the joint American Heart Association
(AHA), American College of Cardiology (ACC) and European Society of Cardiology
(ESC) 2012 guidelines
Medication
Agents used to control rate in
patients with atrial fibrillation
·
beta-blockers
o a common contraindication for
beta-blockers is asthma
·
calcium channel blockers
·
digoxin
o not considered first-line anymore
as they are less effective at controlling the heart rate during exercise
o however, they are the preferred
choice if the patient has coexistent heart failure
Agents used to maintain sinus
rhythm in patients with a history of atrial fibrillation
·
sotalol
·
amiodarone
·
flecainide
·
others (less commonly used in UK): disopyramide, dofetilide,
procainamide, propafenone, quinidine
The table below indicates some of
the factors which may be considered when considering either a rate control or
rhythm control strategy
|
Factors
favouring rate control |
Factors favouring rhythm control |
|
Older than 65 years History of ischaemic heart disease |
Younger than 65 years Symptomatic First presentation Lone AF or AF secondary to a corrected
precipitant (e.g. Alcohol) Congestive heart failure |
Catheter ablation
NICE recommends the use of catheter
ablation for those with AF who have not responded to or wish to avoid,
antiarrhythmic medication.
Technical aspects
·
the aim is to ablate the faulty electrical pathways that are
resulting in atrial fibrillation. This is typically due to aberrant electrical activity between the pulmonary veins and left
atrium
·
the procedure is performed percutaneously, typically via the
groin
·
both radiofrequency (uses heat generated from medium frequency
alternating current) and cryotherapy can be used to ablate the tissue
Anticoagulation
·
should be used 4 weeks before and during the procedure
·
it should be remember that catheter ablation controls the rhythm
but does not reduce the stroke risk, even if patients remain in sinus rhythm.
Therefore, patients still require anticoagulation as per there CHA2DS2-VASc score
o if score = 0: 2 months
anticoagulation recommended
o if score > 1: longterm
anticoagulation recommended
Outcome
·
notable complications include
o cardiac tamponade
o stroke
o pulmonary valve stenosis
·
success rate
o around 50% of patients experience
an early recurrence (within 3 months) of AF that often resolves spontaneously
o longer term, after 3 years, around
55% of patients who've had a single procedure remain in sinus rhythm. Of
patient who've undergone multiple procedures around 80% are in sinus rhythm
From <https://www.passmedicine.com/question/questions.php?q=0>
Wednesday, 23 December 2020
01:07
ACE inhibitors
Angiotensin-converting enzyme (ACE)
inhibitors are now the established first-line treatment in younger patients
with hypertension and are also extensively used to treat heart failure. They
are known to be less effective in treating hypertensive Afro-Caribbean
patients. ACE inhibitors are also used to treat diabetic nephropathy and have a
role in the secondary prevention of ischaemic heart disease.
Mechanism of action:
·
inhibit the conversion angiotensin I to angiotensin II
·
ACE inhibitors are activated by phase 1 metabolism in the
liver
Side-effects:
·
cough
o occurs in around 15% of patients
and may occur up to a year after starting treatment
o thought to be due to increased
bradykinin levels
·
angioedema: may occur up to a year after starting treatment
·
hyperkalaemia
·
first-dose hypotension: more common in patients taking diuretics
Cautions and contraindications
·
pregnancy and breastfeeding - avoid
·
renovascular disease - may result in renal impairment
·
aortic stenosis - may result in hypotension
·
hereditary of idiopathic angioedema
·
specialist advice should be sought before starting ACE
inhibitors in patients with a potassium >= 5.0 mmol/L
Interactions
·
patients receiving high-dose diuretic therapy (more than 80 mg
of furosemide a day)
o significantly increases the risk of
hypotension
Monitoring
·
urea and electrolytes should be checked before treatment is
initiated and after increasing the dose
o a rise in the creatinine and
potassium may be expected after starting ACE inhibitors
o acceptable changes
are an increase in serum creatinine, up to 30% from baseline and an increase in potassium
up to 5.5 mmol/l.
o significant renal impairment may
occur in patients who have undiagnosed bilateral renal artery stenosis
|
|
|
|
|
|
Flow chart showing the management of hypertension as per
current NICE guideliness
22 December 2020
16:57
Hypertension: diagnosis
NICE published updated guidelines
for the management of hypertension in 2019. This builds on the significant
guidelines released in 2011 that recommended:
·
classifying hypertension into stages
·
recommending the use of ambulatory blood pressure
monitoring (ABPM) and home blood pressure monitoring (HBPM)
|
|
|
|
|
|
Flow chart showing simplified schematic for diagnosis
hypertension following NICE guidelines
Why were these guidelines needed?
It has long been recognised by
doctors that there is a subgroup of patients whose blood pressure climbs 20
mmHg whenever they enter a clinical setting, so called 'white coat
hypertension'. If we just rely on clinic readings then such patients may be
diagnosed as having hypertension when, the vast majority of the time, their
blood pressure is normal.
This has led to the use of both
ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring
(HBPM) to confirm the diagnosis of hypertension. These techniques allow a more
accurate assessment of a patients' overall blood pressure. Not only does this
help prevent overdiagnosis of hypertension - ABPM has been shown to be a more
accurate predictor of cardiovascular events than clinic readings.
Blood pressure classification
This becomes relevant later in some
of the management decisions that NICE advocate.
|
Stage |
Criteria |
|
Stage 1 hypertension |
Clinic BP >= 140/90 mmHg and
subsequent ABPM daytime average or HBPM average BP >= 135/85 mmHg |
|
Stage 2 hypertension |
Clinic BP >= 160/100 mmHg and
subsequent ABPM daytime average or HBPM average BP >= 150/95 mmHg |
|
Severe hypertension |
Clinic systolic BP >= 180 mmHg, or
clinic diastolic BP >= 120 mmHg |
Diagnosing hypertension
Firstly, NICE recommend measuring
blood pressure in both arms when considering a diagnosis of hypertension.
If the difference in readings
between arms is more than 20 mmHg then the measurements should be repeated. If
the difference remains > 20 mmHg then subsequent blood pressures should be
recorded from the arm with the higher reading.
It should of course be remember
that there are pathological causes of unequal blood pressure readings from the
arms, such as supravalvular aortic stenosis. It is therefore prudent to listen
to the heart sounds if a difference exists and further investigation if a very
large difference is noted.
NICE also recommend taking a second
reading during the consultation, if the first reading is > 140/90 mmHg. The
lower reading of the two should determine further management.
NICE suggest offering ABPM or HBPM
to any patient with a blood pressure >= 140/90 mmHg.
If the blood pressure is >=
180/120 mmHg:
·
admit for specialist assessment if:
o signs of retinal haemorrhage or
papilloedema (accelerated hypertension) or
o life-threatening symptoms such as new-onset confusion, chest pain, signs of heart failure, or acute
kidney injury
·
NICE also recommend referral if a phaeochromocytoma is suspected
(labile or postural hypotension, headache, palpitations, pallor and
diaphoresis)
·
if none of the above then arrange urgent
investigations for end-organ damage (e.g. bloods, urine ACR, ECG)
o if target organ damage is
identified, consider starting antihypertensive drug treatment immediately,
without waiting for the results of ABPM or HBPM.
o if no target organ damage is
identified, repeat clinic blood pressure measurement within 7 days
Ambulatory blood pressure
monitoring (ABPM)
·
at least 2 measurements per hour during the person's usual
waking hours (for example, between 08:00 and 22:00)
·
use the average value of at least 14 measurements
If ABPM is not tolerated or
declined HBPM should be offered.
Home blood pressure monitoring
(HBPM)
·
for each BP recording, two consecutive measurements need to be
taken, at least 1 minute apart and with the person seated
·
BP should be recorded twice daily, ideally in the morning and
evening
·
BP should be recorded for at least 4 days, ideally for 7 days
·
discard the measurements taken on the first day and use the
average value of all the remaining measurements
Interpreting the results
ABPM/HBPM >= 135/85 mmHg (i.e.
stage 1 hypertension)
·
treat if < 80 years of age AND any of the following apply;
target organ damage, established cardiovascular disease, renal disease,
diabetes or a 10-year cardiovascular risk equivalent to 10% or greater
·
in 2019, NICE made a further recommendation, suggesting that we
should 'consider antihypertensive drug
treatment in addition to lifestyle advice for adults aged under 60 with stage 1
hypertension and an estimated 10-year risk below 10%. '. This seems to be due to evidence
that QRISK may underestimate the lifetime probability of developing
cardiovascular disease
ABPM/HBPM >= 150/95 mmHg (i.e.
stage 2 hypertension)
·
offer drug treatment regardless of age
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:47
Beta-blockers
Beta-blockers are an important
class of drug used mainly in the management of cardiovascular disorders.
Indications
·
angina
·
post-myocardial infarction
·
heart failure: beta-blockers were previously avoided in heart
failure but there is now strong evidence that certain beta-blockers improve
both symptoms and mortality
·
arrhythmias: beta-blockers have now replaced digoxin as the
rate-control drug of choice in atrial fibrillation
·
hypertension: the role of beta-blockers has diminished in recent
years due to a lack of evidence in terms of reducing stroke and myocardial
infarction.
·
thyrotoxicosis
·
migraine prophylaxis
·
anxiety
Examples
·
atenolol
·
propranolol: one of the first beta-blockers to be developed.
Lipid soluble therefore crosses the blood-brain barrier
Side-effects
·
bronchospasm
·
cold peripheries
·
fatigue
·
sleep disturbances, including nightmares
·
erectile dysfunction
Contraindications
·
uncontrolled heart failure
·
asthma
·
sick sinus syndrome
·
concurrent verapamil use: may precipitate
severe bradycardia
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:48
Peri-arrest rhythms: tachycardia
The 2015 Resuscitation Council (UK)
guidelines have simplified the advice given for the management of peri-arrest
tachycardias. Separate algorithms for the management of broad-complex
tachycardia, narrow complex tachycardia and atrial fibrillation have been
replaced by one unified treatment algorithm
Following basic ABC assessment,
patients are classified as being stable or unstable according to the presence
of any adverse signs:
·
shock: hypotension (systolic
blood pressure < 90 mmHg), pallor, sweating, cold, clammy extremities, confusion or
impaired consciousness
·
syncope
·
myocardial ischaemia
·
heart failure
If any of the above adverse signs are
present then synchronised DC shocks should be given
Treatment following this is given
according to whether the QRS complex is narrow or broad and whether the rhythm
is regular or irregular. The full treatment algorithm can be found at the
Resuscitation Council website, below is a very limited summary:
Broad-complex tachycardia
Regular
·
assume ventricular tachycardia (unless previously confirmed SVT
with bundle branch block)
·
loading dose of amiodarone followed by 24 hour infusion
Irregular
·
1. AF with bundle branch block - treat as for narrow complex
tachycardia
·
2. Polymorphic VT (e.g. Torsade de pointes) - IV magnesium
Narrow-complex tachycardia
Regular
·
vagal manoeuvres followed by IV adenosine
·
if above unsuccessful consider diagnosis of atrial flutter and
control rate (e.g. Beta-blockers)
Irregular
·
probable atrial fibrillation
·
if onset < 48 hr consider electrical or chemical
cardioversion
·
rate control (e.g. Beta-blocker or digoxin) and anticoagulation
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
22:38
Acute coronary syndrome: initial management
Acute coronary syndrome (ACS) is a
very common and important presentation in medicine. The management of ACS has
evolved over recent years, with the development of new drugs and procedures
such as primary coronary intervention (PCI).
Emergency departments often have
their own protocols based around local factors such as availability of PCI and
hospital drug formularies. The following is based around the 2020 update to the
NICE ACS guidelines.
Acute coronary syndrome can be
classified as follows:
·
ST-elevation myocardial infarction (STEMI): ST-segment elevation
+ elevated biomarkers of myocardial damage
·
non ST-elevation myocardial infarction (NSTEMI): ECG changes but
no ST-segment elevation + elevated biomarkers of myocardial damage
·
unstable angina
The management of ACS depends on
the particular subtype. NICE management guidance groups the patients into two
groups:
·
1. STEMI
·
2. NSTEM/unstable angina
Common management of all patients
with ACS
·
aspirin 300mg
·
oxygen should only be given if the patient has oxygen
saturations < 94% in keeping with British Thoracic Society oxygen therapy
guidelines
·
morphine should only be given for patients with severe pain
o previously IV morphine was given
routinely
o evidence, however, suggests that
this may be associated with adverse outcomes
·
nitrates
o can be given either sublingually or
intravenously
o useful if the patient has ongoing
chest or hypertension
o should be used in caution if
patient hypotensive
The next step in managing a patient
with suspected ACS is to determine whether they meet the ECG criteria for
STEMI. It is, of course, important to recognise that these should be
interpreted in the context of the clinical history.
STEMI criteria
·
clinical symptoms consistent with ACS (generally of ≥ 20 minutes
duration) with persistent (> 20 minutes) ECG features in ≥ 2 contiguous
leads of:
o 2.5 mm (i.e ≥ 2.5 small squares) ST
elevation in leads V2-3 in men under 40 years, or ≥ 2.0 mm (i.e ≥ 2 small
squares) ST elevation in leads V2-3 in men over 40 years
o 1.5 mm ST elevation in V2-3 in
women
o 1 mm ST elevation in other leads
o new LBBB (LBBB should be considered
new unless there is evidence otherwise)
Management of STEMI
Once a STEMI has been confirmed the
first step is to immediately assess eligibility for coronary reperfusion
therapy. There are two types of coronary reperfusion therapy:
·
primary coronary intervention
o should be offered if the
presentation is within 12 hours of onset of symptoms AND PCI can be delivered
within 120 minutes of the time when thrombolysis could have been given (i.e. consider
thrombolysis if there is a significant delay in being able to provide PCI)
o if patients present after 12 hours
and still have evidence of ongoing ischaemia then PCI should still be
considered
o drug-eluting stents are now used.
Previously 'bare-metal' stents were sometimes used but have higher rates of
restenosis
o radial access is preferred to
femoral access
·
thrombolysis
o should be offered within 12 hours
of onset of symptoms if primary PCI cannot be delivered within 120 minutes of the time when
thrombolysis could have been given
o a practical example may be a
patient who presents with a STEMI to a small district general hospital (DGH)
which does not have facilities for PCI. If they cannot be transferred to a
larger hospital for PCI within 120 minutes then thrombolysis should be given.
If the patient's ECG taken 90 minutes after thrombolysis failed to show
resolution of the ST elevation then they would then require transfer for PCI
If patients are eligible this
should be offered as soon as possible.
Primary coronary intervention for patients
with STEMI
Further antiplatelet prior to PCI
·
this is termed 'dual antiplatelet therapy', i.e. aspirin +
another drug
·
if the patient is not taking an oral anticoagulant: prasugrel
·
if taking an oral anticoagulant: clopidogrel
Drug therapy during PCI
·
patients undergoing PCI with radial access:
o unfractionated heparin with bailout
glycoprotein IIb/IIIa inhibitor (GPI) - this is the action of using a GPI
during the procedure when it was not intended from the outset, e.g. because of
worsening or persistent thrombus
·
patients undergoing PCI with femoral access:
o bivalirudin with bailout GPI
Other procedures during PCI
·
thrombus aspiration, but not mechanical thrombus extraction,
should be considered
·
complete revascularisation should be considered for patients
with multivessel coronary artery disease without cardiogenic shock
Thrombolysis for patients with
STEMI
Thrombolysis used to be the only
form of coronary reperfusion therapy available. However, it is used much less
commonly now given the widespread availability of PCI.
The contraindications to
thrombolysis and other factors are described in other notes.
Patients undergoing thrombolysis
should also be given an antithrombin drug.
If patients have persistent myocardial ischaemia
following thrombolysis then PCI should be considered.
Management of NSTEMI/unstable
The management of NSTEMI/unstable
is complicated and depends on individual patient factors and a risk assessment. The summary below provides an overview but the full NICE
guidelines should be reviewed for further details.
Further drug therapy
·
antithrombin treatment
o fondaparinux should be offered
to patients who are not at a high risk of bleeding and who are not having
angiography immediately
o if immediate angiography is planned
or a patients creatinine is > 265 µmol/L then unfractionated heparin should
be given
Risk assessment
The Global Registry of Acute
Coronary Events (GRACE) is the most widely used tool for risk assessment. It
can be calculated using online tools and takes into account the following
factors:
·
age
·
heart rate, blood pressure
·
cardiac (Killip class) and renal function (serum creatinine)
·
cardiac arrest on presentation
·
ECG findings
·
troponin levels
This results in the patient being
risk stratified as follows:
|
Predicted
6‑month
mortality |
Risk of future adverse cardiovascular
events |
|
1.5% or below |
Lowest |
|
> 1.5% to 3.0% |
Low |
|
> 3.0% to 6.0% |
Intermediate |
|
> 6.0% to 9.0% |
High |
|
over 9.0% |
Highest |
Based on this risk assessment key decisions are
made regarding whether a patient has coronary angiography
(with follow-on PCI if necessary) or has conservative management. The detailed
pros/cons of this descision are covered in other notes.
Which patients with NSTEMI/unstable
angina should have a coronary angiography (with follow-on PCI if necessary)?
·
immediate: patient who are clinically unstable (e.g.
hypotensive)
·
within 72 hours: patients with a GRACE score > 3% i.e. those at
immediate, high or highest risk
·
coronary angiography should also be considered for patients is
ischaemia is subsequently experienced after admission
Primary coronary intervention for
patients with NSTEMI/unstable angina
Further drug therapy
·
unfractionated heparin should be given regardless of whether the
patient has had fondaparinux or not
·
further antiplatelet ('dual antiplatelet therapy', i.e. aspirin
+ another drug) prior to PCI
o if the patient is not taking an
oral anticoagulant: prasugrel or ticagrelor
o if taking an oral anticoagulant:
clopidogrel
Conservative management for
patients with NSTEMI/unstable angina
Further drug therapy
·
further antiplatelet ('dual antiplatelet therapy', i.e. aspirin
+ another drug)
o if the patient is not at a
high-risk of bleeding: ticagrelor
o if the patient is at a high-risk of
bleeding: clopidogrel
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
17:22
Coarctation of the aorta
Coarctation of the aorta describes
a congenital narrowing of the descending aorta.
Overview
·
more common in males (despite association with Turner's
syndrome)
Features
·
infancy: heart failure
·
adult: hypertension
·
radio-femoral delay
·
mid systolic murmur, maximal over back
·
apical click from the aortic valve
·
notching of the inferior border of the ribs (due to collateral
vessels) is not seen in young children
Associations
·
Turner's syndrome
·
bicuspid aortic valve
·
berry aneurysms
·
neurofibromatosis
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
22:49
Atrial fibrillation: anticoagulation
NICE updated their guidelines on
the management of atrial fibrillation (AF) in 2014. They suggest using the CHA2DS2-VASc score to
determine the most appropriate anticoagulation strategy. This scoring system
superceded the CHADS2 score.
|
|
Risk factor |
Points |
|
C |
Congestive heart failure |
1 |
|
H |
Hypertension (or treated hypertension) |
1 |
|
A2 |
Age >= 75 years |
2 |
|
|
Age 65-74 years |
1 |
|
D |
Diabetes |
1 |
|
S2 |
Prior Stroke or TIA |
2 |
|
V |
Vascular disease (including ischaemic
heart disease and peripheral arterial disease) |
1 |
|
S |
Sex (female) |
1 |
The table below shows a suggested anticoagulation strategy based on
the score:
|
Score |
Anticoagulation |
|
0 |
No treatment |
|
1 |
Males: Consider anticoagulation Females: No treatment (this is because
their score of 1 is only reached due to their gender) |
|
2 or more |
Offer anticoagulation |
Remember that if a CHA2DS2-VASc score
suggests no need for anticoagulation it is important to ensure a transthoracic echocardiogram has
been done to exclude valvular heart disease, which in
combination with AF is an absolute indication for anticoagulation.
NICE recommend that we offer
patients a choice of anticoagulation, including warfarin and the novel oral
anticoagulants (NOACs). There are complicated rules surrounding which NOAC is
licensed for which risk factor - these can be found in the NICE guidelines. Aspirin
is no longer recommended for reducing stroke risk in patients with AF
Doctors have always thought
carefully about the risk/benefit profile of starting someone on warfarin. A
history of falls, old age, alcohol excess and a history of previous bleeding
are common things that make us consider whether warfarinisation is in the best
interests of the patient. NICE now recommend we formalise this risk assessment
using the HASBLED scoring system.
|
|
Risk factor |
Points |
|
H |
Hypertension, uncontrolled, systolic BP
> 160 mmHg |
1 |
|
A |
Abnormal renal function (dialysis or
creatinine > 200) Or Abnormal liver function (cirrhosis,
bilirubin > 2 times normal, ALT/AST/ALP > 3 times normal |
1 for any renal abnormalities 1 for any liver abnormalities |
|
S |
Stroke, history of |
1 |
|
B |
Bleeding, history of bleeding or
tendency to bleed |
1 |
|
L |
Labile INRs (unstable/high INRs, time
in therapeutic range < 60%) |
1 |
|
E |
Elderly (> 65 years) |
1 |
|
D |
Drugs Predisposing to Bleeding
(Antiplatelet agents, NSAIDs) Or Alcohol Use (>8 drinks/week) |
1 for drugs 1 for alcohol |
There are no formal rules on how we
act on the HAS-BLED score although a score of >= 3 indicates a 'high risk'
of bleeding, defined as intracranial haemorrhage, hospitalisation, haemoglobin
decrease >2 g/L, and/or transfusion.
From <https://www.passmedicine.com/question/questions.php?q=0>
For
anyone struggling with remember CHA2DS2-VASc, I find SADCHAVS easier to
remember. The top two in the list are the 2 point scores, and the rest 1.
Stroke
2
Age
>75 2
Diabetes
1
Congestive
Heart Failure 1
HTN
1
Age
>65 1
Vascular
Hx 1
Sex
Female 1
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
18:06
Infective endocarditis
The strongest risk factor for
developing infective endocarditis is a previous episode of endocarditis. The following
types of patients are affected:
·
previously normal valves (50%, typically acute presentation)
o the mitral valve is most commonly
affected
·
rheumatic valve disease (30%)
·
prosthetic valves
·
congenital heart defects
·
intravenous drug users (IVDUs, e.g. typically causing tricuspid lesion)
·
others: recent piercings
Causes
·
historically Streptococcus viridans was the most common cause of
infective endocarditis. This is no longer the case, except in developing
countries. Staphylococcus aureus is
now the most common cause of infective endocarditis. Staphylococcus
aureus is also particularly common in acute presentation and IVDUs
·
coagulase-negative Staphylococci such as Staphylococcus
epidermidis commonly colonize indwelling lines and are the most cause of
endocarditis in patients following prosthetic valve surgery, usually the result
of perioperative contamination. After 2 months the spectrum of organisms which
cause endocarditis return to normal (i.e. Staphylococcus
aureus is the most common cause)
·
Streptococcus viridans still accounts for around 20% of
cases. Technically Streptococcus viridans is a pseudotaxonomic term,
referring to viridans streptococci, rather than a particular organism. The two
most notable viridans streptococci are Streptococcus mitis and Streptococcus
sanguinis. They are both
commonly found in the mouth and in particular dental plaque so endocarditis
caused by these organisms is linked with poor
dental hygiene or following a dental procedure
·
Streptococcus bovis is associated with colorectal cancer
o the subtype Streptococcus
gallolyticus is most linked with colorectal cancer
·
non-infective: systemic lupus erythematosus (Libman-Sacks),
malignancy: marantic endocarditis
Culture negative causes
·
prior antibiotic therapy
·
Coxiella burnetii
·
Bartonella
·
Brucella
·
HACEK: Haemophilus, Actinobacillus,
Cardiobacterium, Eikenella, Kingella)
*Lancet 2016; 387: 882-93 Infective
Endocarditis
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:47
Murmurs
Ejection systolic
·
louder on expiration
o aortic stenosis
o hypertrophic obstructive
cardiomyopathy
·
louder on inspiration
o pulmonary
stenosis
o atrial septal defect
·
also: tetralogy of Fallot
Holosystolic (pansystolic)
·
mitral/tricuspid regurgitation (high-pitched and 'blowing' in
character)
o tricuspid regurgitation becomes
louder during inspiration, unlike mitral stenosis
o during inspiration, the venous
blood flow into the right atrium and ventricle are increased → increases the
stroke volume of the right ventricle during systole
·
ventricular septal defect ('harsh' in character)
Late systolic
·
mitral valve prolapse
·
coarctation of aorta
Early diastolic
·
aortic regurgitation (high-pitched and 'blowing' in
character)
·
Graham-Steel murmur (pulmonary regurgitation, again high-pitched
and 'blowing' in character)
Mid-late diastolic
·
mitral stenosis ('rumbling' in character)
·
Austin-Flint murmur (severe aortic regurgitation, again is
'rumbling' in character)
Continuous machine-like murmur
·
patent ductus arteriosus
|
|
|
|
Image
sourced from Wikipedia |
|

From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
17:38
Supraventricular tachycardia
Whilst strictly speaking the term
supraventricular tachycardia (SVT) refers to any tachycardia that is not
ventricular in origin the term is generally used in the context of paroxysmal
SVT. Episodes are characterised by the sudden onset of a narrow complex
tachycardia, typically an atrioventricular nodal re-entry tachycardia (AVNRT).
Other causes include atrioventricular re-entry tachycardias (AVRT) and
junctional tachycardias.
Acute management
·
vagal manoeuvres: e.g. Valsalva manoeuvre, carotid sinus massage
·
intravenous adenosine 6mg → 12mg → 12mg: contraindicated
in asthmatics - verapamil is a preferable option
·
electrical cardioversion
Prevention of episodes
·
beta-blockers
·
radio-frequency ablation
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
22:04
Syncope
Syncope may be defined as a
transient loss of consciousness due to global cerebral hypoperfusion with rapid
onset, short duration and spontaneous complete recovery. Note how this
definition excludes other causes of collapse such as epilepsy.
The European Society of Cardiology
published guidelines in 2009 on the investigation and management of syncope.
They suggested the following classification:
Reflex syncope (neurally mediated)
·
vasovagal: triggered by emotion, pain or stress. Often referred
to as 'fainting'
·
situational: cough, micturition, gastrointestinal
·
carotid sinus syncope
Orthostatic syncope
·
primary autonomic failure: Parkinson's disease, Lewy body
dementia
·
secondary autonomic failure: e.g. Diabetic neuropathy,
amyloidosis, uraemia
·
drug-induced: diuretics, alcohol, vasodilators
·
volume depletion: haemorrhage, diarrhoea
Cardiac syncope
·
arrhythmias: bradycardias (sinus node dysfunction, AV conduction
disorders) or tachycardias (supraventricular, ventricular)
·
structural: valvular, myocardial infarction, hypertrophic
obstructive cardiomyopathy
·
others: pulmonary embolism
Reflex syncope is the most common
cause in all age groups although orthostatic and cardiac causes become
progressively more common in older patients.
Evaluation
·
cardiovascular examination
·
postural blood pressure readings: a symptomatic fall in systolic
BP > 20 mmHg or diastolic BP > 10 mmHg or decrease in systolic BP < 90
mmHg is considered diagnostic
·
ECG
·
carotid sinus massage
·
tilt table test
·
24 hour ECG
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
16:25
Atrial fibrillation: cardioversion
There are two scenarios where
cardioversion may be used in atrial fibrillation:
·
electrical cardioversion as an emergency if the patient is haemodynamically unstable
·
electrical or pharmacological cardioversion as an elective
procedure where a rhythm control strategy is preferred.
The notes below refer to
cardioversion being used in the elective scenario for rhythm control. The
wording of the 2014 NICE guidelines is as follows:
offer rate or rhythm control if the onset of the
arrhythmia is less than 48 hours, and start rate control if it is more than 48
hours or is uncertain
Onset < 48 hours
If the atrial fibrillation (AF) is
definitely of less
than 48 hours onset patients should be
heparinised. Patients who have risk factors for ischaemic stroke should be put
on lifelong oral anticoagulation. Otherwise, patients may be cardioverted using
either:
·
electrical - 'DC cardioversion'
·
pharmacology - amiodarone if structural heart disease,
flecainide or amiodarone in those without structural heart disease
Following electrical cardioversion
if AF is confirmed as being less than 48 hours duration then further
anticoagulation is unnecessary
Onset > 48 hours
If the patient has been in AF for
more than 48 hours then anticoagulation should be given for at least 3 weeks
prior to cardioversion. An alternative strategy is to perform a
transoesophageal echo (TOE) to exclude a left atrial appendage (LAA) thrombus.
If excluded patients may be heparinised and cardioverted immediately.
NICE recommend electrical
cardioversion in this scenario, rather than pharmacological.
If there is a high risk of
cardioversion failure (e.g. Previous failure or AF recurrence) then it is
recommend to have at least 4 weeks amiodarone or sotalol prior to electrical
cardioversion
Following electrical cardioversion
patients should be anticoagulated for at least 4 weeks. After this time
decisions about anticoagulation should be taken on an individual basis depending
on the risk of recurrence
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
16:20
Cardiac tamponade
Cardiac tamponade is characterized
by the accumulation of pericardial fluid under pressure.
Classical features - Beck's triad:
·
hypotension
·
raised JVP
·
muffled heart sounds
Other features:
·
dyspnoea
·
tachycardia
·
an absent Y descent on the JVP - this is due to the limited
right ventricular filling
·
pulsus paradoxus - an abnormally large drop in BP during inspiration
·
Kussmaul's sign - much debate about this
·
ECG: electrical alternans
The key differences between
constrictive pericarditis and cardiac tamponade are summarised in the table
below:
|
|
Cardiac tamponade |
Constrictive pericarditis |
|
JVP |
Absent Y descent |
X + Y present |
|
Pulsus paradoxus |
Present |
Absent |
|
Kussmaul's sign |
Rare |
Present |
|
Characteristic features |
|
Pericardial calcification on CXR |
A commonly used mnemonic to
remember the absent Y descent in cardiac tamponade is TAMponade = TAMpaX
Management
·
urgent pericardiocentesis
|
|
|
|
©
Image used on license from Dr Smith, University of Minnesota |
|
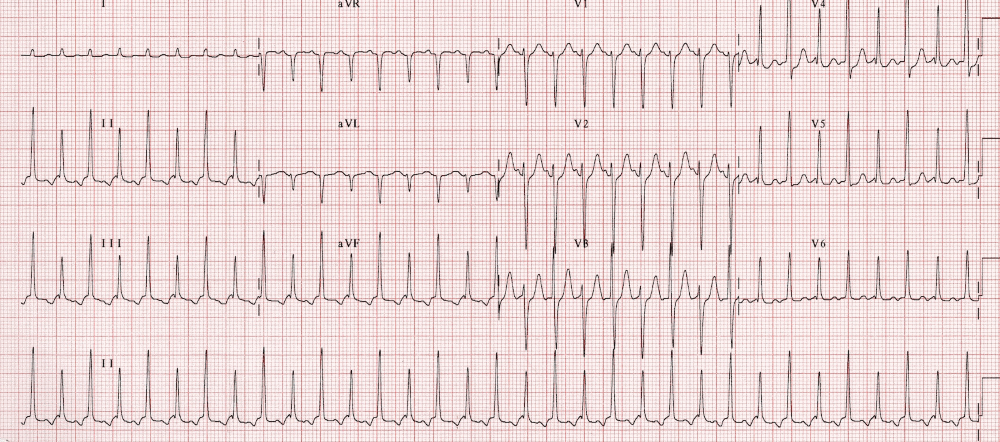
An ECG demonstrating electrical alternans. Note the
alternation of QRS complex amplitude between beats.
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
22:46
Diabetes mellitus: hypertension management
Patient diabetes mellitus have
traditionally had their blood pressure controlled more aggressively to help
reduce their overall cardiovascular risk. However, a 2013 Cochrane review
casted doubt on the wisdom of lower blood pressure targets for patients with
diabetes. It compared patients who had tight blood pressure
control (targets < 130/85 mmHg) with more relaxed control (<
140-160/90-100 mmHg). Patients who were more tightly controlled had a slightly
reduced rate of stroke but otherwise outcomes were not significantly different.
In light of this, NICE recommends a blood
pressure target of < 140/90 mmHg for type 2 diabetics, the same as for patients without diabetes.
For patients with type 1 diabetes,
NICE recommends:
Intervention levels for recommending blood pressure
management should be 135/85
mmHg unless the adult with type 1
diabetes has albuminuria or 2 or more features of metabolic syndrome, in which
case it should be 130/80 mmHg
Because ACE-inhibitors have a renoprotective effect in diabetes they are the first-line
antihypertensives recommended for NICE. Patients of African or Caribbean family origin should be offered an ACE-inhibitor plus
either a thiazide diuretic or calcium channel blocker. Further management then
reverts to that of non-diabetic patients, as discussed earlier in the module.
Remember than autonomic neuropathy
may result in more postural symptoms in patients taking antihypertensive
therapy.
The routine use of beta-blockers in
uncomplicated hypertension should be avoided, particularly when given in
combination with thiazides, as they may cause insulin resistance, impair
insulin secretion and alter the autonomic response to hypoglycaemia.
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
21:47
Myocardial infarction: STEMI management
A number of studies over the past
10 years have provided an evidence for the management of ST-elevation
myocardial infarction (STEMI)
In the absence of
contraindications, all patients should be given
·
aspirin
·
P2Y12-receptor antagonist. Clopidogrel was the first P2Y12-receptor antagonist to
be widely used but now ticagrelor is often favoured as studies have shown
improved outcomes compared to clopidogrel, but at the expense of slightly
higher rates of bleeding. This approached is supported in SIGN's 2016 guidelines.
They also recommend that prasugrel (another P2Y12-receptor antagonist) could be
considered if the patient is going to have a percutaneous coronary intervention
·
unfractionated heparin is usually given for patients
who're are going to have a PCI. Alternatives include low-molecular weight
heparin
NICE suggest the following in terms
of oxygen therapy:
·
do not routinely administer oxygen, but monitor oxygen
saturation using pulse oximetry as soon as possible, ideally before hospital
admission. Only offer supplemental oxygen to:
·
people with oxygen saturation (SpO2) of less than 94% who are
not at risk of hypercapnic respiratory failure, aiming for SpO2 of 94-98%
·
people with chronic obstructive pulmonary disease who are at
risk of hypercapnic respiratory failure, to achieve a target SpO2 of 88-92%
until blood gas analysis is available.
Primary
percutaneous coronary intervention (PCI) has emerged as the gold-standard
treatment for STEMI but is not available in all centres. Thrombolysis should be
performed in patients without access to primary PCI
With regards to thrombolysis:
·
tissue plasminogen activator (tPA) has been shown to offer clear
mortality benefits over streptokinase
·
tenecteplase is easier to administer and has been shown to have
non-inferior efficacy to alteplase with a similar adverse effect profile
An ECG should be performed 90
minutes following thrombolysis to assess whether there has been a greater than
50% resolution in the ST elevation
·
if there has not been adequate resolution then rescue PCI is
superior to repeat thrombolysis
·
for patients successfully treated with thrombolysis PCI has been
shown to be beneficial. The optimal timing of this is still under investigation
Glycaemic control in patients with
diabetes mellitus
·
in 2011 NICE issued guidance on the management of hyperglycaemia
in acute coronary syndromes
·
it recommends using a dose-adjusted insulin infusion with
regular monitoring of blood glucose levels to glucose below 11.0 mmol/l
·
intensive insulin therapy (an intravenous infusion of insulin
and glucose with or without potassium, sometimes referred to as 'DIGAMI')
regimes are not recommended routinely
From <https://www.passmedicine.com/review/textbook.php?s=#>
21 December 2020
21:47
Aortic dissection
Aortic dissection is a rare but
serious cause of chest pain.
Pathophysiology
·
tear in the tunica intima of the wall of the aorta
Associations
·
hypertension: the most important risk factor
·
trauma
·
bicuspid aortic valve
·
collagens: Marfan's syndrome, Ehlers-Danlos syndrome
·
Turner's and Noonan's syndrome
·
pregnancy
·
syphilis
Features:
·
chest pain: typically severe, radiates through to the back and
'tearing' in nature
·
aortic regurgitation
·
hypertension
·
other features may result from the involvement of specific
arteries. For example coronary arteries → angina, spinal arteries → paraplegia, distal aorta → limb ischaemia
·
the majority of patients have no or non-specific ECG changes. In
a minority of patients, ST-segment elevation may be seen
in the inferior leads
Classification
Stanford classification
·
type A - ascending aorta, 2/3 of cases
·
type B - descending aorta, distal to left subclavian origin, 1/3
of cases
DeBakey classification
·
type I - originates in ascending aorta, propagates to at least
the aortic arch and possibly beyond it distally
·
type II - originates in and is confined to the ascending aorta
·
type III - originates in descending aorta, rarely extends
proximally but will extend distally
|
|
|
|
©
Image used on license from Radiopaedia |
|

Stanford type A / DeBakey type I
|
|
|
|
©
Image used on license from Radiopaedia |
|

Stanford type A / DeBakey type II
|
|
|
|
©
Image used on license from Radiopaedia |
|

Stanford type B / DeBakey type III
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
17:03
Atrial flutter
Atrial flutter is a form of
supraventricular tachycardia characterised by a succession of rapid atrial
depolarisation waves.
ECG findings
·
'sawtooth' appearance
·
as the underlying atrial rate is often around 300/min the
ventricular or heart rate is dependent on the degree of AV block. For example
if there is 2:1 block the ventricular rate will be 150/min
·
flutter waves may be visible following carotid sinus massage or
adenosine
Management
·
is similar to that of atrial fibrillation although medication
may be less effective
·
atrial flutter is more sensitive to cardioversion however so
lower energy levels may be used
·
radiofrequency ablation of the tricuspid valve isthmus is
curative for most patients
Next question
Save my notes
Search
Go
Google search on
"Atrial flutter"
Links
|
Life
in the Fast Lane |
20 |
|
|
Suggest linkReport broken link
Media
|
|
|
|
|
|
|
Osmosis
- YouTube |
22 |

From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
22:54
Mitral stenosis
It is said that the causes of
mitral stenosis are rheumatic fever,
rheumatic fever and rheumatic fever. Rarer causes that may be seen in
the exam include mucopolysaccharidoses, carcinoid and endocardial
fibroelastosis
Features
·
mid-late diastolic murmur (best heard in expiration)
·
loud S1, opening snap
·
low volume pulse
·
malar flush
·
atrial fibrillation
Features of severe MS
·
length of murmur increases
·
opening snap becomes closer to S2
Chest x-ray
·
left atrial enlargement may be seen
Echocardiography
·
the normal cross sectional area of the mitral valve is 4-6 sq
cm. A 'tight' mitral stenosis implies a cross sectional area of < 1 sq cm
|
|
|
|
©
Image used on license from Radiopaedia |
|
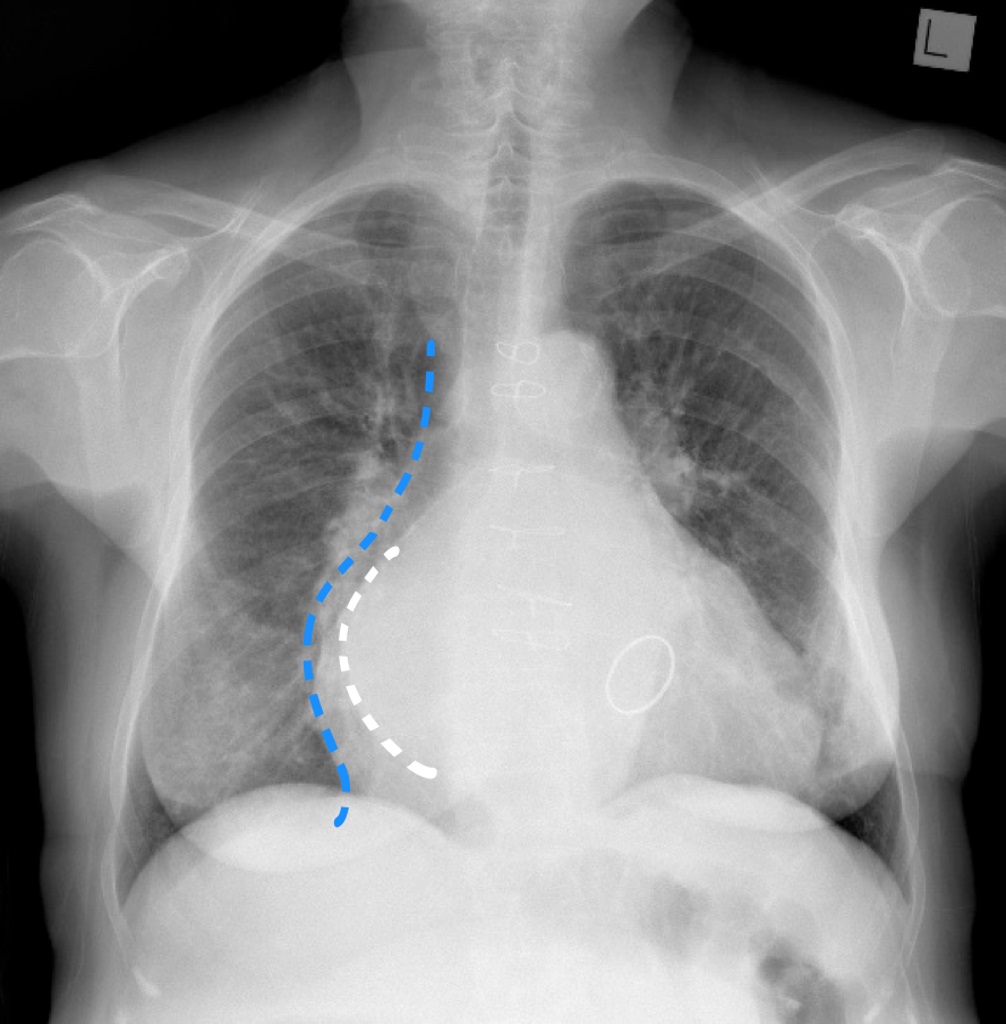
{kind=link}
Chest x-ray from a patient with mitral stenosis. This
patient has had a sternotomy and a prosthetic mitral valve. There is splaying
of the carina with elevation of the left main bronchus, a double right heart
border and cardiomegaly. The features are those of left atrial enlargement.
Although the entire heart is enlarged, a double contour is seen through the
right side of the heart. The more medial line is the enlarged left atrium
(white dotted line) and the heart heart border is more lateral (blue dotted
line).
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
16:31
Cardiomyopathies: key points
The old classification of dilated,
restricted and hypertrophic cardiomyopathy has been largely abandoned due to
the high degree of overlap. The latest classification of cardiomyopathy by the
WHO and American Heart Association reflect this.
The tables below shows a very
limited set of exam related facts for the various cardiomyopathies:
Primary cardiomyopathies -
predominately involving the heart
Genetic - both
conditions listed below are autosomal dominant. An implantable
cardioverter-defibrillator is often inserted to reduce the incidence of sudden
cardiac death.
|
Type
of cardiomyopathy |
Selected points |
|
Hypertrophic obstructive cardiomyopathy |
Leading cause of sudden cardiac death
in young athletes Usually due to a mutation in the gene
encoding β-myosin heavy chain protein Common cause of sudden death Echo findings include MR, systolic
anterior motion (SAM) of the anterior mitral valve and asymmetric septal
hypertrophy |
|
Arrhythmogenic right ventricular
dysplasia |
Right ventricular
myocardium is replaced by fatty and fibrofatty tissue Around 50% of patients have a mutation
of one of the several genes which encode components of desmosome ECG abnormalities in V1-3, typically T
wave inversion. An epsilon wave is
found in about 50% of those with ARV - this is best described as a terminal
notch in the QRS complex |
Mixed - rather
confusingly most of the causes of dilated and restrictive cardiomyopathy are
now listed separately in the 'secondary' causes. This category servers as a
reminder that many patients will have a genetic predisposition to
cardiomyopathy which is then triggered by the secondary process, hence the
'mixed' category
|
Type
of cardiomyopathy |
Selected causes/points |
|
Dilated cardiomyopathy |
Classic causes include ·
alcohol ·
Coxsackie B virus ·
wet beri beri ·
doxorubicin |
|
Restrictive cardiomyopathy |
Classic causes include ·
amyloidosis ·
post-radiotherapy ·
Loeffler's endocarditis |
Familial
restrictive cardiomyopathy demonstrates autosomal dominant inheritance in the
majority of cases.
Acquired
|
Type
of cardiomyopathy |
Selected points |
|
Peripartum cardiomyopathy |
Typical develops between last month of
pregnancy and 5 months post-partum More common in older women, greater
parity and multiple gestations |
|
Takotsubo cardiomyopathy |
'Stress'-induced cardiomyopathy e.g.
patient just found out family member dies then develops chest pain and
features of heart failure Transient, apical ballooning of the
myocardium Treatment is supportive |
Secondary cardiomyopathies- pathological myocardial involvement as part of a generalized
systemic disorder
|
Type
of cardiomyopathy |
Selected causes/points |
|
Infective |
Coxsackie B virus Chagas disease |
|
Infiltrative |
Amyloidosis |
|
Storage |
Haemochromatosis |
|
Toxicity |
Doxorubicin Alcoholic cardiomyopathy |
|
Inflammatory (granulomatous) |
Sarcoidosis |
|
Endocrine |
Diabetes mellitus Thyrotoxicosis Acromegaly |
|
Neuromuscular |
Friedreich's ataxia Duchenne-Becker muscular dystrophy Myotonic dystrophy |
|
Nutritional deficiencies |
Beriberi (thiamine) |
|
Autoimmune |
Systemic lupus erythematosis |
From <https://www.passmedicine.com/question/questions.php?q=0>
Arrhythmogenic
right ventricular cardiomyopathy is characterised by right ventricular
myocardium replacement by fatty and fibrofatty tissue.
Arrhythmogenic
right ventricular cardiomyopathy in late stages may cause dilation of the
ventricles but not initially.
From <https://mle.ncl.ac.uk/cases/page/18128/>
Progressive
deterioration of AV block risk is high in myotonic muscular dystrophy.
Permanent
pacemaker for AV block first degree
From <https://mle.ncl.ac.uk/cases/page/18128/>
Reversible cardiomyopathies: (not
exhaustive)
Viral myocarditis
PVC-induced cardiomyopathy
Tachycardia cardiomyopathy
Alcohol cardiomyopathy
24 December 2020
13:09
ECG: ST elevation
Causes of ST elevation
·
myocardial infarction
·
pericarditis/myocarditis
·
normal variant - 'high take-off'
·
left ventricular aneurysm
·
Prinzmetal's angina (coronary artery spasm)
·
Takotsubo cardiomyopathy
·
rare: subarachnoid haemorrhage
From <https://www.passmedicine.com/review/textbook.php?s=#>
22 December 2020
17:25
ECG: P wave changes
Increased P wave amplitude
·
cor pulmonale
From <https://www.passmedicine.com/question/questions.php?q=0>
21 December 2020
22:35
ECG: T wave changes
Peaked T waves
·
hyperkalaemia
·
myocardial ischaemia
Inverted T waves
·
myocardial ischaemia
·
digoxin toxicity
·
subarachnoid haemorrhage
·
arrhythmogenic right ventricular cardiomyopathy
·
pulmonary embolism ('S1Q3T3')
·
Brugada syndrome
From <https://www.passmedicine.com/question/questions.php?q=0>
22 December 2020
17:13


Endothelin
receptor antagonists
28 December 2020
22:03
Endothelin
receptor antagonists decrease pulmonary vascular resistance. The aim of
endothelin receptor antagonist therapy is to reduce pulmonary vascular
resistance and hence reduce the strain on the right-sided cardiac
chambers. Right ventricular failure is the commonest cause of death in
primary pulmonary hypertension.
From <https://mle.ncl.ac.uk/cases/page/18128/>
Catecholaminergic
polymorphic ventricular
28 December 2020
22:02
HOCM is the most common cause of
sudden cardiac death in young people.
Catecholaminergic
polymorphic ventricular
Inherited cardiac disease
associated with sudden cardiac death
autosomal dominant with prevalence of
1:10,000.
Brugada
More common in South East Asia.
Sodium channelopathy.
Arrhythmogenic right
ventricular dysplasia
Fibro fatty infiltration of right
ventricle. Cause of sudden death
Long QT
Inherited and acquired. Family
history with inherited form. Usually
preceded by history of recurrent
syncopes. Severe forms may cause sudden
deaths.
Prostacyclins
28 December 2020
22:05
Prostacyclins
are used in the treatment of primary pulmonary hypertension.
Hydrochlorothiazide
is not used to treat PAH but may be used for heart failure and systemic
hypertension.
Aspirin
does not affect PAH.
Lisinopril
and carvedilol are first line drugs for heart failure treatment.
From <https://mle.ncl.ac.uk/cases/page/18128/>
occupational
asthma
28 December 2020
22:14
Industrial
chemicals like isocyanates are the most common cause of occupational asthma.
From <https://mle.ncl.ac.uk/cases/page/18128/>
ICD implantation
28 December 2020
23:05

Obesity venous
insufficiency
28 December 2020
23:08
Exertional
dyspnoea walking up an incline is likely due to morbid obesity.
diurnal variation to his ankle swelling, worse
at night compared to morning plus venous varicosities, probably secondary
to obesity.
From <https://mle.ncl.ac.uk/cases/page/18128/>
Mitochrondrial
cardiomyopathy
28 December 2020
23:13
Retinitis pigmentosa may be
present
Maternal inheritance
Nuclear genes coding
mitochondrial proteins may be mutated
Neuromuscular manifestations are
often apparent
Diastolic dysfunction in
hypertrophic cardiomyopathy
28 December 2020
23:14
Cause:
Increased LV stiffness
Impairment of ventricular
relaxation
Compromised myocardial energy
metabolism
Impairment of coronary blood flow
Sudden cardiac death with
HCM
28 December 2020
23:15
Associations:
·
Unexplained syncope
·
History of premature SCD in a first-degree relative
with hypertrophic cardiomyopathy
·
Non-sustained ventricular tachycardia on Holter
·
Previous history of cardiac arrest
Pulmonary hypertension
Classification
28 December 2020
15:57
Defined as mean pulmonary artery pressure (mPAP) ≥ 20mmHg at rest (measured by right heart catheterisation)
Considered severe when:
·
mPAP ≥35 mmHg
·
mPAP ≥20 mmHg + elevated right atrial
pressure
+/-
cardiac index <2L/min/m2
Cardiac index-
·
More accurate picture of heart function
relative to individual body size
·
Cardiac index (L/min/m2)
·
![]()
·
Normal range 2.5-4.0 L/min/m2
·
Minimum cardiac index of 2.0 L/ min/ m2
required to maintain life without mechanical support
Risk factors-
·
Family history of pulmonary arterial
hypertension
·
Congenital heart disease
·
Connective tissue disease (systemic
sclerosis, SLE)
·
Drugs and toxins
·
Aminorex, Methamphetamine, Fenfluramine
o
Aminorex =a type of SSRI, stimulates
weight loss
o
Fenfluramine= appetite suppressant
·
Human Immunodeficiency Virus (HIV)
·
Mechanism not known
·
Portal hypertension
Clinical classifications-
Group 1: Pulmonary Arterial Hypertension (PAH) with Pulmonary
Artery Occlusion Pressure <15mmHg
·
Idiopathic PAH
·
Hereditary PAH
·
Drug and toxin-induced PAH
PAH associated with
·
Connective tissue disease
·
HIV infection
·
Portal hypertension
·
Congenital Heart Disease
·
Schistosomiasis
Group 2: Pulmonary Hypertension due to left heart
disease
·
Heart failure with preserved ejection
fraction
·
Heart failure with reduced ejection
fraction
·
Valvular heart diseases
Group 3: Pulmonary Hypertension due to lung diseases/
hypoxia
·
Obstructive lung disease
·
Restrictive lung disease
·
Other lung disease with mixed restrictive/
obstructive pattern
·
Developmental lung disorders
Group 4: Pulmonary Hypertension due to pulmonary
artery obstructions
·
Chronic thromboembolic pulmonary
hypertension (CTEPH)
·
Other pulmonary artery obstructions
Group 5: Pulmonary Hypertension with unclear/
multifactorial mechanism
·
Systemic and metabolic disorders
·
Others
·
Complex congenital heart diseases
Investigation:
Gold standard: cardiac
catheterisation.
Right heart pressure
measurements are required via cardiac catheterisation.
Management:
Pulmonary arterial hypertension patients with negative response to
vasodilator testing may be treated with prostacyclin analogues, endothelin
receptor antagonists or phosphodiesterase
inhibitors. Combination therapy is often necessary.
Pulmonary arterial
hypertension patients with positive response to vasodilator testing are
treated with calcium channel blockers e.g. nifedipine, felodipine.
Prostacyclin analogues
Iloprost, epoprostenol
Endothelin receptor antagonists
(sentans)
Bosentan, ambrisentan
Phosphodiesterase inhibitor (afils)
Sildenafil, tadalafil, vardenafil
Pulmonary Arterial
Hypertension (PAH)
29 December 2020
00:05
Problem comes from pulmonary artery
BMPR2 gene
Can be genetically passed on
Female sex important factor
Risk factors-
Collagen vascular disease
Congenital heart disease
Portal hypertension
HIV infection
Drugs and toxins
Pregnancy
Susceptibility- Abnormal
BMPR2 gene + other genetic factors
Vascular injury-
Endothelial dysfunction- reduced
nitric oxide synthase, reduced prostacyclin
production, increased thromboxane
production, increased endothelin 1
production
Vascular smooth muscle dysfunction- impaired
voltage-gated potassium channel
Disease progression- loss of
response to short acting vasodilator trial
![Genetics and Genomics of PAH
The most common genetic mutations in familial PAH and IPAH are in
BMPR2 and its sequence variants (SMADI, SMAD4, SMAD9)
Highly expressed in pulmonary vascular endothelium and forms complexes
with ALKI or ALK2 receptors
Female sex is an important factor in penetrance of BMPR2 mutations
Nearly 25% to 30% of patients diagnosed with IPAH should be re-
classified as having HPAH
Genetic testing can explain etiology and stratify risk for family
members and future children
HPAH Genes Identified Through Whole Genome Sequencing
Higher level
BMPR2; EIF2AK4; TBX4; ATP13A3; GDF2; SOX17;
Of evidence (with causal
AQPI,• ACVRLI; SMAD9,• ENG; KCNK3; CAVI
role in disease)
Lower level
SMAD4; SMADI; KLF2; BMPRIB; KCNA5
of evidence
Morrell NW, et al. Eur RespirJ. 2018. [Epub ahead of print].](file:///C:/Users/henry/AppData/Local/Temp/msohtmlclip1/01/clip_image500.jpg)


Idiopathic
Pulmonary Arterial Hypertension
29 December 2020
12:18
·
Most common among group 1 PAH
·
Female : Male = >3:1
·
No known triggering factor
·
Not associated with family history of PAH
·
Pathology mainly in distal arteries
·
Hypertrophy of tunica media
·
Proliferation and fibrotic changes
in tunica intima
·
Thickened tunica adventitia with perivascular
infiltrates, as well as complex and thrombotic lesions
·
Pulmonary veins unaffected
Hereditary
Pulmonary Arterial Hypertension
29 December 2020
12:18
·
6-10% patients with PH
·
Female > Male
·
Autosomal dominance inheritance with
incomplete penetrance
·
20% carriers will develop disease
·
BMPR2
·
1st PAH-predisposing gene
·
Regulates growth, differentiation and
apoptosis of pulmonary artery endothelial and smooth muscle cells
·
Associated with KCNK3 channelopathy
BMPR2 gene
·
Most commonly associated genetic mutation
in hereditary PAH
·
Highly expressed in pulmonary vascular
endothelium
·
Forms complexes with ALK1/ ALK2 receptors
·
Female sex important factor in penetrance
of BMPR2 mutations
Pulmonary
Hypertension due to left heart diseases
29 December 2020
12:27
Problems come from left side of
the heart

Most common cause of Pulmonary
hypertension
Backward transmission of Left
Arterial pressure to the pulmonary vasculature leads to pulmonary vascular
resistance (PVH)
Enlarged and thickened pulmonary
veins, pulmonary capillary dilation
Alveolar hemorrhage, lymphatic
and lymph node enlargement
Distal arteries may be affected
by medial hypertrophy and intimal fibrosis
Trans pulmonary gradient
mPAP-PAWP= <12mmHg
Primary or pathognomic vascular
changes in arterial wall may be present
Pulmonary Hypertension due
to lung disorders
29 December 2020
15:34
Problems come from the lungs
Chronic inflammation causing
alveolar hypoxic + loss of capillaries d/t due to emphysema
Mechanical injury due to
hyperinflation
Muscularization of small
resistance vessels

Chronic Thromboembolic
Pulmonary hypertension CTEPH
29 December 2020
15:55

Definition is based on findings
described after 3 months of effective anti-coagulation to discriminate from
acute
Pre-capillary PH and at least one
segmental perfusion defect detected by V/Q scan, MDCT angiography, or Pulmonary
angiography
Due to obstruction of major
Pulmonary Artery by Pulmonary embolism which can be symptomatic or
asymptomatic, acute or chronic
Pulmonary Arterial
hypertension due to Multifactorial causes
29 December 2020
15:58

Chronic Haemolytic anaemia
Myeloproliferative disorders
Splenectomy
Sarcoidosis
Pulmonary LCH Langerhans cell
histiocytosis
NF1
Gaucher's disease
Tumoral obstruction of Pulmonary
Artery
CRF chronic renal failure?

Pulmonary Arterial Hypertension
with Connective Tissue Disease
Maximum in Scleroderma patients
Long duration of disease > 8
years
Limited scleroderma> diffuse scleroderma
8-12% prevalence
Poor prognosis
Patient with limited scleroderma
have the risk of developing progressive blood vessel narrowing in the lungs
frequently in the absence of lung scarring and inflammation
Low DLCO<55% predicted -
Diffusing Capacity for Carbon Monoxide
Forced Vital Capacity FVC%/ DLCO% >1.6
Anti-centromere
Antinuclear pattern
on ANA
High resolution CT findings in
scleroderma
Scarring and inflammation of
lungs (ILD)- both diffuse and limited scleroderma
Lungs have no scar but larger
blood vessels are dilated, typical of pulmonary arterial hypertension which is
seen mainly in limited scleroderma
Pulmonary Arterial
Hypertension - Portal hypertension
29 December 2020
16:08

6% of patients with Portal
hypertension develop Pulmonary Arterial Hypertension
Problem for liver transplantation
as PAH increases mortality during and after surgery
Poor prognosis as 3 year survival
is only 40%
Females, autoimmune hepatitis
have increased risk while HCV (Hep C virus) has decreased risk
Independent of the cause of the
portal hypertension
Severity of underlying liver
disease does not correlate with the severity of PAH
Hyperdynamic circulation and high
CO lead to increased shear stress on Pulmonary Circulation
The histological abnormalities
are similar to Idiopathic PAH
Portosystemic shunts may allow
the shunting of ET-1, VIP, 5HT, TXA2, IL1 and escape metabolism
Pulmonary arterial
hypertension associated with Congenital heart disease
29 December 2020
16:13


Pulmonary Veno-Occlusive
Disease
29 December 2020
17:00
Most devastating form of PH
Median survival 84 fays
71% dead in 6 months
10% of PHs are PVOD
Luminal narrowing and occlusion
of pulmonary veins
Difficult to distinguish from PH
-profound hypoxia at rest
-CT chest: septal thickening and
ground glass
Vasodilators NOT used due to
pulmonary oedema risk
LUNG TRANSPLANTATION management
Rare disease
Characterized pathologically by
evidence of repeated pulmonary venous thrombosis
The characteristic histologic
feature of pulmonary veno-occlusive disease is obstruction of pulmonary venules
and veins by intima fibrosis; intravascular fibrous septa are nearly always
present
Etiology of disease is unknown
Drugs given in IPAH is
contraindicated here
Pulmonary oedema after giving PAH
therapy is 1st clue

Pulmonary Hypertension
symptoms
29 December 2020
17:12
Shortness of breath
Chest pain
Dizziness
Syncope
Fatigue
Oedema
Dry cough
Raynaud’s phenomenon (associated
with CTDs) (connective tissue diseases)
Skin- Telangiectasias, Raynaud’s
phenomena, Sclerodactyly (when associated with CTD)
Increased jugular venous pressure
(JVP)
Hepatojugular reflux
Peripheral oedema +/- ascites
Heart sounds:
Accentuated split S2
Third heart sound present
Tricuspid regurgitation- heard
best at left lower sternal border

Pulmonary Arterial
Hypertension Screening, Investigation, Diagnosis and Assessment
29 December 2020
17:43

ECG screening- electrocardiogram
not recommended
RV strain may show
Prognostic information
Right heart disease
May show right axis deviation
Insufficiently
sensitive as a screening tool
Echocardiography
screening- RV enlargement, decreased LV
capacity size, abnormal septal configuration consistent with RV overload,
marked dependence on atrial systole for ventricular filling
Right heart
catheterization is MANDATORY to confirm and characterize disease
PAH is defined by
·
mPAP >25mmHg at rest
·
mPAP >30mmHg with exercise
·
PCWP <15mmHg (Pulmonary Capillary Wedge Pressure=
indirectly measure left atrial pressure)
·
PVR >3 units (Pulmonary vascular resistance)
o
Cardiac output is required to calculate PVR
Screening with CX-ray
Large central pulmonary arteries
Peripheral pruning
Enlarged right heart
Asymptomatic patients may have
normal chest xray
May reveal underlying cause of PH
Ventilation perfusion
lung scan- check perfusion defects
CTEPH- pulmonary angiography
Chronic thromboembolic pulmonary
hypertension
Assess thrombus accessibility
Confirm diagnosis
Angiographic patterns- Web
narrowing, post stenotic dilatation, proximal occlusion, pouch defects
cMRI-
Access RV morphology and function
RV systolic and diastolic
dysfunction- poor prognostic indicator





Management of
Pulmonary Hypertension
29 December 2020
17:54

Acute Vasoreactivity test-
idiopathic, Hereditary, Drug induced
Vasoactive- CCB therapy, Calcium
channel blocker
Non vasoactive
Low risk- oral monotherapy/ combo
therapy
High risk- combo therapy
including IV PC
Inadequate response=
double/triple sequential therapy
Lung transplant
Therapy for PAH
Low level graded aerobic exercise-
not heavy exertion, may provoke syncope
Oxygen supplementation
Sodium restricted diet
Routine immunization- influenza
and pneumococcal pneumonia
Nitric oxide-
Inhaled form
Acts as direct smooth muscle
relaxant via activation of guanylate cyclase system
Short therapeutic half-life
Ameliorates hypoxemia and lowers
PVR by direct pulmonary vasodilatation
Specific measure for Idiopathic
PAH-
Long term anticoagulation with
warfarin 1.5.2.5 inr
Pulmonary vasodilators- calcium
channel blockers, prostacyclin, nitric oxide pathway (PD5 inhib, ER
antagonists)
Prostacyclin analogues
Iloprost, epoprostenol
Endothelin receptor
antagonists (sentans)
Bosentan, ambrisentan
Phosphodiesterase inhibitor
(afils)
Sildenafil, tadalafil, vardenafil


Non-vasoreactive patients-
Depends on WHO functional class
Class I
PAH specific agent e.g. PDE5I
Class II or III
Dual therapy e.g. endothelin receptor antagonist plus a PDE5I
Class IV
Combination therapy to include a parenteral prostainoid e.g. iv
epoprostenol
(alternatives: iv, sub-cut or inhaled treprostinil,
inhaled
iloprost)
Lung transplant
indications-
New York Heart Association (NYHA)
functional class III
or IV
Mean right atrial pressure
>10mmHg
Mean pulmonary arterial pressure >50 mmHg
Failure to improve functionally
despite medical therapy
Rapidly progressive disease

Cardiomyopathy Causes
29 December 2020
18:08
Morphologically
and functionally abnormal myocardium
·
In absence of any other
diseases sufficient to explain the observed phenotype
Divided
into Primary and Secondary Cardiomyopathy
Primary-
·
Pathology predominantly involves the
heart
·
Examples:
·
Dilated cardiomyopathy
·
Hypertrophic cardiomyopathy
·
Restrictive cardiomyopathy
·
Arrhythmogenic right ventricular
cardiomyopathy
·
Obliterative cardiomyopathy
Secondary-


Dilated Cardiomyopathy
29 December 2020
18:19
systolic dysfunction +
ventricular dilation

Autosomal Dominant inheritance
1:2500 prevalence
Presentation:
Heart failure
Cardiac arrythmia
Thromboembolism
Sudden death- family history
obtained
Conduction defects
Investigations:
Bedside ECG
-nonspecific ST segment and T
wave changes
-Sinus tachycardia
-Arrhythmias
·
Atrial Fibrillation, Ventricular tachycardia
Imaging
CXR- generalized cardiac
enlargement
Echocardiogram
-LV +/- RV dilation
Decreased ventricular wall
motility
Tricuspid and mitral valve
insufficiency (Doppler)
Poor global function
Cardiac MRI
Coronary angiography- to exclude
coronary artery disease
Endomyocardial Biopsy
indications-
Acute dilated cardiomyopathy +
refractory heart failure symptoms
Dilated cardiomyopathy in
presence of systemic diseases- SLE Polymyositis, sarcoidosis
Rapidly progressive ventricular
dysfunction
-in unexplained, recent onset
cardiomyopathy
New onset cardiomyopathy +
recurrent VT/high grade heart block
Heart failure in setting of
fever, rash, and peripheral eosinophilia

Management
Manage symptoms of cardiac
failure
Implantable Cardioverter
Defibrillator (ICD)
Cardiac transplant
Hypertrophic Cardiomyopathy
29 December 2020
19:00









Created with OneNote.